

- Department of Neurosurgery, Liaquat National Hospital and Medical College, Karachi, Pakistan.
Correspondence Address:
Muhammad Yassar Jazaib Ali, Department of Neurosurgery, Liaquat National Hospital and Medical College, Karachi, Pakistan.
DOI:10.25259/SNI_504_2023
Copyright: © 2023 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Muhammad Yassar Jazaib Ali, Manzar Hussain. Case of lumbar spinal stenosis and chronic tophaceous gout. 18-Aug-2023;14:294
How to cite this URL: Muhammad Yassar Jazaib Ali, Manzar Hussain. Case of lumbar spinal stenosis and chronic tophaceous gout. 18-Aug-2023;14:294. Available from: https://surgicalneurologyint.com/surgicalint-articles/12503/
Date of Submission
14-Jun-2023
Date of Acceptance
31-Jul-2023
Date of Web Publication
18-Aug-2023
Abstract
Background: Rarely, chronic tophaceous gout can result in lumbar spinal stenosis and neural compression.
Case Description: A 67-year-old male presented with the radiographic and magnetic resonance findings of gout involving and causing compression of the lumbar spine that responded to surgical decompression.
Conclusion: It is difficult to diagnose lumbar spinal stenosis secondary to tophaceous gout. Notably, the treatment, based on the clinical presentation, may include both medication and surgical decompression.
Keywords: Joint inflammation, Lumbar spinal stenosis, Multidisciplinary approach, Tophaceous gouty arthritis, Tophi, Urate crystals
INTRODUCTION
Tophaceous gouty arthritis is characterized by the accumulation of urate crystals in and around joints. It constitutes a chronic and debilitating form of arthritis that primarily affects the peripheral joints (i.e., toes, fingers, and knees), but can also involve other structures (i.e., tendons, bursa, and spine).[
CASE REPORT
A 67-year-old male presented with bilateral radicular lower back pain and neurogenic claudication (i.e., occurring within <5 min of ambulation) for 20 years. He also had pain in both his hands and feet. On physical examination, he had multiple hard, nodular swellings consistent with tophi in his hands and feet, including 0.5 cm tophi involving both big toes and the right little toe, a large 1.4 cm tophus involving the right middle finger, a 1 cm tophus on the right ring, and a 0.8 cm tophus at the right wrist [

Magnetic resonance (MR) studies
Axial and sagittal MR imaging views showed disc desiccation at multiple levels with disc space narrowing and Type II endplate changes at the L3/4 and L4/5 levels. At L3/4, L4/5, and L5/S1, there was significant bilateral lateral recess stenosis attributed to central disc bulges, and marked facet hypertrophy/reactive arthrosis and thickening of the yellow ligament. Added hyperintensities were also noted bilaterally adjacent to the spinous processes of L3 through L5 [
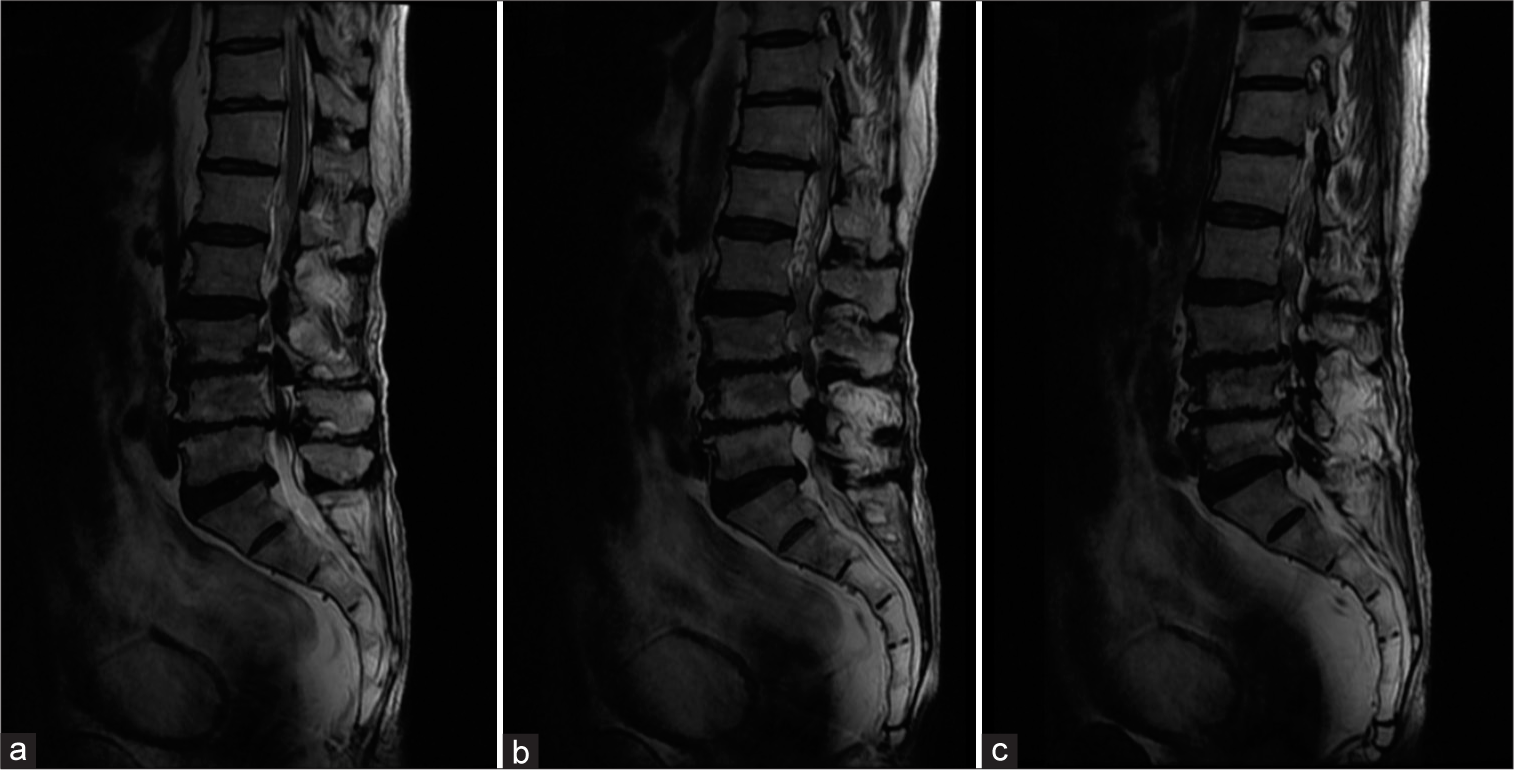

Figure 3:
Axial views of the magnetic resonance imaging lumbosacral spine at (a) L3-4, (b) L4-5, and (c) L5-S1 levels of the patient. The green arrow in (a) is demonstrating the thickening of the spinous process noted at the L3-4 level. The yellow arrow in (b) demonstrates a hyper-intense signal in the left paraspinal region.
Surgery
He underwent a decompressive laminectomy from L3 to L5 with medial facetectomy/foraminotomy and bilateral excision of tophi involving the spinous process and around the bilateral facet joints under spinal anesthesia. Intraoperatively, thickened yellow ligament and hypertrophied facet joints and spinous processes were removed along with multiple tophaceous nodules [

DISCUSSION
Definition of tophaceous spinal gout
Gout is a crystal arthropathy characterized by the deposition of uric acid within joints. The lumbar region is particularly susceptible to gout,[
Symptoms of spinal tophaceous gout
Patients may present with back pain, myelopathy, and/or radiculopathy (i.e., radiculopathy is the most prevalent symptom in 34.5% of cases)[
MR diagnosis of tophaceous spinal gout
Tophi, characteristic of gout, in the spine may produce a homogenous intermediate to hypointense signal on T1-weighted images, while intensity is variable on T2-weighted sequences.[
Medical management
Pharmacologic urate acid-lowering therapies form the mainstay of treatment for spinal gout and tophi. Gout is typically managed using colchicine, nonsteroidal anti-inflammatory drugs, or a combination of both to stabilize acute attacks. Urate-lowering therapy is achieved through the use of xanthine oxidase inhibitors (XOIs), which minimize uric acid synthesis and reduce serum urate levels.[
Surgery
When tophaceous gout contributes to spinal stenosis and root/cord compression, root surgical decompression often resulting in favorable outcomes may be warranted.[
CONCLUSION
Here, a 67-year-old male presented with lumbar radiculopathy and neurogenic claudication attributed to lumbar stenosis complicated by superimposed tophaceous gouty arthritis involving the yellow ligament, lumbar facet joints, and spinous processes. Notably, the patient markedly improved following the lumbar decompression surgery.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Elgafy H, Liu X, Herron J. Spinal gout: A review with case illustration. World J Orthop. 2016. 7: 766-75
2. Golenbiewski J, Keenan RT. Moving the needle: Improving the care of the gout patient. Rheumatol Ther. 2019. 6: 179-93
3. Hasegawa EM, de Mello FM, Goldenstein-Schainberg C, Fuller R. Gout in the spine. Rev Bras Reumatol. 2013. 53: 296-302
4. Hasturk AE, Basmaci M, Canbay S, Vural C, Erten F. Spinal gout tophus: A very rare cause of radiculopathy. Eur Spine J. 2012. 21: S400-3
5. King JC, Nicholas C. Gouty arthropathy of the lumbar spine: A case report and review of the literature. Spine (Phila Pa 1976). 1997. 22: 2309-12
6. Konatalapalli RM, Lumezanu E, Jelinek JS, Murphey MD, Wang H, Weinstein A. Correlates of axial gout: A cross-sectional study. J Rheumatol. 2012. 39: 1445-9
7. Richette P, Doherty M, Pascual E, Barskova V, Becce F, Castañeda-Sanabria J. 2016 updated EULAR evidence-based recommendations for the management of gout. Ann Rheum Dis. 2017. 76: 29-42
8. Wendling D, Prati C, Hoen B, Godard J, Vidon C, GodfrinValnet M. When gout involves the spine: Five patients including two inaugural cases. Joint Bone Spine. 2013. 80: 656-9
9. Yen PS, Lin JF, Chen SY, Lin SZ. Tophaceous gout of the lumbar spine mimicking infectious spondylodiscitis and epidural abscess: MR imaging findings. J Clin Neurosci. 2005. 12: 44-6
10. Zheng ZF, Shi HL, Xing Y, Li D, Jia JY, Lin S. Thoracic cord compression due to ligamentum flavum gouty tophus: A case report and literature review. Spinal Cord. 2015. 53: 881-6


JOSE LOMELI
Posted September 15, 2023, 10:34 am
Very interesting paper, there was a 3 level decompression, however if there was no spinal fussion like trasnpedicular fussion, then it is likely to have fail back syndrome in the future.