

- Department of Neuroscience and Reproductive and Dental Sciences, Division of Neurosurgery, Azienda Ospedaliera Universitaria Federico II, Naples Napoli, Italy.
- Department of Neurosurgery, IRCCS Neuromed, Pozzilli, Italy.
- Department of Neuroradiology, IRCCS Neuromed, Pozzilli, Italy.
Correspondence Address:
Valentina Pizzuti, Department of Neurosurgery, IRCCS Neuromed, Pozzilli, Italy.
DOI:10.25259/SNI_343_2022
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Ciro Mastantuoni1, Valentina Pizzuti2, Francesco Ricciardi2, Alessandro D’Elia2, Settimio Leonetti2, Claudio Colonnese3, Gualtiero Innocenzi2. Cervical spine arachnoid cyst complicated by spontaneous intracystic hemorrhage: Case report and review of the literature. 23-Sep-2022;13:427
How to cite this URL: Ciro Mastantuoni1, Valentina Pizzuti2, Francesco Ricciardi2, Alessandro D’Elia2, Settimio Leonetti2, Claudio Colonnese3, Gualtiero Innocenzi2. Cervical spine arachnoid cyst complicated by spontaneous intracystic hemorrhage: Case report and review of the literature. 23-Sep-2022;13:427. Available from: https://surgicalneurologyint.com/surgicalint-articles/11891/
Date of Submission
11-Apr-2022
Date of Acceptance
20-Apr-2022
Date of Web Publication
23-Sep-2022
Abstract
Background: Spinal intradural extramedullary arachnoid cysts represent about 1–3% of all primary spinal space-occupying lesions often causing spinal cord and/or radicular nerve compression. Spontaneous intralesional hemorrhages are extremely rare and are typically found within intracranial arachnoid cysts. Here, a 55-year-old female presented with a spontaneous hemorrhage into a cervical spine arachnoid cyst warranting surgical intervention (i.e., fenestration/excision/occlusion).
Case Description: A 55-year-old female presented with 3 weeks of dull pain in the cervicothoracic region. She subsequently developed paresthesias and progressive lower extremity weakness with (urinary incontinence. The cervical magnetic resonance revealed a right anterolateral intradural extramedullary “cystic” lesion extending from C7 to T2; it contained a heterogeneous signalon T2W sequences, and a fluid-fluid level was documented on the T2-GRE and FLAIR sequences. At surgery, consisting of a laminectomy, two hemorrhagic cystic lesions were identified and removed. Histological findings were consistent with hemorrhagic into an arachnoid cyst.
Conclusion: Only rarely hemorrhages develop in intraspinal intradural extramedullary spinal arachnoid cysts.
Keywords: Case report, Cavernomas, Cervical spine, Intracystic hemorrhage, Spine arachnoid cyst
INTRODUCTION
Spinal intradural extramedullary arachnoid cysts account for about 1–3% of all primary spinal space-occupying lesions, (i.e., sub-group III Nabors classification).[
CASE DESCRIPTION
A 55-year-old female presented with 3 weeks of dull cervicothoracic pain, accompanied by lower extremity paresthesia (right >left), progressive weakness (right 0/5; left 1/5), and urinary incontinence. The cervicothoracic magnetic resonance imaging (MRI) studies showed an anteroateral intradural extramedullary cystic lesion extending from C7 to T2 resulting in the left posterolateral shift of the spinal cord. A hemorrhagic cystic lesion was strongly suspected when the T1W sequences showed an hyperintense anterior component and a posterior cerebrospinal fluid (CSF)-isointense area. Contrariwise, the anterior component was isointense to CSF and the posterior one was hyperintense T2W-Flair sequences. Further, the GRE-T2W sequences revealed a fluid-fluid level, namely, an hypointense line dividing the different components and identifying the presence of hemosiderin, and the lesion did not enhance with contrast [
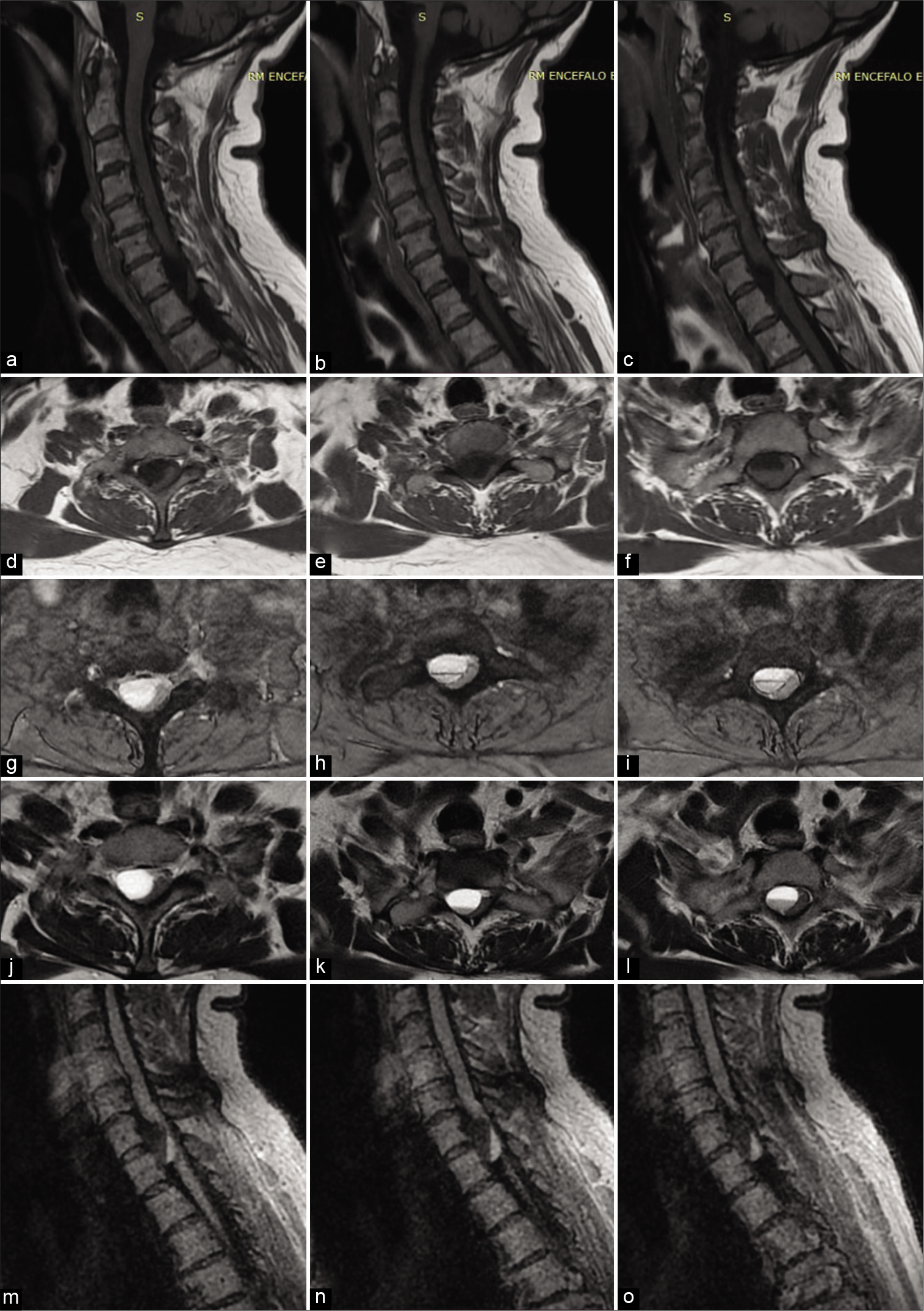
Figure 1:
(a, b, c) Sagittal T1W MRI shows a lesion extending from C7 to T2 with an hyperintense anterior component and a posterior CSF-isointense area; d, e, f) axial T1W MRI shows the right anterolateral extra-axial cystic lesion determining left posterolateral shift of the spinal cord; g, h, i) axial GRE-T2W sequences detect fluid-fluid level: an hypointense line divides two components of different intensity; j, k, l) axial T2W sequences show fluid-fluid level with anterior hyperintense and posterior hypointense components ; m, n, o) in Sagittal T2W-Flair sequences the anterior component results CSF-isointense and the posterior one is hyperintense.
Surgery
The patient underwent a C7-T1 laminectomy. The spinal cord was dorsolaterally displaced toward the left. On the right side, just below dentate ligament, a cystic lesion was found and opened; a second contiguous lesion was detected showing signs of recent bleeding and was removed en block [
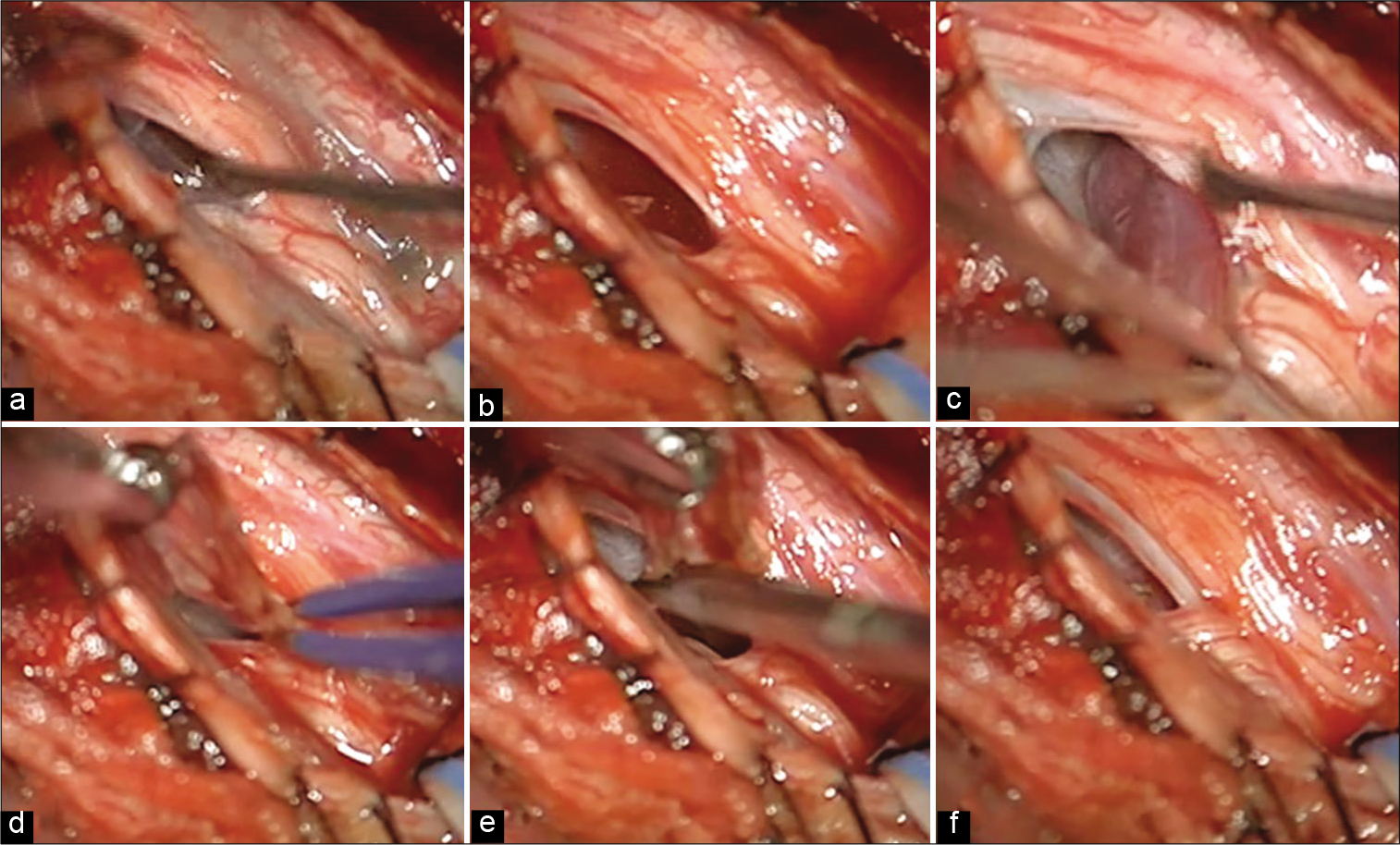
Figure 2:
Spinal cord appeared dorsally displaced (a). On the right side, just below dentate ligament, a cystic formation was opened, revealing a citrine fluid (b) below, a second lesion was detected, showing signs of recent bleeding (c). The lesion was coagulated (d) and removed en block (e). (f) If shows the surgical field after lesions removal.
Postoperative course
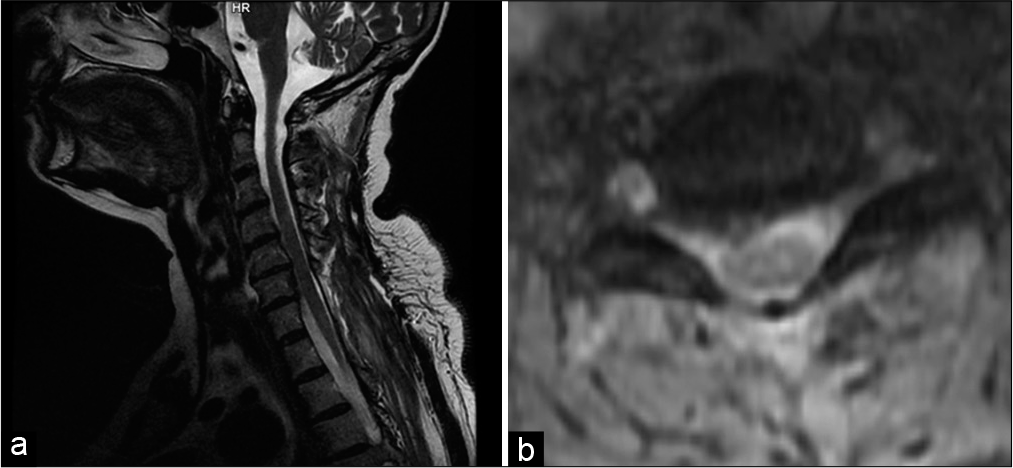
Three months after surgery, her lower extremity strength improved to 3/5 and hypoesthesias/sensory deficits resolved, along with normal sphincter functions. The follow-up cervical MR revealed no residual lesion [
Pathology
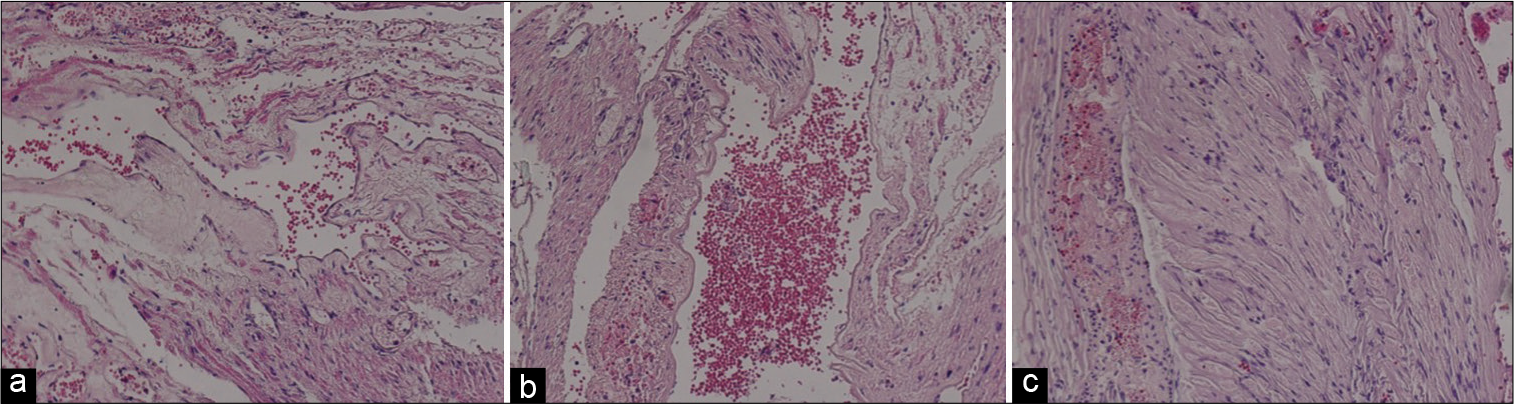
The pathology was consistent with a hemorrhagic arachnoid cyst [
DISCUSSION
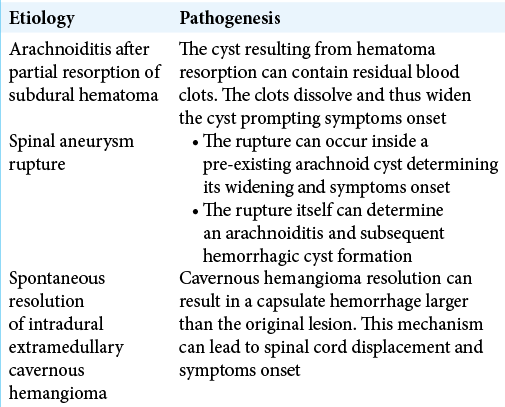
Spinal arachnoid cysts are mostly located at thoracic level followed by lumbosacral and cervical spine segments. They are often placed dorsally to the spinal cord, excepted in the Cavernous hemangioma resolution can result in a capsulate hemorrhage larger than the original lesion. This mechanism can lead to spinal cord displacement and symptoms onset cervical spine where they are more often ventral.[
MRI of spinal arachnoid cysts
On MRI, spinal arachnoid cysts have CSF intensity in T1W sequences but on T2W studies, they may have either CSF intensity or may be even brighter since there is no signal loss from pulsation/flow. They typically demonstrate no contrast-enhancement and on DWI studies, showing no evidence of restricted diffusion.[
Treatment of symptomatic spinal arachnoid cysts
Select symptomatic spinal arachnoid cysts may warrant surgery, especially if an acute hemorrhage had results in rapid neurological impairment. Surgical techniques variously include decompressive procedures with cyst fenestration, resection, occlusion of communication with the subarachnoid space, and/or cyst-peritoneal shunts.[
CONCLUSION
Herein, we report a spontaneous C7-T2 intra spinal hemorrhagic arachnoid cyst resulting in subacute cord compression that resolved following a decompressive laminectomy with cyst excision.
Declaration of patient consent
Patient’s consent not required as patient’s identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Fam MD, Woodroffe RW, Helland L, Noeller J, Dahdaleh NS, Menezes AH. Spinal arachnoid cysts in adults: Diagnosis and management. A single-center experience. J Neurosurg Spine. 2018. 29: 711-9
2. Fukumoto H, Samura K, Katsuta T, Miki K, Fukuda K, Inoue T. Extensive multilocular spinal extradural meningeal cyst that developed 16 years after traumatic brachial plexus injury: A case report. World Neurosurg. 2016. 86: 510.e5-10
3. Golnari P, Ansari SA, Shaibani A, Hurley MC, Potts MB, Kohler ME. Intradural extramedullary cavernous malformation with extensive superficial siderosis of the neuraxis: Case report and review of literature. Surg Neurol Int. 2017. 8: 109
4. Hong JC, Kim MS, Chang CH, Kim SH. Arachnoid cyst with spontaneous intracystic hemorrhage and chronic subdural hematoma. J Korean Neurosurg Soc. 2008. 43: 54-6
5. Kadono Y, Yuguchi T, Ohnishi Y, Iwatsuki K, Yoshimine T. A symptomatic spinal extradural arachnoid cyst with lumbar disc herniation. Case Rep Orthop. 2015. 2015: 250710
6. Kieu HD, Le TD, Tran TQ. Arachnoid cyst with spontaneous intracystic hemorrhage and associated chronic subdural hematoma: A case report. Int J Surg Case Rep. 2021. 81: 105789
7. Paramore CG. Dorsal arachnoid web with spinal cord compression: Variant of an arachnoid cyst? Report of two cases. J Neurosurg. 2020. 93: 287-90
8. Schmutzer M, Tonn JC, Zausinger S. Spinal intradural extramedullary arachnoid cysts in adults-operative therapy and clinical outcome. Acta Neurochir (Wien). 2020. 162: 691-702

