

- Department of Anesthesiology, Kansai Medical University, Hirakata, Japan.
- Department of Neurosurgery, Kansai Medical University, Hirakata, Japan.
Correspondence Address:
Satoshi Aihara, Department of Anesthesiology, Kansai Medical University, Hirakata, Osaka, Japan.
DOI:10.25259/SNI_342_2024
Copyright: © 2024 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Satoshi Aihara1, Takeshi Umegaki1, Takehiro Soeda1, Haruka Iwamura, Junichi Takeda2, Masahiro Nonaka2, Takahiko Kamibayashi1. Cerebral vasospasm occurring immediately after endoscopic transsphenoidal resection of a pituitary adenoma: A case report. 14-Jun-2024;15:201
How to cite this URL: Satoshi Aihara1, Takeshi Umegaki1, Takehiro Soeda1, Haruka Iwamura, Junichi Takeda2, Masahiro Nonaka2, Takahiko Kamibayashi1. Cerebral vasospasm occurring immediately after endoscopic transsphenoidal resection of a pituitary adenoma: A case report. 14-Jun-2024;15:201. Available from: https://surgicalneurologyint.com/surgicalint-articles/12940/
Date of Submission
06-May-2024
Date of Acceptance
23-May-2024
Date of Web Publication
14-Jun-2024
Abstract
Background: Cerebral vasospasm is a rare postoperative complication of transsphenoidal pituitary adenoma surgery with potentially severe consequences. These vasospasms generally have a delayed presentation at a mean of 8 postoperative days. We report an unusual case of hyperacute onset of cerebral vasospasm that occurred immediately after surgery.
Case Description: A 38-year-old man underwent endoscopic transsphenoidal surgery for a nonfunctioning pituitary adenoma. The patient experienced mild subarachnoid hematoma during surgery. Three hours after surgery, he developed rightward conjugate eye deviation and complete paralysis of the left upper and lower extremities. Diagnostic imaging revealed cerebral vasospasm in both middle cerebral arteries, and symptoms improved after intra-arterial administration of fasudil hydrochloride.
Conclusion: There is a need for prompt diagnosis and therapeutic intervention when typical symptoms of cerebral vasospasm, such as paralysis, occur at any time during the postoperative course.
Keywords: Pituitary adenoma, Transsphenoidal surgery, Vasospasm
INTRODUCTION
Cerebral vasospasm is a rare postoperative complication of transsphenoidal pituitary adenoma surgery with potentially severe consequences and can present as neurological deterioration such as hemiparesis, impaired consciousness, and cranial nerve neuropathy.[
CASE PRESENTATION
A 38-year-old Japanese man (height: 168 cm; weight: 76.2 kg) with a history of hypertension presented to Kansai Medical University Hospital with the chief complaint of bitemporal hemianopsia. Magnetic resonance imaging (MRI) revealed a large 3.8-cm mass in the sella turcica. The patient was diagnosed with a nonfunctioning pituitary adenoma, and endoscopic transsphenoidal resection was scheduled. Surgery was performed under general anesthesia, which was induced and maintained with total intravenous anesthesia. Although irregular surgical procedures and surgical maneuvers for hypothalamus, intraoperative complications included mild cerebrospinal fluid leak and slight bleeding from the tumor dripped into the arachnoid and resulting in mild subarachnoid hematoma. After surgery, the patient was extubated in the operating room. The patient exhibited a relatively low level of consciousness during emergence from anesthesia. Total anesthesia time was 5 h 9 min, operative time was 3 h 33 min, and intraoperative blood loss was 250 mL.
A computed tomography (CT) scan of the patient’s head was performed after he left the operating room, which confirmed that a mild subarachnoid hematoma had occurred [

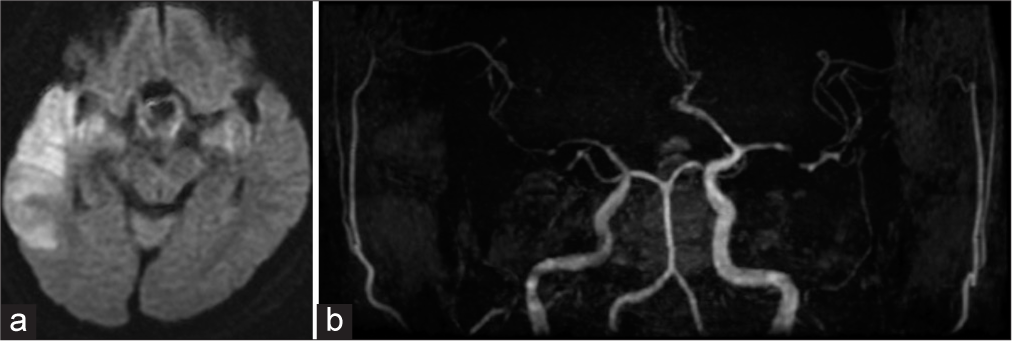
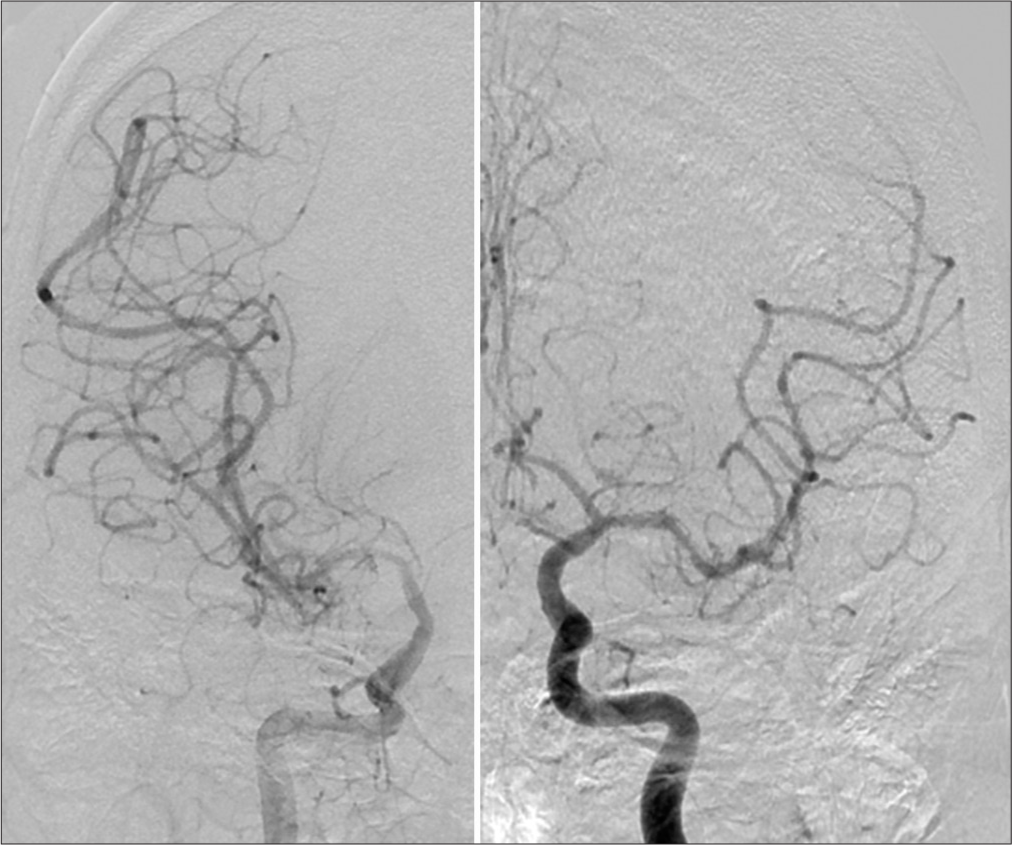
Emergency angiography was performed, which confirmed vasospasm in the M1-M2 segments of the right middle cerebral artery territory and the M1 segment of the left middle cerebral artery territory [

DISCUSSION
Postoperative complications of transsphenoidal pituitary adenoma surgery include infection, epistaxis, sinonasal complications, cerebrospinal fluid leak, electrolyte imbalance, hormonal disturbance, and vascular injuries.[
Several pathogenic mechanisms for cerebral vasospasms have been proposed, such as direct vascular injury and damage to the arachnoid layer leading to the leakage of blood into the subarachnoid layer, cerebrospinal fluid rhinorrhea, and meningitis.[
At present, there are no established general treatments for cerebral vasospasm after transsphenoidal pituitary adenoma surgery, and treatment strategies follow the same principles as the management of vasospasm following aneurysmal subarachnoid hemorrhage. These strategies include monitoring and controlling blood volume, ruling out infections and seizures, correcting electrolyte imbalance, and endovascular treatment.[
CONCLUSION
This report described a rare case of cerebral vasospasm – a usually delayed complication – in the hyperacute phase 3 h after transsphenoidal pituitary adenoma surgery. Regardless of patient age, intraoperative subarachnoid hemorrhage followed by typical symptoms such as paralysis occurring at any time during the postoperative course requires prompt diagnosis and therapeutic intervention.
Availability of data and materials
Not applicable.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Alzhrani G, Sivakumar W, Park SM, Taussky P, Couldwell WT. Delayed complications after transsphenoidal surgery for pituitary adenomas. World Neurosurg. 2018. 109: 233-41
2. Chhabra R, Singh A, Salunke P, Virk R. Unusual presentation of vasospasm masking underlying pseudoaneurysm after endoscopic transsphenoidal surgery in pituitary macroadenoma. World Neurosurg. 2019. 131: 163-5
3. Eseonu CI, ReFaey K, Geocadin RG, Hinojosa AQ. Postoperative cerebral vasospasm following transsphenoidal pituitary adenoma surgery. World Neurosurg. 2016. 92: 7-14
4. Molina ES, Somma DA, Stummer W, Briganti F, Cavallo LM. Clinical vasospasm after an extended endoscopic endonasal approach for recurrent pituitary adenoma: Illustrative case and systematic review of the literature. World Neurosurg. 2019. 128: 29-36
5. Popugaev KA, Savin IA, Lubnin AU, Gorachev AS, Kadashev BA, Kalinin PL. Unusual cause of cerebral vasospasm after pituitary surgery. Neurol Sci. 2011. 32: 673-80

