

- Department of Radiation Oncology, The Ohio State University, Columbus, Ohio, United States.
- Department of Neuropathology The Ohio State University, Columbus, Ohio, United States.
- Department of Neurosurgery, The Ohio State University, Columbus, Ohio, United States.
Correspondence Address:
Raju. R. Raval, Department of Radiation Oncology, The Ohio State University, Columbus, Ohio, United States.
DOI:10.25259/SNI_781_2021
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Khaled Dibs1, Rahul Neal Prasad1, Kajal Madan1, Kevin Liu1, Will Jiang1, Jayeeta Ghose1, Dukagjin M. Blakaj1, Joshua D. Palmer1, Peter Kobalka2, Daniel M. Prevedello3, Raju R. Raval1. Cerebellopontine angle ependymoma presenting as isolated hearing loss in an elderly patient: A case report and literature review. 23-Nov-2021;12:572
How to cite this URL: Khaled Dibs1, Rahul Neal Prasad1, Kajal Madan1, Kevin Liu1, Will Jiang1, Jayeeta Ghose1, Dukagjin M. Blakaj1, Joshua D. Palmer1, Peter Kobalka2, Daniel M. Prevedello3, Raju R. Raval1. Cerebellopontine angle ependymoma presenting as isolated hearing loss in an elderly patient: A case report and literature review. 23-Nov-2021;12:572. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=11243
Date of Submission
05-Aug-2021
Date of Acceptance
19-Oct-2021
Date of Web Publication
23-Nov-2021
Abstract
Background: Ependymoma is an uncommon tumor accounting for approximately 1.9% of all adult central nervous system tumors. Ependymomas at the cerebellopontine angle (CPA) are even more rare and only previously described in isolated case reports. Typically, acoustic neuromas and meningiomas represent the bulk of adult CPA tumors. Diagnosis can be challenging, as ependymomas have clinical findings and imaging characteristics that overlap with more common tumor histologies at the CPA.
Case Description: We present the case of a 70-year-old male patient with progressive, isolated left-sided hearing loss found to have a World Health Organization (WHO) Grade II CPA ependymoma, representing one of the oldest recorded patients presenting with this primarily pediatric malignancy in this unique location. The patient presentation with isolated hearing loss was particularly unusual. When associated with neurologic deficits, CPA ependymomas more characteristically result in facial nerve impairment with fully preserved hearing, while vestibular schwannomas tend to present with isolated hearing loss. The standard of care for pediatric ependymomas is maximal safe resection with adjuvant radiotherapy, but treatment paradigms in adult CPA ependymoma are not well defined particularly for WHO Grade II disease. After resection, he received adjuvant radiation to decrease the risk of local recurrence. Twenty-nine months after resection, the patient remains free of treatment-related toxicity or disease recurrence.
Conclusion: We review this patient’s clinical course in the context of the literature to highlight the challenges associated with timely diagnosis of this rare tumor and the controversial role of adjuvant therapy in preventing local recurrence in these patients.
Keywords: Adjuvant therapy, Adult ependymoma, Cerebellopontine angle ependymoma, Ependymoma, Radiation therapy
INTRODUCTION
Ependymoma is an uncommon tumor accounting for approximately 1.9% of all adult central nervous system (CNS) tumors.[
CASE DESCRIPTION
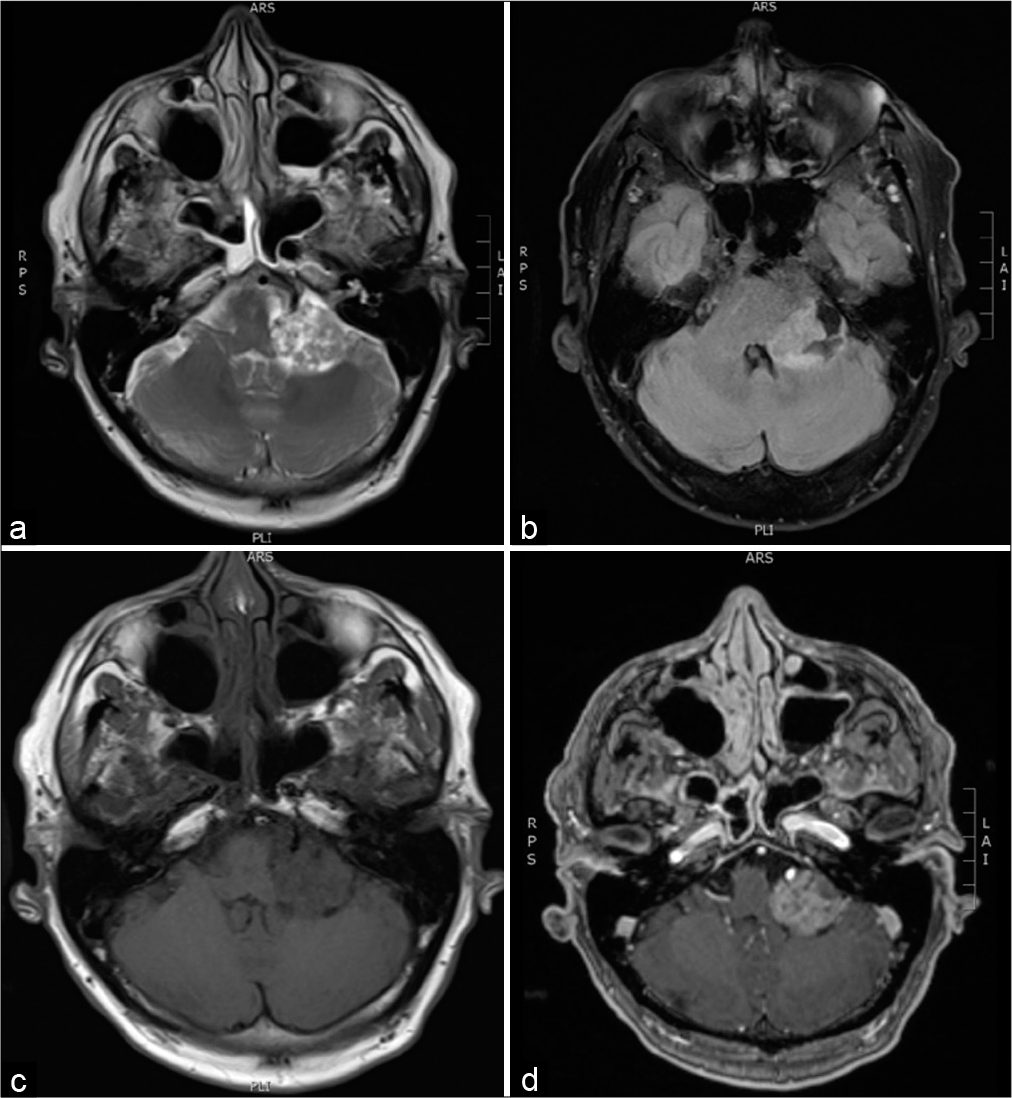
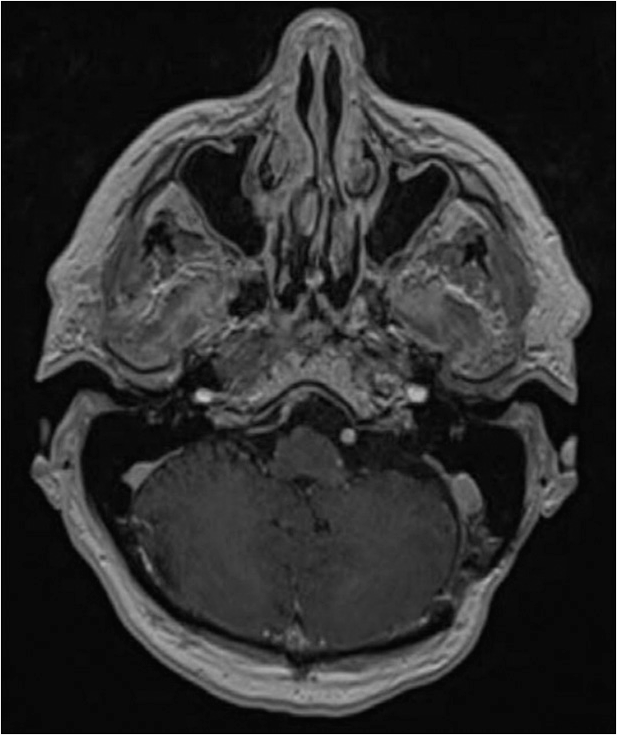
A 70-year-old male presented to our institution with progressive left-sided hearing deficit over several years with accelerated loss in the immediately preceding months. He denied headache, weakness, numbness, nausea, vomiting, dysphagia, speech issues, dizziness, vertigo, and difficulty walking. Physical examination including detailed neurologic exam was unremarkable except for significant left-sided hearing loss confirmed by audiogram; the facial nerve was intact. MRI of the brain with contrast revealed a 2.5 cm heterogeneously enhancing, extra-axial, well-defined mass with cystic components in the left CPA causing mild to moderate mass effect on the left-sided pons, anterior cerebellar hemisphere, and middle ear cerebellar peduncle [
Surgical pathology was significant for cells arranged in perivascular pseudorosette formations.
Immunohistochemistry revealed tumor cells diffusely positive for glial fibrillary acidic protein and S100 with scattered positivity for Olig2 and epithelial membrane antigen (dot-like perinuclear), and a Ki-67 proliferation index highlighted up to 15% of tumor cell nuclei [
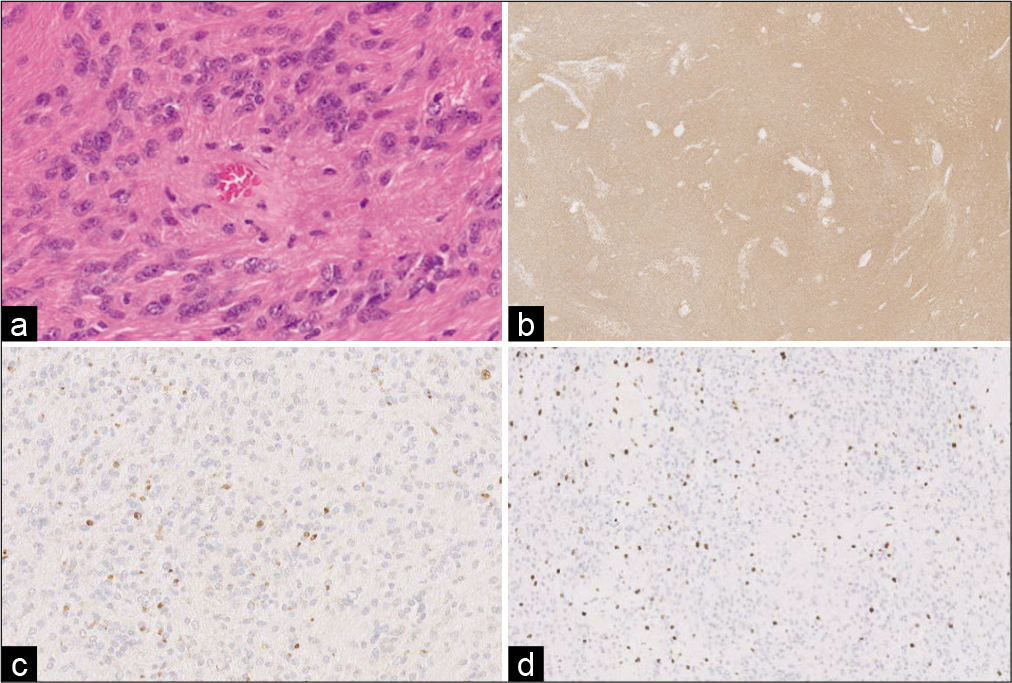
Figure 2:
Hematoxylin and eosin-stained sections from surgical pathology revealed a non-infiltrating glial neoplasm with round to ovoid cells arranged in perivascular pseudorosette formations (a, ×40). Tumor cells were diffusely positive for glial fibrillary acidic protein (b, ×20) and epithelial membrane antigen in a scattered, dot-like perinuclear distribution (c, ×20). A Ki-67 proliferation index highlighted up to 15% of tumor cell nuclei (d, ×10). Based on these findings, a diagnosis of WHO Grade II ependymoma was made.
The role of post-operative radiotherapy in patients with ependymoma WHO grade II undergoing gross tumor resection remains controversial. Because this patient was >59 years at presentation, male sex, and had a rare site of presentation with unknown molecular subgroup, radiotherapy for improved local control was offered after discussion at multidisciplinary tumor board. A dose of 5400 cGy in 30 daily fractions was prescribed to the planning target volume which consisted of the resection cavity plus a 3 mm margin as identified on the T1 post-contrast MRI sequence [
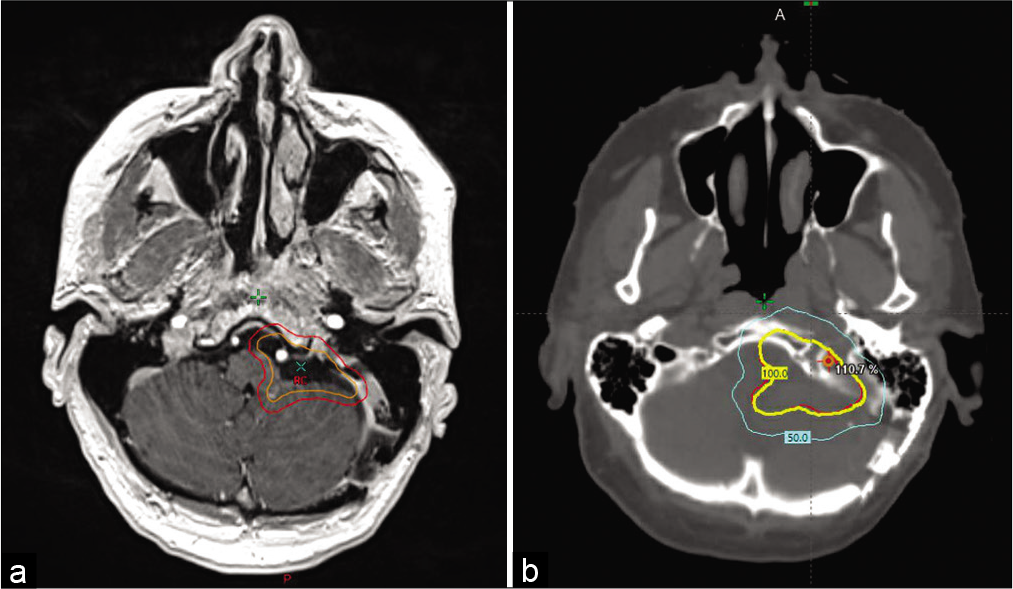
Figure 3:
The planning target volume (PTV) consisted of the resection cavity (outlined in orange) plus a 3 mm margin (outlined in red) as identified on the T1 post-contrast sequence (a). 100% of the dose was prescribed to this volume. A 3-arc volumetric modulated arc therapy technique with 6-MV photons was used to cover the volume with the 100% isodose line (5400 cGy) (in yellow) covering the PTV target (resection cavity + 3 mm margin) (in red) on the planning CT head (b).
DISCUSSION
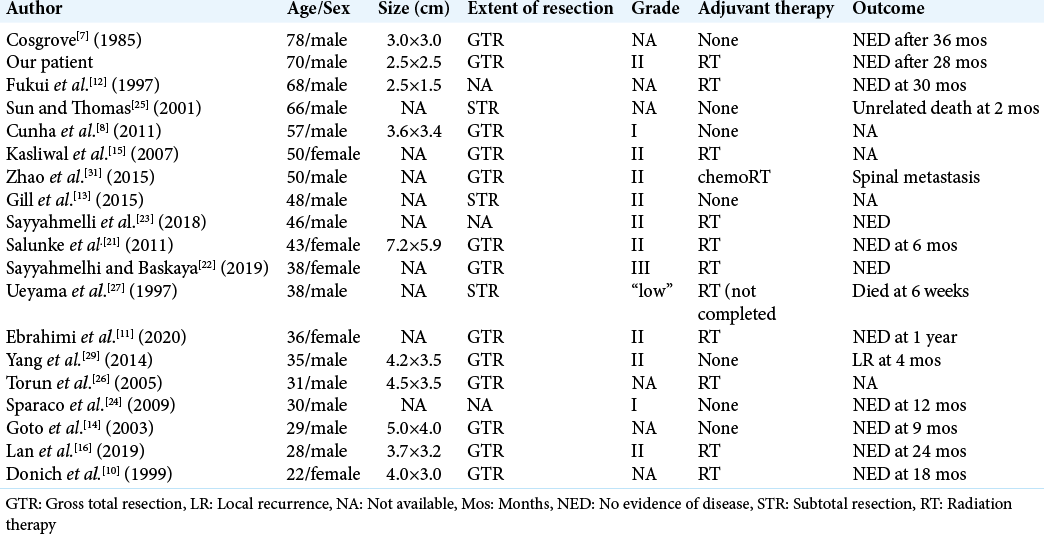
We present nearly the oldest recorded case of a patient presenting with CPA ependymoma, which presented significant challenges for diagnosis and management due to the uniqueness of this histology in a patient of this age and the paucity of literature guiding adjuvant therapy. Nearly every previously reported case of CPA ependymoma occurred in the fifth decade or earlier [
Given the rarity of CPA ependymoma, there is only limited retrospective data to help identify patients most likely to benefit from adjuvant treatment. Poor prognostic factors identified in adults include advanced age >68, anaplastic histology, high E3 ubiquitin ligase MIB-1 labeling index, and the extent of resection.[
CONCLUSION
In summary, we present nearly the oldest recorded case of a patient presenting with CPA ependymoma, which demonstrates that diagnosing CPA ependymoma in elderly adults based on imaging and symptoms alone can be challenging due to overlapping characteristics with tumors more commonly seen at this location including vestibular schwannoma. Although surgery, when feasible, is first line therapy for every tumor in the differential diagnosis, improving the odds of an accurate clinical diagnosis is essential to providing accurate upfront prognostic information to guide patient expectations. With limited evidence to guide therapy, the role of adjuvant therapy remains uncertain particularly for patients with the WHO Grade II disease, although groups at higher risk of recurrence have increasingly been identified. Further investigations into the role and potential benefit of adjuvant radiotherapy for patients with CPA ependymoma are warranted.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Amirian ES, Armstrong TS, Aldape KD, Gilbert MR, Scheurer ME. Predictors of survival among pediatric and adult ependymoma cases: A study using surveillance, epidemiology, and end results data from 1973 to 2007. Neuroepidemiology. 2012. 39: 116-24
2. Amirian ES, Armstrong TS, Gilbert MR, Scheurer ME. Predictors of survival among older adults with ependymoma. J Neurooncol. 2012. 107: 183-9
3. Armstrong TS, Vera-Bolanos E, Bekele BN, Aldape K, Gilbert MR. Adult ependymal tumors: Prognosis and the M.D. Anderson Cancer Center experience. Neuro Oncol. 2010. 12: 862-70
4. Bonneville F, Sarrazin JL, Marsot-Dupuch K, Iffenecker C, Cordoliani YS, Doyon D. Unusual lesions of the cerebellopontine angle: A segmental approach. Radiographics. 2001. 21: 419-38
5. Bonneville F, Savatovsky J, Chiras J. Imaging of cerebellopontine angle lesions: An update. Part 1 Enhancing extra-axial lesions. Eur Radiol. 2007. 17: 2472-82
6. Bonneville F, Savatovsky J, Chiras J. Imaging of cerebellopontine angle lesions: An update Part 2 Intra-axial lesions, skull base lesions that may invade the CPA region, and non-enhancing extra-axial lesions. Eur Radiol. 2007. 17: 2908-20
7. Cosgrove GR, Villemure JG, Robitaille Y, Melanson D. Extraaxial ependymoma of the posterior fossa. Surg Neurol. 1985. 24: 433-6
8. Cunha AM, Brito AC, de Almeida Lima G, de Souza LA, Simões EL, Telles C. Cerebellopontine angle subependymoma without fourth ventricle extension: An uncommon tumor in a rare location. Neuropathology. 2012. 32: 164-70
9. DeLong M, Kaylie D, Kranz PG, Adamson DC. Vestibular schwannomas: Lessons for the neurosurgeon: Part I: Diagnosis, neuroimaging, and audiology. Contemp Neurosurg. 2011. 33: 1-5
10. Donich D, Lee JH, Prayson R. Giant extra-axial cerebellopontine angle/cavernous sinus ependymoma: case report. Neurosurgery. 1999. 44: 195-8
11. Ebrahimi H, Jelodar S, Yarandi KK, Javadi AE, Alimohamadi M. Adult cerebellopontine angle ependymoma presenting as an isolated cisternal mass: A case report. J Med Imaging Radiat Sci. 2020. 51: 689-93
12. Fukui MB, Hogg JP, Martinez AJ. Extraaxial ependymoma of the posterior fossa. AJNR Am J Neuroradiol. 1997. 18: 1179-81
13. Gill AS, Taheri MR, Hamilton J, Monfared A. Extra-axial ependymoma presenting as a cerebellopontine angle mass. Otol Neurotol. 2015. 36: e138-9
14. Goto T, Ohata K, Tsuyuguchi N, Takami T, Hara M. Extra-axial subarachnoid ependymoma of the cerebral convexity. Acta Neurochir (Wien). 2003. 145: 913-7
15. Kasliwal MK, Chandra PS, Sharma BS. Images in neuro oncology: Primary extraaxial cerebellopontine angle ependymoma. J Neurooncol. 2007. 83: 31-2
16. Lan Z, Richard SA, Zhang Y. Cerebellopontine angle ependymoma in a young adult: A case report. Medicine (Baltimore). 2019. 98: e15019
17. Luryi AL, Michaelides EM, Babu S, Bojrab DI, Kveton JF, Hong RS. Reliability of clinical diagnosis of masses of the cerebellopontine angle: A retrospective multi-institutional study. Am J Otolaryngol. 2019. 40: 133-6
18. Merchant TE, Bendel AE, Sabin ND, Burger PC, Shaw DW, Chang E. Conformal radiation therapy for pediatric ependymoma, chemotherapy for incompletely resected ependymoma, and observation for completely resected, supratentorial ependymoma. J Clin Oncol. 2019. 37: 974-83
19. Metellus P, Guyotat J, Chinot O, Durand A, Barrie M, Giorgi R. Adult intracranial WHO grade II ependymomas: Long-term outcome and prognostic factor analysis in a series of 114 patients. Neuro Oncol. 2010. 12: 976-84
20. Ostrom QT, Gittleman H, Fulop J, Liu M, Blanda R, Kromer C. CBTRUS statistical report: Primary brain and central nervous system tumors diagnosed in the United States in 2008-2012. Neuro Oncol. 2015. 17: iv1-62
21. Salunke P, Kovai P, Sura S, Gupta K. Extra-axial ependymoma mimicking a parasagittal meningioma. J Clin Neurosci. 2011. 18: 418-20
22. Sayyahmelli S, Baskaya MK. Microsurgical resection of anaplastic ependymoma of the cerebellopontine angle in an adult: 3-Dimensional operative video. Oper Neurosurg (Hagerstown). 2019. 16: E91
23. Sayyahmelli S, Ucer M, Baskaya MK. Microsurgical gross total resection of a WHO grade II cerebellopontine angle ependymoma in an adult. J Neurol Surg B Skull Base. 2018. 79: S426-7
24. Sparaco M, Morelli L, Piscioli I, Donato S, Catalucci A, Licci S. Primary myxopapillary ependymoma of the cerebellopontine angle: Report of a case. Neurosurg Rev. 2009. 32: 241-4
25. Sun X, Thomas C. Pathologic quiz case: An unusual cerebellopontine angle tumor. Arch Pathol Lab Med. 2001. 125: 1113-4
26. Torun F, Tuna H, Bozkurt M, Deda H. Extra-axial ependymoma of posterior fossa extending to the Meckel’s cave. Clin Neurol Neurosurg. 2005. 107: 334-6
27. Ueyama T, Tamaki N, Kondoh T, Kokunai T, Asada M. Cerebellopontine angle ependymoma with internal auditory canal enlargement and pineal extension--case report. Neurol Med Chir (Tokyo). 1997. 37: 762-5
28. Weber DC, Wang Y, Miller R, Villà S, Zaucha R, Pica A. Long-term outcome of patients with spinal myxopapillary ependymoma: Treatment results from the MD Anderson cancer center and institutions from the rare cancer network. Neuro Oncol. 2015. 17: 588-95
29. Yang X, Ren Y, Wu W, Wang X, Liu X, Zhang Y. Intracranial extra-axial ependymoma involving the petroclival region: A rare case report. Int J Clin Exp Pathol. 2014. 7: 9067-71
30. Yuh EL, Barkovich AJ, Gupta N. Imaging of ependymomas: MRI and CT. Childs Nerv Syst. 2009. 25: 1203-13
31. Zhao C, Wang C, Zhang M, Jiang T, Liu W, Li W. Primary cerebellopontine angle ependymoma with spinal metastasis in an adult patient: A case report. Oncol Lett. 2015. 10: 1755-8

