

- Mar Gregorios Memorial Muthoot Medical Centre, Kozhencherry, Kerala, India
Correspondence Address:
Ajaya Kumar Ayyappan Unnithan
Mar Gregorios Memorial Muthoot Medical Centre, Kozhencherry, Kerala, India
DOI:10.4103/2152-7806.177886
Copyright: © 2016 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Ayyappan Unnithan AK, Joseph TP, Gautam A, Shymole V. Case report of lumbar intradural capillary hemangioma. Surg Neurol Int 02-Mar-2016;7:
How to cite this URL: Ayyappan Unnithan AK, Joseph TP, Gautam A, Shymole V. Case report of lumbar intradural capillary hemangioma. Surg Neurol Int 02-Mar-2016;7:. Available from: http://surgicalneurologyint.com/surgicalint_articles/case-report-of-lumbar-intradural-capillary-hemangioma/
Abstract
Background:Capillary hemangioma is a rare tumor in spinal intradural location. Despite the rarity, early recognition is important because of the risk of hemorrhage. This is a case report of a woman who had capillary hemangioma of cauda equina.
Case Description:A 54 -year-old woman presented with a low backache, radiating to the left leg for 2 months. She had left extensor hallucis weakness, sensory impairment in left L5 dermatome, and mild tenderness in lower lumbar spine. Magnetic resonance imaging (MRI) LS spine showed L4/5 intradural tumor, completely occluding canal in myelogram, enhancing with contrast, s/o benign nerve sheath tumor. L4 laminectomy was done. Reddish tumor was seen originating from a single root. It was removed preserving the root. Postoperatively, she was relieved of symptoms. MRI showed no residue. Histopathology showed lobular proliferation of capillary-sized blood vessels and elongated spindle cells. Immunohistochemistry showed CD34 positivity in endothelial cell lining of blood vessel and smooth muscle actin positivity in blood vessel muscle cells. HPR-capillary hemangioma.
Conclusion:Although rare, capillary hemangioma should be in the differential diagnosis of intradural tumors. It closely mimics nerve sheath tumor.
Keywords: Benign nerve sheath tumor, capillary hemangioma, cauda equina, intradural tumors, lumbar spinal tumors, meningioma
INTRODUCTION
Common spinal intradural tumors are schwannoma, meningioma, ependymoma etc. Capillary hemangioma is rare in this location. Despite the rarity, early recognition is important because of risk of hemorrhage. Literature shows only few reports of capillary hemangioma in this location. This is a case report of a woman who had capillary hemangioma of cauda equina.
CASE SUMMARY
A 54-year-old woman presented with a low backache for 2 months. Pain aggravated for 10 days. It was of lancinating type, radiating to left leg, increasing more in night. Pain was not relieved by medicines. It was progressively increasing in intensity. She had numbness in the left lateral leg and mild weakness of foot while walking. She has diabetes mellitus. On examination, she had positive straight leg raising test on the left side, left extensor hallucis weakness, sensory impairment for touch, and pain in left L5 dermatome. There was mild tenderness in the lower lumbar spine.
Magnetic resonance imaging (MRI) of lumbar spine was done. A well-defined oval-shaped solid mass lesion was seen in spinal canal at L4/L5 level within thecal sac. It measured 17 mm × 14 mm × 11 mm. It exhibited isointensity on T1-weighted and slight hyperintensity on the T2-weighted sequence. Lesion was seen in intradural compartment [


MRI brain screening was done to rule out any schwannoma, and it was normal.
Evaluatory investigations were hemoglobin - 13.5 g%, total count - 8100/mm3, platelet count - 240,000/mm3, blood sugar - 192 mg%, and urea - 26 mg%.
Surgery was done under general anesthesia in the prone position. L4 laminectomy was done under fluoroscopic guidance for localization. Dura was bulging. It was opened in midline. An oval reddish tumor was seen occupying the whole canal [


In the postoperative period, she was relieved of pain, numbness, and weakness. She was ambulated on the 3rd day. MRI was done, and it showed complete removal with no residue [

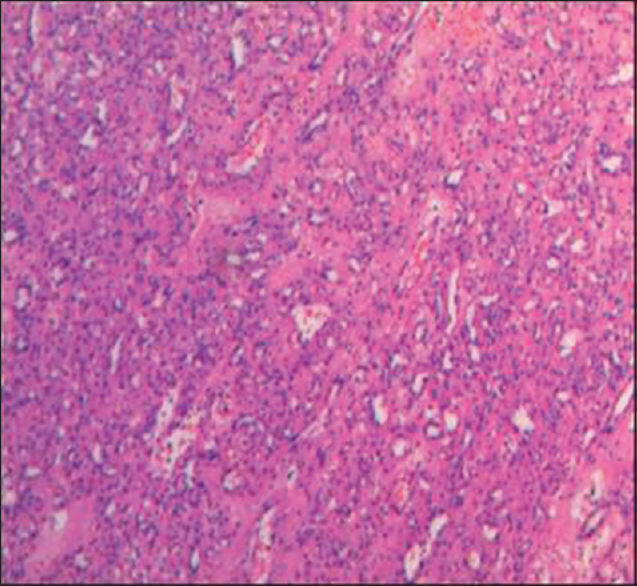
Histopathology sections showed a vascular spindle cell tumor composed of a lobular proliferation of capillary-sized blood vessels and elongated spindle cells [
DISCUSSION
The differential diagnosis for enhancing intradural tumors is schwannoma, meningioma, hemangioblastoma, hemangioma, paraganglioma, drop metastasis, lymphoma, filum terminale ependymoma, etc. The most common intradural tumors are schwannoma and meningioma.[
Capillary hemangioma (also known as “Strawberry hemangioma”) is the most common variant of hemangioma which appears as a raised, reddish-purple, lumpy area of flesh anywhere on the body. It most frequently occurs in cutaneous, subcutaneous, or mucosal tissues, and in those locations, it is commonly seen in childhood. It is characterized microscopically by the lobules of capillary-sized channels that are tightly aggregated into nodules nourished by feeding vessels. Hemangiomas, either capillary or cavernous, have been rarely encountered in the spinal intradural space.[
There are only a few reports of capillary hemangioma in this location. Most of the patients were between 50 and 60 years of age[
Our case also was similar in age, presentation, MRI findings, and peroperative findings. Only difference is that tumor was removed preserving the nerve root. Thus, the patient was relieved of symptoms completely.
CONCLUSION
This is a case report of lumbar intradural capillary hemangioma which was successfully excised. Although rare, capillary hemangioma should be in the differential diagnosis of intradural tumors. It closely mimics nerve sheath tumor. Literature shows good prognosis.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Choi BY, Chang KH, Choe G, Han MH, Park SW, Yu IK. Spinal intradural extramedullary capillary hemangioma: MR imaging findings. AJNR Am J Neuroradiol. 2001. 22: 799-802
2. Hanakita J, Suwa H, Nagayasu S, Suzuki H. Capillary hemangioma in the cauda equina: Neuroradiological findings. Neuroradiology. 1991. 33: 458-61
3. Holtzman RN, Brisson PM, Pearl RE, Gruber ML. Lobular capillary hemangioma of the cauda equina. Case report. J Neurosurg. 1999. 90: 239-41
4. Liu JJ, Lee DJ, Jin LW, Kim KD. Intradural extramedullary capillary hemangioma of the cauda equina: Case report and literature review. Surg Neurol Int. 2015. 6: S127-31
5. Miri SM, Habibi Z, Hashemi M, Meybodi AT, Tabatabai SA. Capillary hemangioma of cauda equina: A case report. Cases J. 2009. 2: 80-

