

- Department of Neurosurgery, Hospital de Clínicas, José de San Martín, Ciudad de Buenos Aires.
- Department of Cardiology, Hospital de Clínicas, José de San Martín, Ciudad de Buenos Aires.
Correspondence Address:
Javier Goland
Department of Neurosurgery, Hospital de Clínicas, José de San Martín, Ciudad de Buenos Aires.
DOI:10.25259/SNI-171-2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Javier Goland, Ezequiel Yasuda, Martín Monteverde, Silvia Garbugino. Catheter fragment retrieved from an arterial branch of the right middle cerebral artery. 28-Jun-2019;10:129
How to cite this URL: Javier Goland, Ezequiel Yasuda, Martín Monteverde, Silvia Garbugino. Catheter fragment retrieved from an arterial branch of the right middle cerebral artery. 28-Jun-2019;10:129. Available from: http://surgicalneurologyint.com/surgicalint-articles/9441/
Date of Submission
04-Mar-2019
Date of Acceptance
04-May-2019
Date of Web Publication
28-Jun-2019
Abstract
Background: Cerebral emboli is a rare complication of endovascular procedures and foreign bodies in the cerebrovascular system can lead to stroke. When an intravascular foreign body is identified, endovascular retrieval should be attempted due to its high success rate and minimal morbidity.
Case Description: A 59-year-old male patient underwent cine-coronario-graphy through a trans-radial approach because of angina. During the study, a 6Fr catheter fragment ruptured, detached and migrated to a right middle cerebral artery branch. We recovered it with a coronary balloon.
Conclusion: A coronary angioplasty balloon is an option for retrieving foreign objects or device fragments that have migrated into cerebral vasculature.
Keywords: Endovascular procedure, Fragment catheter, Complication, Coronary baloon
BACKGROUND
Cerebral emboli are commonly reported following thrombolysis, tumor embolization, and aneurysm occlusions with coils.[
CASE PRESENTATION
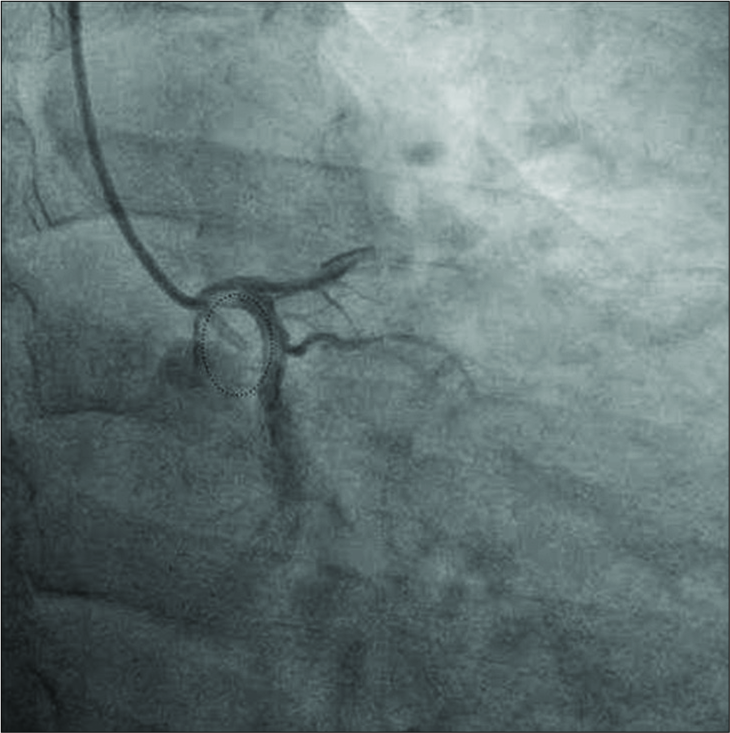
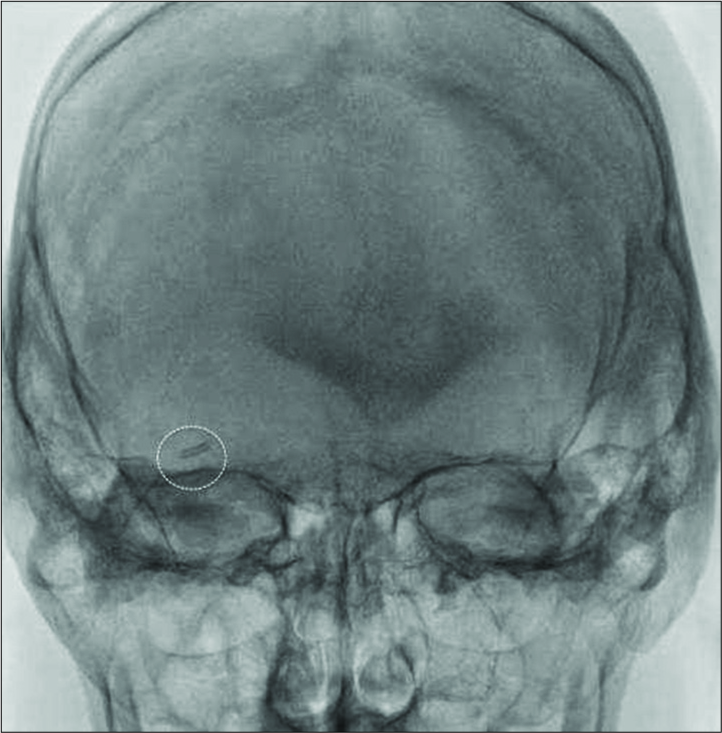
A 59-year-old male with a history of hypertension, heavy smoking, acute coronary syndrome, and circumflex artery stenting 1 year previously underwent coronary angiography, due to angina. It was performed through transradial access using a JR 6Fr catheter. During the study, a distal fragment of the catheter ruptured and migrated, lodging inside a branch of the right middle cerebral artery [
Treatment
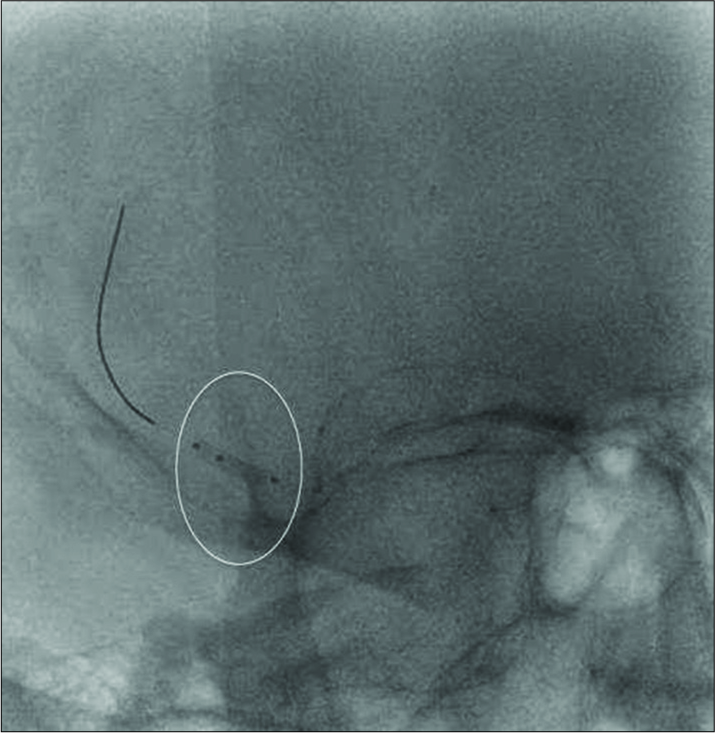
We decided to attempt retrieval of the catheter segment using the same radial approach as used for coronary angiography. With the patient under general anesthesia, the right carotid artery was catheterized with a Simmons II catheter (Merit Medical, South Jordan UT, USA), which was exchanged, using a 260 mm guide wire (Radifocus, Terumo, Somerset NJ, USA) in the external carotid, for a 6Fr guide catheter JR (Merit Medical, South Jordan UT, USA). We then catheterized the right internal carotid artery with a 6Fr guide catheter (Merit Medical, South Jordan UT, USA). Angiography revealed a radio-opaque fragment localized distal to the right medial cerebral artery bifurcation. With a 0.014 microwire (Hybrid 12–14, Balt, Montmorency, France), we navigated inside the catheter fragment, up to the M2-M3 segment. Then, we tried to pass it with a double-lumen 6 mm per 7 mm balloon (Eclipse, Balt, Montmorency, France), but it was impossible to pass distal to the catheter fragment with the balloon, and when we inflated it, the fragment was displaced distally [

We changed through a 300 mm 0.014 wire (FineCross, Terumo, Somerset NJ, USA), the remodeling balloon to a coronary angioplasty balloon of 1.25 mm per 20 mm (Ryujin, Terumo, Somerset NJ, USA), with which we were able to cross the catheter fragment. Then, we insufflated the balloon, half inside the fragment and half distal to it, and pulled the inflated balloon back. We retrieved the inflated balloon until it, and the catheter fragment reached the end of top of the guide catheter. Then, we retrieved the balloon, fragment, and guide catheter together, and all of them were extracted with the radial sheath [
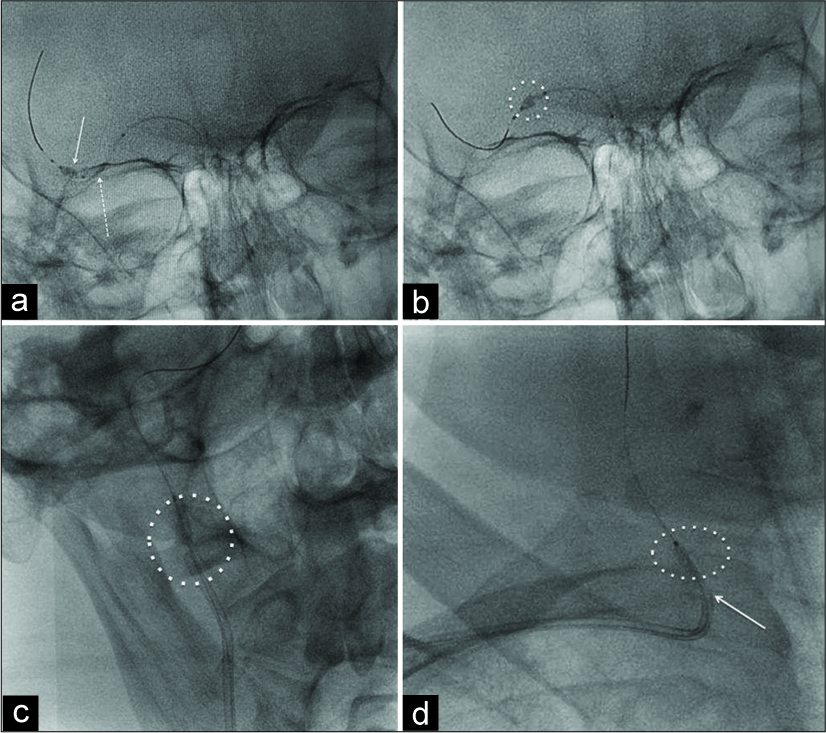
Figure 5:
(a) Skull radiography. Continued white arrow shows the inflated balloon half inside the catheter fragment and half distal to it. Dotted white arrow shows the catheter fragment. (b) Skull radiography. Dotted white circle shows the inflated balloon pushing the catheter fragment at M1 segment of cerebral media artery. (c) Facial bones radiography. Dotted white circle shows the catheter fragment near the tip of the guide catheter at cervical segment of carotid artery. (d) Chest radiography centered on the clavicle. Inside the dotted white circle, note the inflated balloon and catheter fragment at the level of the right common carotid’s origin. White arrow shows the tip of the guide catheter at the level of the right brachiocephalic trunk.
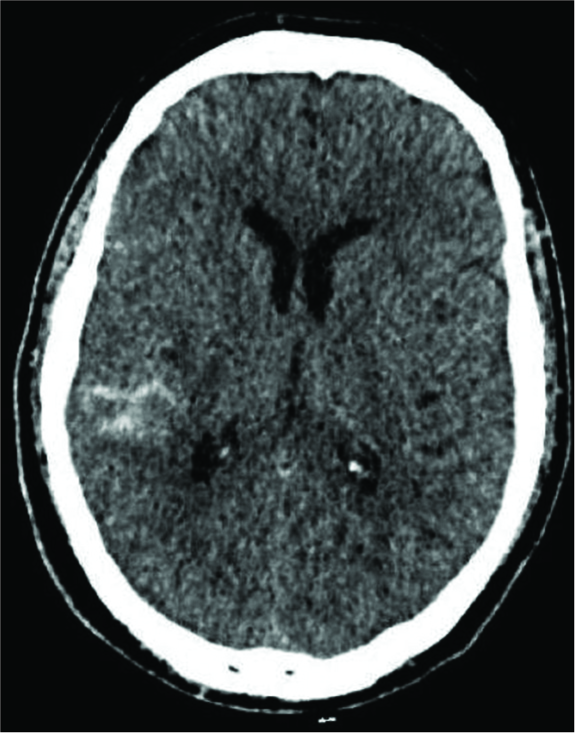
After the procedure, the patient reported a headache, after which computed tomography (CT) demonstrated a subarachnoid hemorrhage (SAH) [
DISCUSSION
There are published descriptions of conservative management of this situation, but results are difficult to predict when the situation appears.[
Cerebral emboli are a described complication of cerebrovascular procedures, and different devices have been utilized to retrieve them. Specific devices, listed previously, have been described for retrieving foreign bodies from the cerebrovascular circulation. Another technique, utilizing two microcatheters, or a microwire plus a microcatheter, or a stent retriever, has been employed in such circumstances.
However, there are no published reports of such a large fragment of catheter migrating to the cerebral circulation and being extracted, so it was not easy for us to decide which device to use in such a circumstance. In our patient, the foreign body that migrated was a 10 mm fragment of a JR 6Fr diagnosis catheter, which became lodged in a branch of the right middle cerebral artery. This was a problem since it was constructed of a rigid material and hence difficult to ensnare with a retriever stent, with a microcatheter and guidewire, or with a microsnare.
For this case, we believed that the best option was a balloon. Initially, we used a remodeling balloon that reaches up to 6 mm of diameter; however, since it was for cerebral vessels, it had a small enough profile. However, it was not rigid enough to completely pass through the catheter fragment. Then, we decided to try a lower profile coronary angioplasty balloon, which was a little stiffer; and this allowed us to cross the catheter fragment without difficulty. Once the tip of our guide catheter was reached, since it was the same size as the migrated fragment, we extracted the catheter, together with the guide wire, until we reached the introducer and then removed everything together, thereby recovering the migrated fragment.
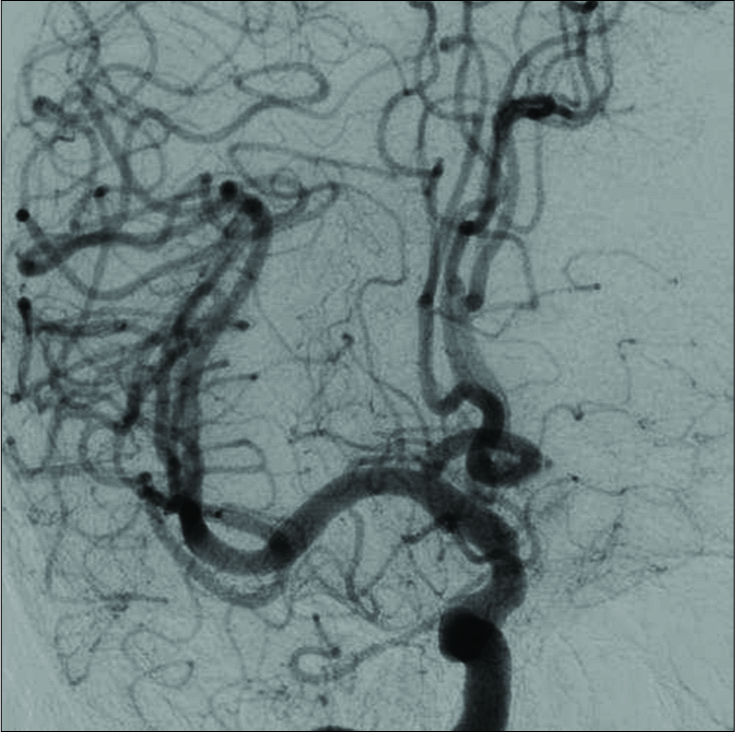
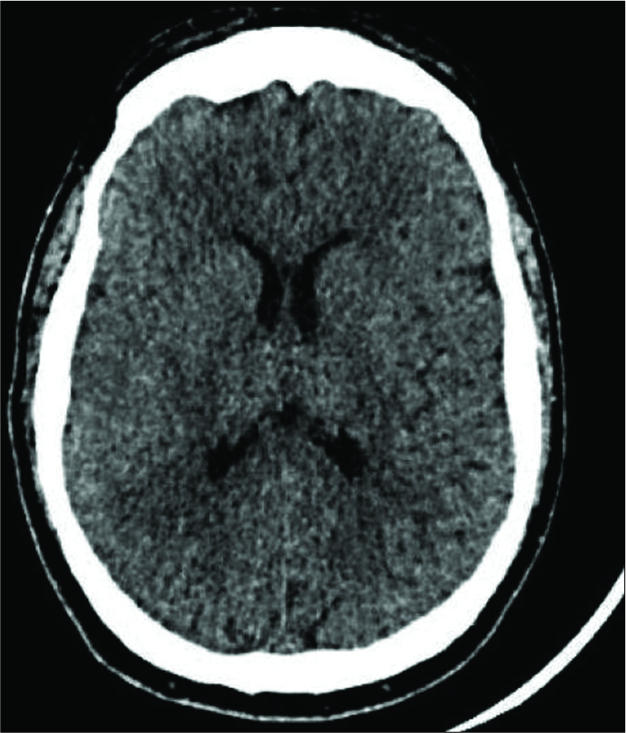
The patient had postprocedural headaches, for which a CT scan was considered indicated; and it revealed a SAH. We believe that the microwire’s rigidity was the cause of this complication, puncturing a vessel as the angioplasty balloon was being advanced. Follow-up cerebral angiography identified no contrast extravasation or pseudoaneurysm. The patient’s headaches resolved, with no further complications, and he was discharged 1 week after the procedure, at which time no residual SAH was observed on CT.
CONCLUSION
A coronary angioplasty balloon is an option for retrieving foreign objects or device fragments that have migrated into cerebral vasculature when a cerebral balloon fails.
Cerebral angiography is always required after an endovascular intervention.
Transradial artery approach is a good option for cerebral endovascular procedures.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Barnwell SL, D’Agostino AN, Shapiro SL, Nesbit GM, Kellogg JX. Foreign bodies in small arteries after use of an infusion microcatheter. AJNR Am J Neuroradiol. 1997. 18: 1886-9
2. Fealey ME, Edwards WD, Giannini C, Piepgras DG, Cloft H, Rihal CS. Complications of endovascular polymers associated with vascular introducer sheaths and metallic coils in 3 patients, with literature review. Am J Surg Pathol. 2008. 32: 1310-6
3. Mehta RI, Mehta RI, Fishbein MC, Solis OE, Jahan R, Salamon N. Intravascular polymer material after coil embolization of a giant cerebral aneurysm. Hum Pathol. 2009. 40: 1803-7
4. Carroll MI, Ahanchi SS, Kim JH, Panneton JM. Endovascular foreign body retrieval. J Vasc Surg. 2013. 57: 459-63
5. Al-Schameri AR, Deshmukh A, Debaseh H, Griessenauer C, Killer-Oberpfalzer M.editors. Accidental guide catheter fracture in mechanical thrombectomy. Interv Neuroradiol. 2018. 21: 1591019918814011-
6. Dinc H, Kuzeyli K, Kosuu P. Retrieval of prolapsed coils during endovascular treatment of cerebral aneurysms. Neuroradiology. 2006. 48: 269-72
7. Miyashita Y, Saigusa T, Ikeda U. Novel microsnare successfully used to remove small debris from the right coronary artery. J Invasive Cardiol. 2011. 23: E161-3
8. Kabbani MR, Smith A, Leider M. Endovascular coil retrieval using a trevoProVue stentriever. BMJ Case Rep. 2014. 2014: 2014011181-

