

- Department of Neurosurgery, Kesennuma City Hospital, Kesennuma, Miyagi, Japan.
- Department of Rehabilitation, Kesennuma City Hospital, Kesennuma, Miyagi, Japan.
Correspondence Address:
Norio Narita
Department of Rehabilitation, Kesennuma City Hospital, Kesennuma, Miyagi, Japan.
DOI:10.25259/SNI_186_2021
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Masahito Katsuki1, Iori Yasuda1, Norio Narita1, Dan Ozaki1, Yoshimichi Sato1, Yuya Kato1, Wenting Jia1, Taketo Nishizawa1, Ryuzaburo Kochi1, Kanako Sato1, Kokoro Kawamura1, Naoya Ishida1, Ohmi Watanabe1, Siqi Cai1, Shinya Shimabukuro1, Kenichi Yokota2. Chronic subdural hematoma in patients over 65 years old: Results of using a postoperative cognitive evaluation to determine whether to permit return to driving. 10-May-2021;12:212
How to cite this URL: Masahito Katsuki1, Iori Yasuda1, Norio Narita1, Dan Ozaki1, Yoshimichi Sato1, Yuya Kato1, Wenting Jia1, Taketo Nishizawa1, Ryuzaburo Kochi1, Kanako Sato1, Kokoro Kawamura1, Naoya Ishida1, Ohmi Watanabe1, Siqi Cai1, Shinya Shimabukuro1, Kenichi Yokota2. Chronic subdural hematoma in patients over 65 years old: Results of using a postoperative cognitive evaluation to determine whether to permit return to driving. 10-May-2021;12:212. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=10802
Date of Submission
22-Feb-2021
Date of Acceptance
08-Apr-2021
Date of Web Publication
10-May-2021
Abstract
Background: Chronic subdural hematoma (CSDH) is usually associated with good recovery with burr hole irrigation and postoperative drainage under local anesthesia. In Japan, traffic accidents by the elderly drivers over 65 years old are severely increasing, and there is no consensus on whether or not to return to driving after CSDH treatment. We perform a postoperative cognitive assessment. We retrospectively investigated the return-to-driving rate and associated factors.
Methods: Of the 45 patients over 65 y.o. and who had usually driven, 30 patients wished to drive again. We performed tests composed of Mini-Mental State Examination (MMSE), line cancellation and line bisection task, Kohs block design test, trail making test (TMT)-A and B, Kana-hiroi test, Rey-Osterrieth complex figure test, and behavioral assessment of the dysexecutive syndrome, in order. When all tests’ scores were better than the cutoff values, we let patients drive again. When some of the scores were worse than the cutoff values, we reevaluated the patients at the outpatient every month. If the patients’ scores could not improve at the outpatient, we recommended them to stop driving.
Results: Nineteen of 30 patients could return to driving. Worse MMSE, Kohs block design test, TMT-A, TMT-B scores, higher age, dementia, or consciousness disturbance as chief complaints were associated with driving disability.
Conclusion: CSDH is known as treatable dementia. However, we should perform an objective cognitive assessment before discharge because only 63% of the patients over 65 y.o. who wished to drive could return to driving.
Keywords: Chronic subdural hematoma, Cognitive assessment, Dementia, Elderly, Higher brain dysfunction
INTRODUCTION
Chronic subdural hematoma (CSDH) is one of the most common diseases seen by neurosurgeons. It is usually associated with good recovery with burr hole irrigation and postoperative drainage under local anesthesia.[
We work in a rural area in Japan with 37% of elderly population. We should prevent traffic accidents by elderly CSDH patients from happening after discharge. We have a few medical staff and many elderly patients, and the hospitalization term is short in CSDH patients. Therefore, we perform a simple cognitive assessment during hospitalization for elderly CSDH patients who want to drive after discharge. We retrospectively investigated the return-to-driving rate after CSDH treatment at our hospital and what factors were associated with return-to-driving. This is a unique investigation on the association between elderly CSDH patients’ cognitive function and return-to-driving rate.
MATERIALS AND METHODS
Study population
This retrospective study included 121 consecutive CSDH patients treated between 2017 and 2020 in our hospital. We usually performed burr hole, irrigation, and drainage surgery under local anesthesia. However, we sometimes used neuroendoscopy and suction cannula to penetrate the septum in the hematoma cavity so that the CSDH was not divided into compartments by the septum and that efflux of the hematoma could be achieved.[
Our hospital’s research ethics committee approved the study, and we gained written informed consent for this study from all of the patients, the legally authorized representative of the patients, or the next of kin of the deceased patients. All methods were carried out in accordance with relevant guidelines and regulations (Declaration of Helsinki). All personal patient information were deleted from the database for this study to protect patient privacy.
Cognitive assessment
We postoperatively performed the simple cognitive assessment composed of seven tests, including Mini-Mental State Examination (MMSE), line cancellation and line bisection task, Kohs block design test, trail making test (TMT)-A and B, Kana-hiroi test, Rey-Osterrieth complex figure test, and behavioral assessment of the dysexecutive syndrome, in order. The cutoff values are shown in [
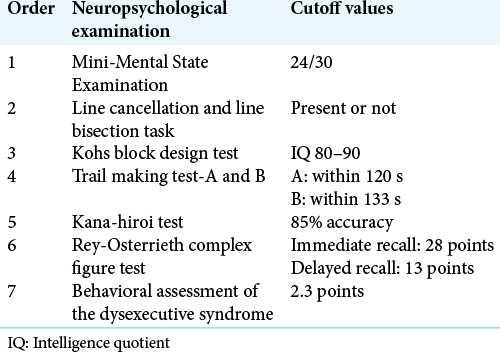
First, patients with MMSE score under 24/30 or unilateral spatial neglect evaluated by line cancellation and line bisection task were recommended to stop driving. Then, we performed other tests in order. When all tests’ scores were better than the cutoff values, we let patients drive again. When some of the scores were worse than the cutoff values, we reevaluated the patients at the outpatient every month, and if the patients’ cognitive function improved superior to the cutoff values, we let them drive again. If the patients’ scores could not improve at the outpatient, we recommend them to stop driving and to consult the police station if they wanted to drive.
Regarding patients who did not wish to drive, who were physically unable to drive due to comorbidities like fractures and wish to stop driving, or who were prohibited from driving by family members, the cognitive assessment was stopped as appropriate.
Outcome and variables
The outcome was whether the patient eventually could return to driving or not. We also investigated the age, sex, chief complaint, presence of hypertension, diabetes mellitus, and dyslipidemia that are now treated, atrial fibrillation, habitual smoking, and habitual alcohol consumption. Laboratory data, including levels of total protein, albumin, triglycerides, total cholesterol, high- and low-density lipoprotein cholesterol, white blood cell count, hemoglobin level, and lymphocyte count, were also investigated. These are related to nutrition status, and some are related to the neurosurgical diseases’ outcomes.[
Statistical analysis
To assess the association between the outcome and variables described above, we used the Mann–Whitney U-test, Fisher’s exact test, or Pearson’s Chi-square test adequately. Continuous variables were summarized as median (interquartile range). A two-tailed P < 0.05 was considered statistically significant. We conducted these calculations using SPSS software version 24.0.0. (IBM, New York, USA).
RESULTS
Clinical characteristics
All patients’ surgical procedures were successfully completed, and all the symptoms were improved after surgery. Among the 121 CSDH patients (median age 81, interquartile range 74–86, 41 women and 80 men), 10 patients were under 65 years old, and all passed the cognitive assessment. Among the 111 patients over 65 years old, 66 patients (59%) had already quit driving before admission. Among the 45 patients (41%) who had usually driven, 15 patients (33%) did not wish to drive or could not drive due to other comorbidities. Therefore, the rest of the 30 patients (67%) who wished to drive were assessed on driving ability [
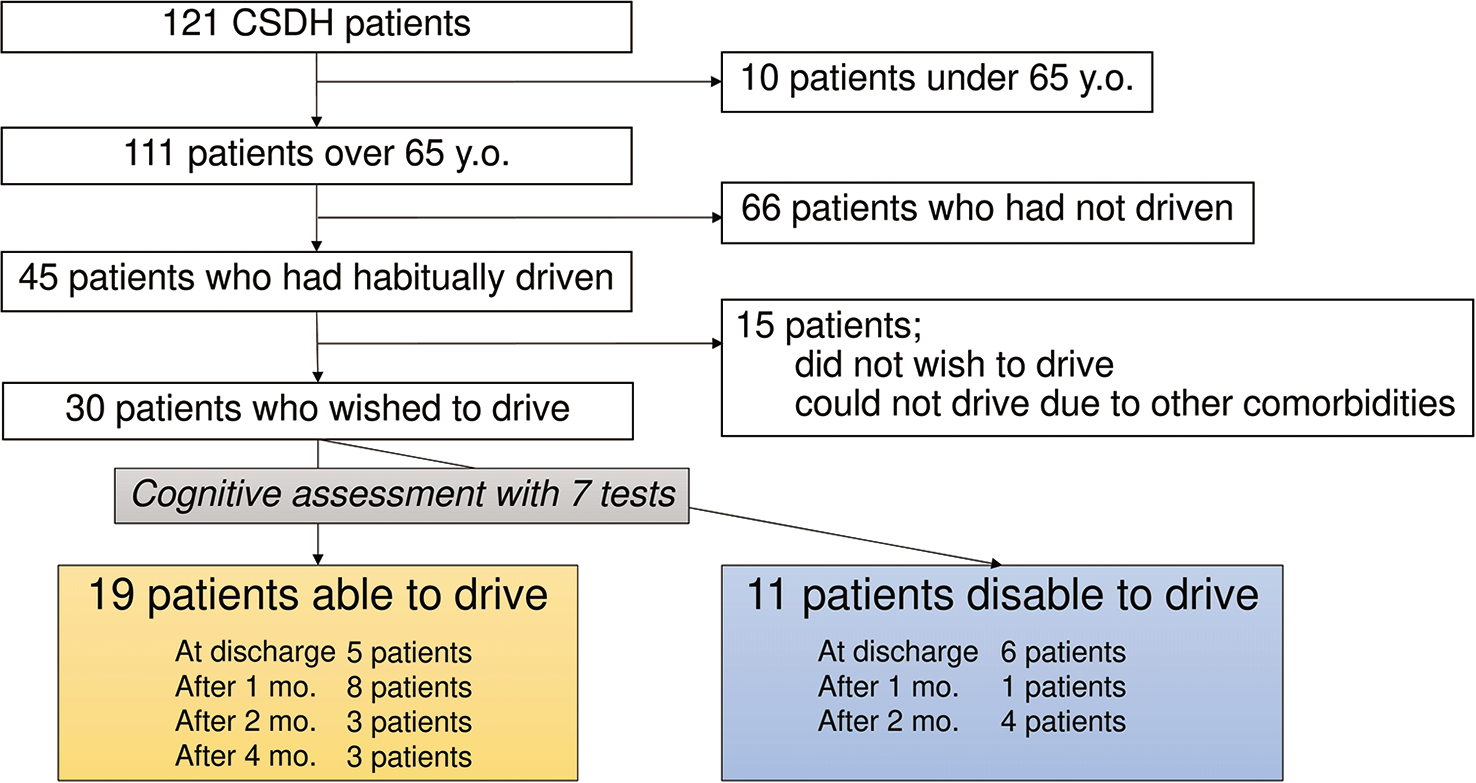
Figure 1:
Among the 121 CSDH patients (median age 81, interquartile range 74–86, 41 women and 80 men), 10 patients were under 65 years old, and all passed the cognitive assessment. Among the 111 patients over 65 years old, 66 patients had already quit driving before admission. Among the 45 patients who had usually driven, 15 patients did not wish to drive or could not drive due to other comorbidities. Therefore, the rest of the 30 patients who wish to drive were assessed on driving ability. Then, 19 patients could return to driving eventually, and 11 could not. Five patients could return to driving at discharge, eight after 1 month, three after 2 months, and three after 4 months. Six patients were judged as disable to drive at discharge, one after 1 month, and four after 2 months.
Clinical characteristics of the 30 CSDH patients who wished to drive (8 women and 22 men) are summarized in [

After cognitive assessment, 19 patients could return to driving eventually, and 11 could not. Five patients could return to driving at discharge, eight after 1 month, three after 2 months, and three after 4 months. Six patients were judged as disable to drive at discharge, one after 1 month, and four after 2 months [
Relationship between outcome and variables
We performed the Mann–Whitney U-test, Fisher’s exact test, and Pearson’s Chi-square test. Lower MMSE score and worse TMT-A score were significantly related to driving disability (P < 0.001, P = 0.046, each). Higher age, dementia or disturbance of consciousness as chief complaints, and worse Kohs block design test and TMT-B scores were also associated with driving disability, though they were not statistically significant (P = 0.064, 0.077, 0.051, and 0.087, respectively) [
DISCUSSION
We herein report 111 CSDH patients over 65 years old, and 45 of 111 patients had usually driven. Eventually, only 19 patients could return to driving, and 15 or 11 patients did not wish to drive or could not return to driving. Higher age, dementia or disturbance of consciousness as chief complaints, lower MMSE, worse Kohs block design test, and TMT-A and B scores were associated with driving disability. This is the first report on whether elderly CSDH patients could return to driving or not in Japan. CSDH is known as treatable dementia. However, our results suggest that we should perform an objective cognitive assessment before discharge because only 63% of the patients could return to driving.
Road traffic laws in Japan
In the road traffic law, dementia is a disease specified as a requirement for restricting driving licenses from 2002. “Dementia” in this context is defined as “dementia with no hope of cure,” and it is ambiguous whether CSDH is included or not. Furthermore, as for the higher brain dysfunction, it is stated that “the license shall be revoked in accordance with the provisions on dementia,” and the criteria are still vague.[
In this unclear and complex context, when CSDH patients consult the police officers, they must let doctors make medical certificates describing whether or not the cognitive function is expected to recover within 6 months. If the patient submits a medical certificate stating that they are expected to recover, the police will evaluate cognitive and driving functions and make a final decision after 6 months.[
In Japan, “memory and judgment function tests” are conducted every 3 years for elderly drivers over 75 years old by the National Police Agency, but not for those under 75 years old.[
CSDH and cognitive function
From the Japanese epidemiological study on CSDH, the overall incidence of CSDH was 20.6/100,000/year in all age groups, and the mean ± standard deviation of age was 71.2 ± 12.8 years old. Furthermore, the incidence was 80.1/100,000/ year in people over 65 years of age.[
Some report describes that treatable dementia accounts for 8%, and CSDH is 0.4% of all the dementia outpatients.[
Cognitive assessment
A composite cognitive battery is likely to be better than testing single cognitive domains in assessing fitness to drive in patients with dementia.[
MMSE is a typical test for dementia, not to mention its importance to whether or not one can drive.
Kohs block design test is an intelligence quotient test with creating 17 different patterns by combining wooden cubes of 3 cm on a side. Kohs block design test is thought to reflect spatial cognitive ability.[
TMT requires tracing numbers and alphabets (hiragana in the Japanese version) alternately in ascending order, so it requires various abilities such as recognition of numbers and letters, mental flexibility, attention span, visual search, visual motility, and coordination of hand movement and vision.[
Our cognitive assessment consists of seven tests, but these results suggest that our cognitive assessment for CSDH can be simplified into 3–5 tests, including MMSE, Kohs block design test, and TMT, leading to saving the medical and time resources. Further studies are desired.
Limitations
First, the sample size was small, and we performed only univariate analysis. We should continue to study with large samples and perform multivariate analysis. Second, we should have investigated the patients’ psychological status after the judgment of driving disability because driving is needed in this rural area. The patients and their families’ burden might have become severe. Third, the cutoff values and the number of tests should be reconsidered. Our cognitive assessment is relatively simple and could be performed by a few medical staff in the short-term hospitalization. However, overestimating and restricting driving could lead to patient frustration and worsen the quality of lives, while underestimating might lead to causing accidents. Fourth, it is unclear whether the cognitive function deteriorated due to CSDH itself or whether it had already got worse preoperatively.
CONCLUSION
CSDH is known as treatable dementia. However, we should perform an objective cognitive assessment before discharge because only 63% of the patients who wished to drive could return to driving.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Almenawer SA, Farrokhyar F, Hong C, Alhazzani W, Manoranjan B, Yarascavitch B. Chronic subdural hematoma management: A systematic review and meta-analysis of 34,829 patients. Ann Surg. 2014. 259: 449-57
2. Special Feature: “Preventing Traffic Accidents Involving the Elderly” I. Available from: https://www8.cao.go.jp/koutu/taisaku/h29kou_haku/gaiyo/features/feature01.html [Last accessed on 2021 Jan 04].
3. Egeto P, Badovinac SD, Hutchison MG, Ornstein TJ, Schweizer TA. A systematic review and meta-analysis on the association between driving ability and neuropsychological test performances after moderate to severe traumatic brain injury. J Int Neuropsychol Soc. 2019. 25: 868-77
4. Hori C, Koura A, Ota T. Comparison of neuropsychological and driving simulator test results between the allowed and withheld/ unallowed driving groups for people with higher brain dysfunction. Ishikawa Sagyo Ryoho Gakujutsu Zasshi. 2019. 28: 31-5
5. de Ulíbarri JI, González-Madroño A, de Villar NG, González P, González B, Mancha A. CONUT: A tool for controlling nutritional status. First validation in a hospital population. Nutr Hosp. 2005. 20: 38-45
6. Ishikawa E, Yanaka K, Sugimoto K, Ayuzawa S, Nose T. Reversible dementia in patients with chronic subdural hematomas. J Neurosurg. 2002. 96: 680-3
7. Ivamoto HS, Lemos HP, Atallah AN. Surgical treatments for chronic subdural hematomas: A comprehensive systematic review. World Neurosurg. 2016. 86: 399-418
8. Indication and Judgment of Cine-Psychological Testing Methods in Cases of Suspected Higher Brain Dysfunction due to Stroke, Brain Trauma, Etc. Available from: https://www.higherbrain.or.jp/07_osirase/img/20200301_pub2.pdf [Last accessed on 2021 Jan 09].
9. Karibe H, Kameyama M, Kawase M, Hirano T, Kawaguchi T, Tominaga T. Epidemiology of chronic subdural hematomas. No Shinkei Geka. 2011. 39: 1149-53
10. Katayama K, Matsuda N, Kakuta K, Naraoka M, Takemura A, Hasegawa S. The effect of goreisan on the prevention of chronic subdural hematoma recurrence: Multi-center randomized controlled study. J Neurotrauma. 2018. 35: 1537-42
11. Katsuki M, Fujimura M, Tashiro R, Tomata Y, Nishizawa T, Tominaga T. Pre-operative higher hematocrit and lower total protein levels are independent risk factors for cerebral hyperperfusion syndrome after superficial temporal artery-middle cerebral artery anastomosis with pial synangiosis in adult moyamoya disease patients-case-control study. Neurosurg Rev. 2020. 2020: 01395
12. Katsuki M, Kakizawa Y, Nishikawa A, Yamamoto Y, Uchiyama T. Lower total protein and absence of neuronavigation are novel poor prognostic factors of endoscopic hematoma removal for intracerebral hemorrhage. J Stroke Cerebrovasc Dis. 2020. 29: 105050
13. Katsuki M, Kakizawa Y, Wada N, Yamamoto Y, Uchiyama T, Nakamura T. Endoscopically observed outer membrane color of chronic subdural hematoma and histopathological staging: White as a risk factor for recurrence. Neurol Med Chir (Tokyo). 2020. 60: 126-35
14. Katsuki M, Narita N, Matsumori Y, Ishida N, Watanabe O, Cai S. Kampo (Japanese herbal) medicine for primary headache as an acute treatment a retrospective investigation in Kesennuma city hospital during five years. J Neurosurg Kampo Med. 2022. 7:
15. Katsuki M, Narita N, Sasaki K, Sato Y, Suzuki Y, Mashiyama S. Standard values for temporal muscle thickness in the Japanese population who undergo brain check-up by magnetic resonance imaging. Surg Neurol Int. 2021. 12: 67
16. Katsuki M, Suzuki Y, Kunitoki K, Sato Y, Sasaki K, Mashiyama S. Temporal muscle as an indicator of sarcopenia is independently associated with hunt and kosnik grade on admission and the modified rankin scale score at 6 months of patients with subarachnoid hemorrhage treated by endovascular coiling. World Neurosurg. 2020. 137: e526-34
17. Katsuki M, Suzuki Y, Kunitoki K, Sato Y, Sasaki K, Mashiyama S. Temporal muscle thickness and area with various characteristics data of the patients with aneurysmal subarachnoid hemorrhage who underwent endovascular coiling. Data Brief. 2020. 31: 105715
18. Katsuki M, Yamamoto Y, Uchiyama T, Nishikawa A, Wada N, Kakizawa Y. Temporal muscle thickness and area with various characteristics data of the elderly patients over 75 with aneurysmal subarachnoid haemorrhage whose World Federation of Neurosurgical Societies grade were I to III. Data Brief. 2020. 28: 104832
19. Katsuki M, Yamamoto Y, Uchiyama T, Wada N, Kakizawa Y. Clinical characteristics of aneurysmal subarachnoid hemorrhage in the elderly over 75; would temporal muscle be a potential prognostic factor as an indicator of sarcopenia?. Clin Neurol Neurosurg. 2019. 186: 105535
20. Kawai N, Hatakeyama T, Tamiya T. The driver’s license knowledge required for daily neurosurgical practice (5) Resuming driving in patients with neuropsychological impairment after traumatic brain injury. No Shinkei Geka. 2020. 48: 1200-9
21. Kawamura T. Kampo medicine in neurosurgery. No Shinkei Geka. 2020. 48: 267-74
22. Knight RG, McMahon J, Green TJ, Skeaff CM. Regression equations for predicting scores of persons over 65 on the rey auditory verbal learning test, the mini-mental state examination, the trail making test and semantic fluency measures. Br J Clin Psychol. 2006. 45: 393-402
23. Liu W, Bakker NA, Groen RJ. Chronic subdural hematoma: A systematic review and meta-analysis of surgical procedures. J Neurosurg. 2014. 121: 665-73
24. Statistics and the Elderly in Japan. Available from: https://www.stat.go.jp/data/topics/pdf/topics126.pdf [Last accessed on 2021 Feb 22].
25. Mitrushina M.editors. Handbook of Normative Data for Neuropsychological Assessment. New York: Oxford University Press; 2005. p.
26. Nakamura M, Hitosugi M. The driver’s license knowledge required for daily neurosurgical practice (1) General remark. No Shinkei Geka. 2020. 48: 758-64
27. Cognitive Function Test Procedure for Driving. Available from: https://www.npa.go.jp/policies/application/license_renewal/ninti/sinkoyoryo.pdf [Last accessed on 2021 Mar 18].
28. Onodera H, Mogamiya T, Mori M, Matsushima S, Sase T, Nakamura H. High protein intake after subarachnoid hemorrhage improves ingestion function and temporal muscle volume. Clin Nutr ESPEN. 2020. 40: 595
29. Onodera HMogamiya TMatsushima SSase TKawaguchi KNakamura H. High protein intake after subarachnoid hemorrhage improves oral intake and temporal muscle volume. in press. Available: https://www.linkinghub.elsevier.com/retrieve/pii/S0261561421000674 [Last accessed on 2021 Feb 07].
30. Oyama H, Ueda M, Inoue S, Ikeda A, Shibuya M, Katsumata T. Improvement of cognition after trepanation for the chronic subdural hematoma. No To Shinkei. 1998. 50: 249-52
31. Piercy M, Hecaen H, de Ajuriaguerra. Constructional apraxia associated with unilateral cerebral lesions-left and right sided cases compared. Brain. 1960. 83: 225-42
32. Rashid R, Standen P, Carpenter H, Radford K. Systematic review and meta-analysis of association between cognitive tests and on-road driving ability in people with dementia. Neuropsychol Rehabil. 2020. 30: 1720-61
33. Steindl A, Leitner J, Schwarz M, Nenning KH, Asenbaum U, Mayer S. Sarcopenia in neurological patients: Standard values for temporal muscle thickness and muscle strength evaluation. J Clin Med. 2020. 9: 1272
34. Takada LT, Caramelli P, Radanovic M, Anghinah R, Hartmann AP, Guariglia CC. Prevalence of potentially reversible dementias in a dementia outpatient clinic of a tertiary university-affiliated hospital in Brazil. Arq Neuropsiquiatr. 2003. 61: 925-9
35. Toi H, Kinoshita K, Hirai S, Takai H, Hara K, Matsushita N. Present epidemiology of chronic subdural hematoma in Japan: analysis of 63,358 cases recorded in a national administrative database. J Neurosurg. 2018. 128: 222-8
36. Tsuboi K, Maki Y, Nose T, Matsuki T. Psychiatric symptoms of patients with chronic subdural hematoma. No Shinkei Geka. 1984. 12: 275-9
37. Yamamoto Y, Mimura M. (3)The elderly, dementia and automobile driving. No Shinkei Geka. 2020. 48: 973-8

