

- Professor of Clinical Neurosurgery, School of Medicine, State University of N.Y. at Stony Brook, Mineola, New York, USA
- Chief of Neurosurgical Spine and Education, Winthrop NeuroScience, NYU Winthrop Hospital, Mineola, New York, USA
Correspondence Address:
Nancy E. Epstein
Professor of Clinical Neurosurgery, School of Medicine, State University of N.Y. at Stony Brook, Mineola, New York, USA
Chief of Neurosurgical Spine and Education, Winthrop NeuroScience, NYU Winthrop Hospital, Mineola, New York, USA
DOI:10.4103/sni.sni_66_18
Copyright: © 2018 Surgical Neurology International This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.How to cite this article: Nancy E. Epstein. Case presentation and short perspective on management of foraminal/far lateral discs and stenosis. 23-Apr-2018;9:87
How to cite this URL: Nancy E. Epstein. Case presentation and short perspective on management of foraminal/far lateral discs and stenosis. 23-Apr-2018;9:87. Available from: http://surgicalneurologyint.com/surgicalint-articles/case-presentation-and-short-perspective-on-management-of-foraminal-far-lateral-discs-and-stenosis/
Date of Submission
27-Feb-2018
Date of Acceptance
27-Feb-2018
Date of Web Publication
23-Apr-2018
Abstract
Background:The management of lumbar foraminal/far lateral discs (FOR/FLD) with stenosis remains controversial. Operative choices should be based on each patient's preoperative dynamic X-ray findings, magnetic resonance (MR), and computed tomography (CT) studies. Here we reviewed several options for decompression alone vs. decompression with fusion.
Methods:Safe excision of FOR/FLD with stenosis should begin at the level above the disc herniation, as identification of the superior, foraminally, and far laterally exiting nerve root is critical. Performing an undercutting laminectomy and utilizing an operating microscope usually preserves the facet joints, and in many cases, avoids the need for fusion. Other decompressive techniques include; the intertransverse (ITT), and Wiltse approaches. Fusions following complete unilateral full facetectomy may be; noninstrumented (e.g., older, osteoporotic patients) vs. instrumented (e.g., posterolateral fusion or occasionally transforaminal lumbar interbody fusion). Here we present a patient with L2-L5 stenosis, and a left L3-L4 FOR/FLD, and multiple synovial cysts who was successfully managed with an l2-L5 laminecotmy, left L34 FOR/FLD diksectomy without fusion.
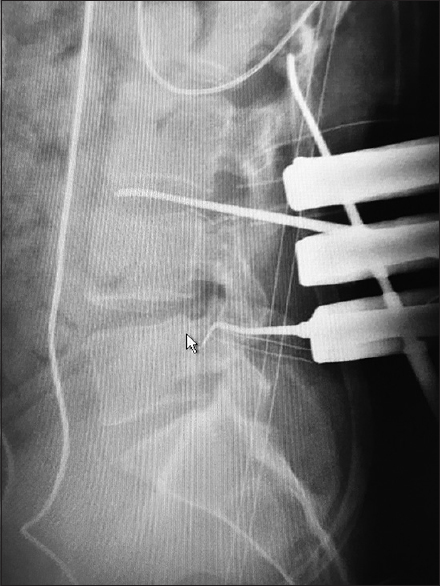
Results:Postoperatively, the patient was neurologically intact, and stability was maintained. Adjunctive measures for FOR/FLD diksectomy should include; intraoperative monitoring, use of the operating microscope, and an intraoperative film with a radiopaque marker in the correct disc space to confirm the correct level of diskectomy.
Conclusions:There are multiple approaches to the excision of FOR/FLD with stenosis. These include; decompression alone vs. decompression with non-instrumented vs. instrumented fusion. Surgical choices must be based on individual patient's X-ray, MR, and CT findings. The aim should be to maximize the safety of disc excision with decompression of stenosis, and to preserve stability, reducing the need for fusion, while minimizing morbidity.
Keywords: Decompression, facet excision, far lateral disc, foraminal, fusion, intertransverse technique, instrumented fusion, intraoperative monitoring, lumbar, microscope, Wiltse approach, X-ray control
INTRODUCTION
There are many techniques available for treating lumbar foraminal/far lateral disc (FOR/FLD) herniations with stenosis. The choice of surgical procedures must be based on each patient's preoperative dynamic X-ray, MR, and CT findings. Decompressive procedures may vary, and can include; laminotomy/laminectomy alone, the intertransverse approach (ITT), and Wiltse's far lateral technique. Where full unilateral facetectomy is warranted, patients may require noninstrumented vs. instrumented fusions (e.g., pedicle screws with posterolateral lumbar fusion (PLF), or rarely, transforaminal lumbar interbody fusion (TLIF)). No matter what operative approach is chose, adjunctive measures should include; continuous intraoperative physiological monitoring (e.g., somatosensory evoked potentials and electromyography), the use of an operating microscope, and an intraoperative radiograph with a marker within the disc space to confirm the correct level of disc removal.
MATERIALS AND METHODS
Symptoms and signs of foraminal/far lateral discs
The symptoms and signs for patients with lumbar FOR/FLD vary.[
Evaluation of FOR/FLD with dynamic X-rays, MR, and CT studies
Dynamic X-rays, MR, and CT studies contribute to the correct diagnosis, localization, and management of lumbar FOR/FLD and attendant stenosis.[
History of decompressive surgery for lumbar FOR/FLD
FLD: Wiltse far lateral approach to lumbar FLD
Wiltse and Spencer in 1988 described a purely far lateral approach to lumbar disc herniations [
Decompressions for 170 Lumbar FOR/FLD
In 1995, Epstein initially evaluated the surgical procedure/outcomes for 170 MR/CT confirmed FOR/FLD (1984–1994) [
SF-36 outcome study for FOR/FLD lumbar discs
In 1997, Epstein and Hood utilized the Medical Outcome Trust's SF-36 Short Form to assess outcomes for 76 (45% of the original sample of 170 patients) patients undergoing the three different operative approaches enumerated above for lumbar FOR/FLD (1984 and 1994) [
2007: Minimally invasive endoscopic discectomy/FOR/FLD; increased morbidity
In 2007, Sasani et al. evaluated the safety/efficacy of percutaneous minimally invasive (MI) endoscopic discectomy for FOR/FLD in 66 patients (1998–2005) [
2012: Three different minimally invasive decompressions for FOR/FLD
Liu et al. (2012) documented comparable results for three different MI procedures addressing 52 (2000–2006) FLD [
2014: Extraforaminal intertransverse (ITT) approach to lumbar FLD (far lateral lumbar disc herniation)
In 2014, Celikoglu et al. evaluated the extraforaminal surgical management of 33 far lateral lumbar discs utilizing an intertransverse approach (ITT) (e.g. with median or paramedian incisions) (2006–2011) [
Efficacy of laminectomy alone for excision of FOR/FLDs
Over two postoperative years, Epstein (2017) observed low complication and reoperation rates for 58 patients undergoing 2-3 level and 79 patients undergoing 4-6 level lumbar laminectomies without fusions, including those with FOR/FLD [
CASE REPORT
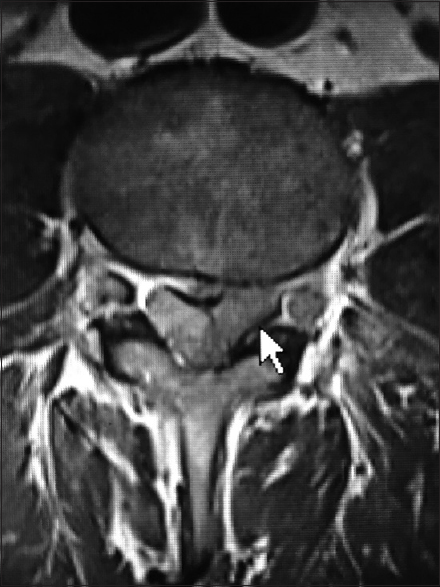
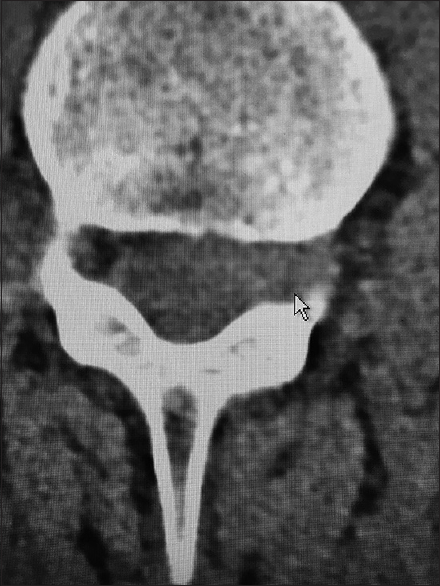
A patient with a history of low back pain, presented with 10 days of severe left lower extremity numbness, tingling, and weakness. The dynamic X-rays, MR, and CT studies demonstrated moderate stenosis/OYL L2-L5, bilateral synovial cysts at L4-L5, a left L3-L4 synovial cyst, and a massive left L3-L4 FOR/FLD with limbus fracture. The FOR/FLD disc herniation extended all the way to the L2-L3 level (e.g. markedly compressing the axilla of the L3 root) [Figures


Noninstrumented and instrumented fusion alternatives for lumbar FOR/FLD
Lumbar laminectomy with in situ fusion for stenosis and including FOR/FLD
In 2017, 59 patients underwent multilevel laminectomies (average 4.0 levels) and noninstrumented fusions (average 1.2 level) [
Decompression with instrumented fusion for far lateral lumbar discs
A unilateral full facetectomy may be required for excision of FOR/FLD, particularly when combined with severe spondyloarthrosis, DS, and/or spondylolisthesis/lysis. Here, a full facetectomy provides excellent visualization of the entire course of the cephalad, foraminally, and far laterally exiting nerve root along with the ipsilateral thecal sac and inferiorly exiting nerve root. In these cases, patients may require a posterolateral fusion (PLF) utilizing pedicle/screw instrumentation, or in select cases, a TLIF. Nevertheless, the addition of an interbody device may require increased manipulation of the thecal sac and/or nerve roots increasing perioperative morbidity (e.g., neruological root deficits, increased cerebrospinal fluid leak, etc.).
2016 Dorsal root ganglion (DRG) injury for MI TLIF for FLD
In 2016, Wang et al. observed that 5 (0.9%) of 539 patients exhibited postoperative dysesthesias (POD) attributed to DRG injury following MI TLIF (2010–2014) [
DISCUSSION
There are multiple alternative operative approaches for the management of lumbar FOR/FLD with stenosis. Preoperative assessment requires dynamic X-rays, MR, and CT studies to document the full extent/location of the FOR/FLD and accompanying stenosis and other degenerative pathology. When performing a medial intracanalicular decompression, one should utilize the operative microscope and the undercutting technique to preserve the lateral 2/3 of the facet joint, and maintain stability. Further, the extent of facet resection should be minimized by utilizing the operative microscope. The use of intraoperative monitoring should help avoid neural injury. Performing any one of the various MI techniques (e.g., endoscopic discectomy or MI TLIF) may unnecessarily add morbidity (e.g., root injury, retained disc, residual stenosis). Finally, no matter what the operative approach, it is critical to obtain an intraoperative lateral radiograph with an instrument in the correct disc space to avoid wrong level surgery.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Celikoglu E, Kiraz I, Is M, Cecen A, Ramazanoǧlu A. The surgical treatment of far lateral lumbar disc herniation: 33 cases. Acta Orthop Belg. 2014. 80: 468-76
2. Epstein NE. Evaluation of varied surgical approaches used in the management of 170 far-lateral lumbar disc herniations: Indications and results. J Neurosurg. 1995. 83: 648-56
3. Epstein NE, Hood DC. A comparison of surgeon's assessment to patient's self analysis (short form 36) after far lateral lumbar disc surgery.An outcome study. Spine (Phila Pa 1976). 1997. 22: 2422-8
4. Epstein NE, Hollingsworth RD. Nursing review section of Surgical Neurology International: Part 1 lumbar disc disease. Surg Neurol Int. 2017. 8: 301-
5. Epstein NE. High lumbar noninstrumented fusion rates using lamina autograft and Nanoss/bone marrow aspirate. Surg Neurol Int. 2017. 8: 153-
6. Epstein NE. Tisseel's impact on hemostasis for 2-3 and 4-6-level lumbar laminectomies. Surg Neurol Int. 2017. 8: 299-
7. Liu T, Zhou Y, Wang J, Chu TW, Li CQ, Zhang ZF. Clinical efficacy of three different minimally invasive procedures for far lateral lumbar disc herniation. Chin Med J (Engl). 2012. 125: 1082-8
8. Sasani M, Ozer AF, Oktenoglu T, Canbulat N, Sarioglu AC. Percutaneous endoscopic discectomy for far lateral lumbar disc herniations: Prospective study and outcome of 66 patients. Minim Invasive Neurosurg. 2007. 50: 91-7
9. Wang H, Zhou Y, Zhang Z. Postoperative dysesthesia in minimally invasive transforaminal lumbar interbody fusion: A report of five cases. Eur Spine J. 2016. 25: 1595-600
10. Wiltse LL, Spencer CW. New uses and refinements of the paraspinal approach to the lumbar spine. Spine (Phila Pa 1976). 1988. 13: 696-706

