

- Department of Neurosurgery, Kagawa Rosai Hospital, Marugame, Kagawa, Japan
Correspondence Address:
Atsuhito Uneda
Department of Neurosurgery, Kagawa Rosai Hospital, Marugame, Kagawa, Japan
DOI:10.4103/sni.sni_210_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Atsuhito Uneda, Satoru Yabuno, Takahiro Kanda, Kenta Suzuki, Koji Hirashita, Masatoshi Yunoki, Kimihiro Yoshino. Cavernous angioma presenting with subarachnoid hemorrhage which was diffusely distributed in the basal cisterns and mimicked intracranial aneurysm rupture. 22-Aug-2017;8:202
How to cite this URL: Atsuhito Uneda, Satoru Yabuno, Takahiro Kanda, Kenta Suzuki, Koji Hirashita, Masatoshi Yunoki, Kimihiro Yoshino. Cavernous angioma presenting with subarachnoid hemorrhage which was diffusely distributed in the basal cisterns and mimicked intracranial aneurysm rupture. 22-Aug-2017;8:202. Available from: http://surgicalneurologyint.com/surgicalint-articles/cavernous-angioma-presenting-with-subarachnoid-hemorrhage-which-was-diffusely-distributed-in-the-basal-cisterns-and-mimicked-intracranial-aneurysm-rupture/
Date of Submission
09-Jun-2017
Date of Acceptance
11-Jul-2017
Date of Web Publication
22-Aug-2017
Keywords: Angiographically negative, cavernous angioma, cavernoma, subarachnoid hemorrhage
INTRODUCTION
Intracranial cavernous angiomas (cavernomas, cavernous hemangiomas, cavernous malformations) usually cause intraparenchymal hemorrhage but are rarely described as a cause of isolated subarachnoid hemorrhage (SAH).[
CASE REPORT
A 50-year-old woman suddenly developed severe headache, vomiting, and dizziness, and had a high blood pressure (193/103 mmHg). Brain computed tomography (CT) showed that SAH was diffusely distributed in the basal cisterns, as well as blood at the fourth ventricle [Figure
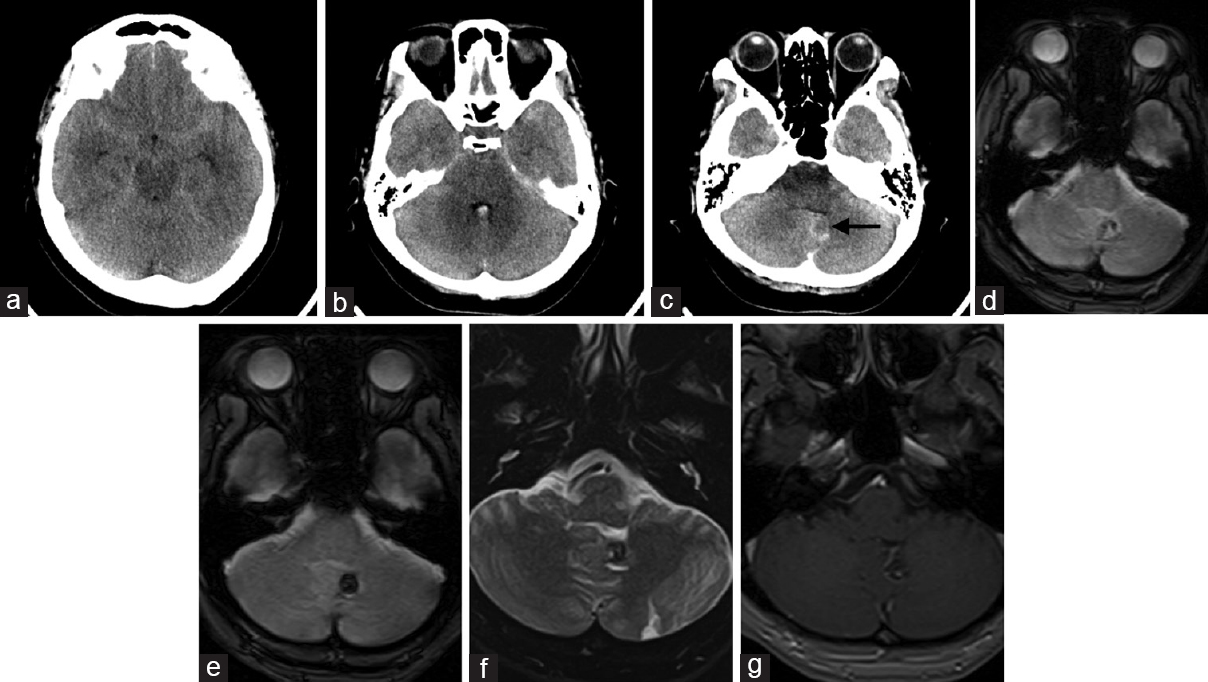
Figure 1
(a-c) Axial slices of acute unenhanced brain CT show SAH diffusely distributed in the basal cisterns and also show blood at the fourth ventricle. An obscure lesion, which suggested the presence of cavernous angioma (arrow), was found by retrospective review of the initial CT scan. (d) Axial T2-weighted image on day 10 shows a hypointense lesion on the surface of the left cerebellar hemisphere. (e) Axial T2-weighted image on day 16 more obviously shows the angioma. (f) Axial T2-weighted image on day 16 shows a mixed signal core surrounded by a hypointense rim. (g) Contrast-enhanced T1-weighted image shows a coexisting, developmental, venous anomaly
DISCUSSION
We described a case of cavernous angioma presenting with SAH, which was diffusely distributed in the basal cisterns and mimicked intracranial aneurysm rupture. Cavernous angiomas are vascular hematomas of blood vessels. The incidence of cavernous angiomas ranges 0.4–0.6% in the general population, and approximately 36% of these present with hemorrhage.[
Some cases of cavernous angiomas in the brain stem, cerebellum, cerebellopontine angle, sylvian cistern, and suprasellar cistern presenting with isolated SAH have been reported.[
The precise percentage of cavernous angioma in angiographically negative SAH is unknown. Of 213 patients with CT angiographically negative SAH, Heit et al. reported that a single cortical cavernous malformation (0.4%) was identified on MRI.[
In our case, the lesion gradually became apparent on delayed MRI over time. An obscure lesion, which suggested the presence of cavernous angioma, was found by a retrospective review of the initial CT after identifying the cavernous angioma on MRI. However, this lesion was difficult to identify at first review in the initial CT.
Surgically accessible cavernous angiomas with sudden or progressive symptoms and those with recurrent hemorrhage should be considered for surgical treatment.[
This report suggests that cavernous angioma should be considered in the differential diagnosis of patients with angiographically negative aneurysmal-like SAH. This condition should be considered even in the absence of distinct intraparenchymal hemorrhage that suggests the presence of angiographically occult cavernous angioma. A careful search of CT images for an obscure lesion that suggests the presence of cavernous angioma is important for early diagnosis, but this lesion is difficult to identify at first sight. Delayed brain MRI is the most useful method for revealing such an angioma.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Cantu C, Murillo-Bonilla L, Arauz A, Higuera J, Padilla J, Barinagarrementeria F. Predictive factors for intracerebral hemorrhage in patients with cavernous angiomas. Neurol Res. 2005. 27: 314-8
2. Cuvinciuc V, Viguier A, Calviere L, Raposo N, Larrue V, Cognard C. Isolated acute nontraumatic cortical subarachnoid hemorrhage. AJNR Am J Neuroradiol. 2010. 31: 1355-62
3. Escott EJ, Rubinstein D, Cajade-Law AG, Sze CI. Suprasellar cavernous malformation presenting with extensive subarachnoid hemorrhage. Neuroradiology. 2001. 43: 313-6
4. Gross BA, Du R. Cerebral cavernous malformations: Natural history and clinical management. Expert Rev Neurother. 2015. 15: 771-7
5. Gross BA, Lin N, Du R, Day AL. The natural history of intracranial cavernous malformations. Neurosurg Focus. 2011. 30: E24-
6. Heit JJ, Pastena GT, Nogueira RG, Yoo AJ, Leslie-Mazwi TM, Hirsch JA. Cerebral angiography for evaluation of patients with CT angiogram-negative subarachnoid hemorrhage: An 11-year experience. AJNR Am J Neuroradiol. 2016. 37: 297-304
7. Lenzi J, Seferi A, Nardone A, Salvati M, Vreto G, Santoro A. Sylvian subarachnoid and extra-pial cavernous angioma. J Neurosurg Sci. 2005. 49: 163-6
8. Pozzati E, Acciarri N, Tognetti F, Marliani F, Giangaspero F. Growth, subsequent bleeding, and de novo appearance of cerebral cavernous angiomas. Neurosurgery. 1996. 38: 662-
9. Takado Y, Minakawa T, Hadeishi H, Yoshida Y. A mass in the cerebellopontine angle presenting with subarachnoid haemorrhage. J Clin Neurosci. 2009. 16: 1051-117
10. Woodfield J, Rane N, Cudlip S, Byrne JV. Value of delayed MRI in angiogram-negative subarachnoid haemorrhage. Clin Radiol. 2014. 69: 350-6
11. Yaghi S, Oomman S, Keyrouz SG. Non-aneurysmal perimesencephalic subarachnoid hemorrhage caused by a cavernous angioma. Neurocrit Care. 2011. 14: 84-5
12. Yamamoto M, Fukushima T, Ikeda K, Nagasaka S, Sakamoto S, Oka K. Intracranial cavernous angioma manifesting as subarachnoid hemorrhage-case report. Neurol Med Chir (Tokyo). 1993. 33: 706-9

