

- Department of Neurosurgery of Hospital e Maternidade Celso Pierro, PUC-CAMPINAS, Campinas, São Paulo, Brazil
Correspondence Address:
T. A. B. Belsuzarri
Department of Neurosurgery of Hospital e Maternidade Celso Pierro, PUC-CAMPINAS, Campinas, São Paulo, Brazil
DOI:10.4103/sni.sni_359_16
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: N. B. Seixas, T. A. B. Belsuzarri, N. C. B. Belsuzarri, M. Pozetti, J. F. M. Araujo. Cavernous sinus syndrome as the first manifestation of metastatic breast disease. 05-Apr-2017;8:40
How to cite this URL: N. B. Seixas, T. A. B. Belsuzarri, N. C. B. Belsuzarri, M. Pozetti, J. F. M. Araujo. Cavernous sinus syndrome as the first manifestation of metastatic breast disease. 05-Apr-2017;8:40. Available from: http://surgicalneurologyint.com/surgicalint-articles/cavernous-sinus-syndrome-as-the-first-manifestation-of-metastatic-breast-disease/
Date of Submission
29-Aug-2016
Date of Acceptance
24-Jan-2017
Date of Web Publication
05-Apr-2017
Abstract
Background:The cavernous sinus is a venous plexus crossed by vital neurovascular structures. Metastases to the region are uncommon and often associated with a headache, facial pain, or progressive neurological deficit in III, IV, and VI cranial nerves. The treatment options are surgery, including endoscopic approach, radiotherapy, radiosurgery, and chemotherapy.
Case Description:We report the case of a 26-year-old female with cavernous sinus syndrome due to breast cancer metastasis, who was subjected to chemotherapy with complete neurological recovery. A literature review was performed using the databases Bireme, Pubmed, Cochrane, Lilacs and Medline with the keywords: cavernous sinus/metastasis/surgery/radiosurgery for multiple management options review.
Conclusion:Cavernous sinus metastases are rare, and the cavernous sinus syndrome is rarely the first sign of cancer, especially in young patients. Because the syndrome has multiple causes, the history of rapid progression and atypical image findings can arise suggesting metastatic diseases. As in our case, the image was suggestive of meningioma, however, the clinical presentation and further investigations led us to suspect as a metastatic disease. The therapeutic decision considers clinical and functional status, the extent of primary and metastatic disease, radiological study, tumor histopathology, and biological behavior. Often associated with significant symptoms and disseminated systemic disease, nowadays radiosurgery is the first and less invasive strategy, offering low risk of new deficits, clinical improvement, and good local control. The prognosis depends on early treatment and disease staging because mortality is associated with progression of cancer.
Keywords: Breast, cavernous sinus, metastasis, radiosurgery, surgery
INTRODUCTION
The cavernous sinus is a venous plexus crossed by vital neurovascular structures. Metastases to the region are uncommon and often associated with a headache, facial pain, or a progressive neurological deficit in III, IV, and VI cranial nerves.[
CASE REPORT
A 26-year-old woman presented with 10 months of diplopia, 4 months of hemifacial hypoesthesia at the right side, and 2 months of frontal headache, which was also associated with a superior visual field deficit of the right eye, an ocular dry, and a convergent strabismus in the same eye. During neurosurgery clinical analysis, the patient presented hypoesthesia of maxillary (V2) division of trigeminal nerve (V), associated with partial III and complete VI nerve palsy, on the right side. Moreover, the patient had a scalp lesion, which had shown progressive growth during the last month, for which biopsy was done on the same day. Magnetic resonance imaging (MRI) showed an irregular contrast-enhanced lesion on the right cavernous sinus, causing a slight mass effect in the brainstem [
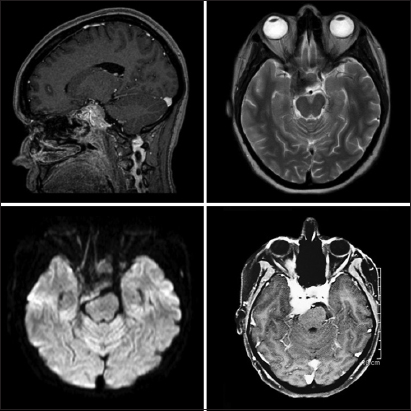
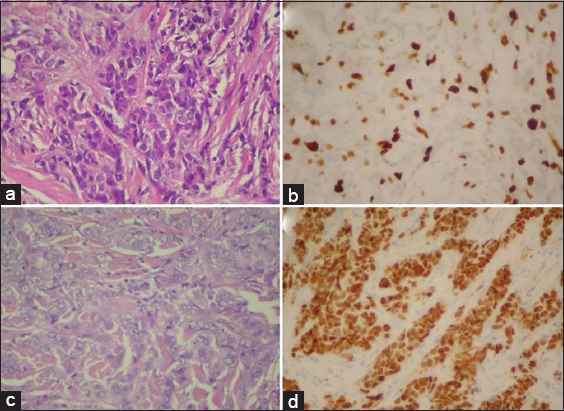
Figure 2
(a) Scalp histology: pleomorphic large cell neoplasia infiltrating subepithelial soft tissue (b) Scalp immunohistochemistry: epithelial neoplasia consistent with adenocarcinoma, breast or gynecological region are considered as possible primary sites - positive for estrogen receptors (c) Breast histology: invasive ductal carcinoma, Nottingham 2 (d) Breast immunohistochemistry: positivity for estrogen and progesterone receptors
DISCUSSION
The cavernous sinus is a venous plexus crossed by vital neurovascular structures. Metastases to the region are uncommon, and the anatomical proximity described is responsible for different clinical manifestations, secondary to inflammatory, vascular, or neoplastic diseases.[
Metastases to cavernous sinus occur in less than 1% of patients with cancer, and it is considered a late event when patients have disseminated disease.[
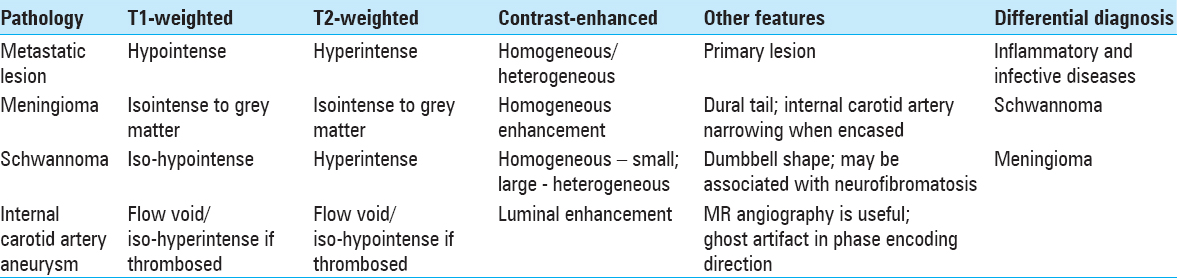
The diagnosis of metastatic lesion considers the clinical condition and the radiological findings obtained on MRI. This investigation can detect hypointense signal on T1-weighted images and hyperintense on T2-weighted images. Moreover, it can demonstrate homogeneous or heterogeneous contrast enhancement. In several cases, the cavernous sinus metastasis can be mistaken as a meningioma, as occurred in our patient. Clinical and radiological correlation can exclude the differential diagnosis of metastasis, which includes other neoplastic, inflammatory, or infective diseases, as some presented in
A study conducted by The Cleveland Clinic Foundation reported the use of 111 indium-octreotide brain scintigraphy (OBS) for noninvasive differentiation of meningiomas from other cranial dural-based pathology. The meningioma's somatostatin receptors bind to octreotide after 6 hours from administration, and small meningiomas (volume < 5 ml) should be evaluated after 24 hours. The OBS has 100% sensitivity, 50% specificity, and positive and negative predictor values of 75% and 100%, respectively. False positive results were found in 3 of the 50 patients studied (metastasis, chronic inflammation, and lymphoma).[
The low prevalence of metastasis to the cavernous sinus and the individual aspects of each case can perform different management strategies. Clinical and functional status, the extent of primary and metastatic disease, radiological study, tumor histopathology, and biological behavior, including response to prior therapy, are necessary for the therapeutic decision. Some tumors, as small cell lung cancer, breast cancer, and prostate cancer are sensitive to radiation and usually respond better to radiosurgery. On the other hand, melanoma, renal cell carcinoma, and sarcomas are frequently radioresistant, and surgery can be indicated in particular cases.[
In cavernous sinus lesions, usually, complete resection is not achieved and can be related to several complications. A surgical analysis of Pamir et al. evaluated the results of nonmeningeal tumors of the cavernous sinus. It was possible to achieve complete resection in 21 (50%) patients, and gamma knife radiosurgery was used in 13 and fractionated radiotherapy in 3 of the incompletely resected cases. The surgical approaches used were pterional extradural (Dolenc), cranial-orbitozygomatic and combined cranio-orbitozygomatic, and transfacial, 85.7%, 7.1%, and 4.8% of cases, and some were operated twice for tumor resection. Complications occurred in 12 (28.6%) patients, including cerebrospinal fluid fistula (4), hematoma in the surgical field (2), cerebral infarction (1), hydrocephalus (1), diabetes insipidus (1), and pulmonary embolus (1). The rate of cranial nerve morbidity was 26.1% for transient and 16.7% for new and permanent damage.[
Endonasal access can also be used for anterior skull base lesions and can be indicated as a possible site for biopsy if no other local could be achieved. Zacharia et al. studied 749 patients of New York Presbyterian Hospital, 12 (1.6%) with metastatic disease, 1 (8%) of them to the cavernous sinus. The case had a thyroid carcinoma as the primary tumor, presenting left ptosis as the clinical manifestation of the metastasis. The surgical approach was transsphenoidal, transselar, and transcavernous. The surgery obtained subtotal resection (STR).[
Radiosurgery, which began to be applied in the 1990s to patients who had failed in the previous radiotherapy, aims to preserve structures such as the optic nerve. Earlier treatment, within four months, is associated with better outcomes in cavernous sinus metastasis, since avoiding tumor progression and deterioration of nerve function. Furthermore, the effect is dose-dependent, and the dose must consider the lesion size (a volume of 6.3 cm3 was found in the study) and adjacent structures as optical apparatus. This relationship, previous radiotherapy, and larger tumor sizes were limiting factors of dose. Patients who received ≥15 Gy had better PFS, 22.9 months, compared to 9 months with lower margin dose. The PFS at one year was 89.7% and 35.9% for ≥15 Gy and <15 Gy, respectively. Although patients treated with the highest dose presented with lesion volume of 6.1 cm3, different of 11.7 cm3 of the lowest dose patients, the tumor size was not significantly associated with better PFS, which was attributed to higher marginal dose. Of the 34 patients with cranial nerve deficits, 12 (35.3%) improved by approximately 1.7 months after treatment, associated with optic nerve (33.3%), oculomotor (33.3%), trochlear (40%), trigeminal (36.8%), and abducent (40%) in addition to the improvement of facial palsy (10%). Of the four patients with hearing loss, none reported a change. Worsening of symptoms occurred in 8 patients, related to disease progression and not to radiosurgery. The remaining patients did not report clinical response to the treatment.[
Iwai et al. reported 47% improvement among 21 patients who underwent radiosurgery due to cranial nerve deficits secondary to metastasis to the cavernous sinus. Of these, 3 had complete success and 7 revealed good results related to the nerves – optic (2), oculomotor (2), trigeminal (4) and abducent (4). No patient experienced nausea, vomiting, damage to cranial nerves, or radiographic and clinical evidence of radiation necrosis. The deaths were a result of tumor progression or bleeding in 2 cases, and 1 case had meningitis caused by the reduction of the tumor by radiosurgery.[
Chemotherapy is used for disseminated disease, however, can be limited due to the ability to cross the blood–brain barrier. Agent and concentration are directly associated with the brain penetration.[
Nowadays surgical resection for metastatic brain metastasis, even more for cavernous sinus, are not usually indicated. New chemotherapies and radiosurgery can achieve good local control with good neurological recovery without surgical risks.
CONCLUSION
Cavernous sinus metastases are often associated with prominent symptoms and disseminated systemic disease. We presented a case of a patient with a cavernous sinus lesion which was the first symptomatic lesion in a metastatic breast disease. The lesion was first radiologically diagnosed as a meningioma, nevertheless with further investigation and the clinical correlation, was rediscussed to be a cavernous sinus metastasis, that was referred to systemic chemotherapy and stereotactic radiosurgery for the lesion. After a month of chemotherapy, the patient had complete regression of the symptoms and the radiosurgery expected was no longer indicated.
Surgery can be indicated in metastases without a defined diagnosis, brain swelling, and manifestations due to its location, as brainstem compression,[
The prognosis depends on the histologic type of the primary tumor, disease staging, and proximity to the optical apparatus, which defines the dose in radiosurgery. The use of ≥15 Gy showed better PFS,[
Cavernous sinus metastases are a significant differential diagnose of the syndrome associated. In approximately 28% of cases the lesions can be the first sign of cancer;[
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Chaichana KL, Flores M, Acharya S, Sampognaro P, Bettegowda C, Rigamonti D. Survival and recurrence for patients undergoing surgery of skull base intracranial metastases. J Neurol Surg B. 2013. 74: 228-35
2. Chamoun RB, DeMonte F. Management of skull base metastases. Neurosurg Clin N Am. 2011. 22: 61-6
3. Chamoun RB, Suki D, DeMonte F. Surgical management of cranial base metastases. Neurosurgery. 2012. 70: 802-10
4. Iwai Y, Yamanaka K, Yoshimura M. Gamma knife radiosurgery for cavernous sinus metastases and invasion. Surg Neurol. 2005. 64: 406-10
5. Kano H, Niranjan A, Kondziolka D, Flickinger JC, Lunsford LD. The role of palliative radiosurgery when cancer invades the cavernous sinus. Int J Radiation Oncology Biol Phys. 2009. 73: 709-15
6. Mehta MP, Paleologos NA, Mikkelsen T, Robinson PD, Ammirati M, Andrews DW. The role of chemotherapy in the management of newly diagnosed brain metastases: A systematic review and evidence-based clinical practice guideline. J Neurooncol. 2010. 96: 71-83
7. Nadarajah J, Madhusudhan KS, Yadav AK, Chandrashekhara SH, Kumar A. MR imaging of cavernous sinus lesions: Pictorial review. J Neuroradiol. 2015. 42: 305-19
8. Nathoo N, Ugokwe K, Chang AS, Li L, Ross J, Suh JH. The role of 111indium-octreotide brain scintigraphy in the diagnosis of cranial, dural-based meningiomas. J Neurooncol. 2007. 81: 167-74
9. Pallini R, Sabatino G, Doglietto F, Lauretti L, Fernandez E, Maira G. Clivus metastases: Report of seven patients and literature review. Acta Neurochir. 2009. 151: 291-6
10. Pamir MN, Kilic T, Özek MM, Özduman K, Türe U. Non-meningeal tumours of the cavernous sinus: A surgical analysis. J Clin Neurosci. 2006. 13: 626-35
11. Zacharia BE, Romero FR, Rapoport SK, Raza SM, Anand VK, Schwartz TH. Endoscopic endonasal management of metastatic lesions of the anterior skull base: Case series and literature review. World Neurosurg. 2015. 84: 1267-77

