

- Department of Adult Neurosurgery, National Neuroscience Institute, King Fahed Medical City, Riyadh, Saudi Arabia,
- Division of Neurosurgery, Department of Surgery, King Abdulaziz Medical City, Ministry of the National Guard - Health Affairs, King Abdullah International Medical Research Center, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia,
- Department of Neurosciences, Division of Neurosurgery, King Faisal Specialist Hospital and Research Center, Riyadh, Saudi Arabia.
Correspondence Address:
Mohammed Bafaquh
Department of Adult Neurosurgery, National Neuroscience Institute, King Fahed Medical City, Riyadh, Saudi Arabia,
DOI:10.25259/SNI_188_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Mohammed Bafaquh1, Sami Khairy2, Mahmoud Alyamany1, Abdullah Alobaid1, Gmaan Alzhrani2, Ali Alkhaibary2, Wafa F. Aldhafeeri1, Areej A. Alaman2, Hanan N. Aljohani3, Basim Noor Elahi1, Fatimah A. Alghabban1, Yasser Orz1, Abdulrahman Y. Alturki1. Classification of internal carotid artery injuries during endoscopic endonasal approaches to the skull base. 21-Oct-2020;11:357
How to cite this URL: Mohammed Bafaquh1, Sami Khairy2, Mahmoud Alyamany1, Abdullah Alobaid1, Gmaan Alzhrani2, Ali Alkhaibary2, Wafa F. Aldhafeeri1, Areej A. Alaman2, Hanan N. Aljohani3, Basim Noor Elahi1, Fatimah A. Alghabban1, Yasser Orz1, Abdulrahman Y. Alturki1. Classification of internal carotid artery injuries during endoscopic endonasal approaches to the skull base. 21-Oct-2020;11:357. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=10338
Date of Submission
17-Apr-2020
Date of Acceptance
20-Jun-2020
Date of Web Publication
21-Oct-2020
Abstract
Background: Internal carotid artery (ICA) injuries are a major complication of endoscopic endonasal approaches (EEAs), which can be difficult to manage. Adding to the management difficulty is the lack of literature describing the surgical anatomical classification of these types of injuries. This article proposing a novel classification of ICA injuries during EEAs.
Methods: The classification of ICA injuries during EEAs was generated from the review of the literature and analysis of the main author observation of ICA injuries in general. All published cases of ICA injuries during EEAs in the literature between January 1990 and January 2020 were carefully reviewed. We reviewed all patients’ demographic features, preoperative diagnoses, modes of injury, cerebral angiography results, surgical and medical management techniques, and reported functional outcomes.
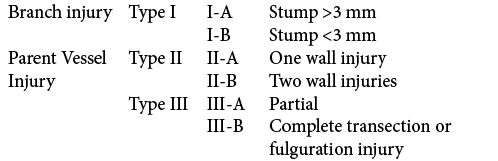
Results: There were 31 papers that reported ICA injuries during EEAs in the past three decades, most studies did not document the type of injury, and few described major laceration type of it. From that review of the literature, we classified ICA injuries into three main categories (Types I-III) and six sub-types. Type I is ICA branch injury, Type II is a penetrating injury to the ICA, and Type III is a laceration of the ICA wall. The functional neurological outcome was found to be worse with Type III and better with Type I.
Conclusion: This is a novel classification system for ICA injuries during EEAs; it defines the patterns of injury. It could potentially lead to advancements in the management of ICA injuries in EEAs and facilitate communication to develop guidelines.
Keywords: Classification, Endonasal, Endoscopic, Internal carotid artery, Injury
INTRODUCTION
Endoscopic endonasal approaches (EEAs) to skull-base lesions have been substantially advanced over the past three decades.[
Internal carotid artery (ICA) injuries are rare but can be catastrophic when they occur during EEAs.[
These differences in incidence result from the differences in surgical techniques, complexity of the approach, and size of the tumor.[
Unfortunately, the literature lacks a surgical anatomical classification for these injuries, and most publications only reported the mode of injury without detailed anatomical description of the injury.[
MATERIALS AND METHODS
A literature review of the MEDLINE database using the PubMed search engine was performed. All published cases of ICA injury during EEAs in the literature between January 1990 and January 2020 were thoroughly reviewed. Animal studies, simulation studies, and non-English studies were excluded from the study.
We reviewed all patients’ demographic features, preoperative diagnoses, modes of injury (when available), cerebral angiography results, surgical and medical management strategies, as well as the reported functional outcomes. From the collected data, the authors proposed a new classification system for these injuries. Three main factors were used to defined the three main types, first is the type of vessel injured (parent artery vs. a branch of the ICA); when the injury involves only a branch of the ICA the type of injury was named “branch injury” and it is classified as Type I. The second and third factors (apply to parent vessel injuries) are the cause and degree of the injury (sharp penetrated injury vs. laceration injury); when the injury involves a sharp penetration the type of injury is named “penetration injury” and is classified as Type II and when the injury is a tear in the three layer of the ICA wall it is named “laceration” and is classified as Type III.
Further factors were used to divide each type into two sub-types. For the “branch injury” (Type I); the distance of the stump from the ICA is an important factor, thus we divided this type further into branch injury with stump more than 3 mm or <3 mm, this is based on the fact that stumps of <3 mm are difficult to control with bipolar coagulation without further injury to or stenosis of the parent vessel; which is the main author observation. The second type (Type II) is a sharp penetration injury, which is further divided based on number of ICA walls involved; into single wall penetration or two-sided wall penetration “through and through” injury. The third type (Type III) was divided into two subtypes, partial laceration (including branch avulsion) or completes transection of the ICA wall with or without fulguration (burning contusion) of the wall of ICA [
RESULTS
The new classification
ICA injuries during EEAs were classified into three main types and six subtypes [
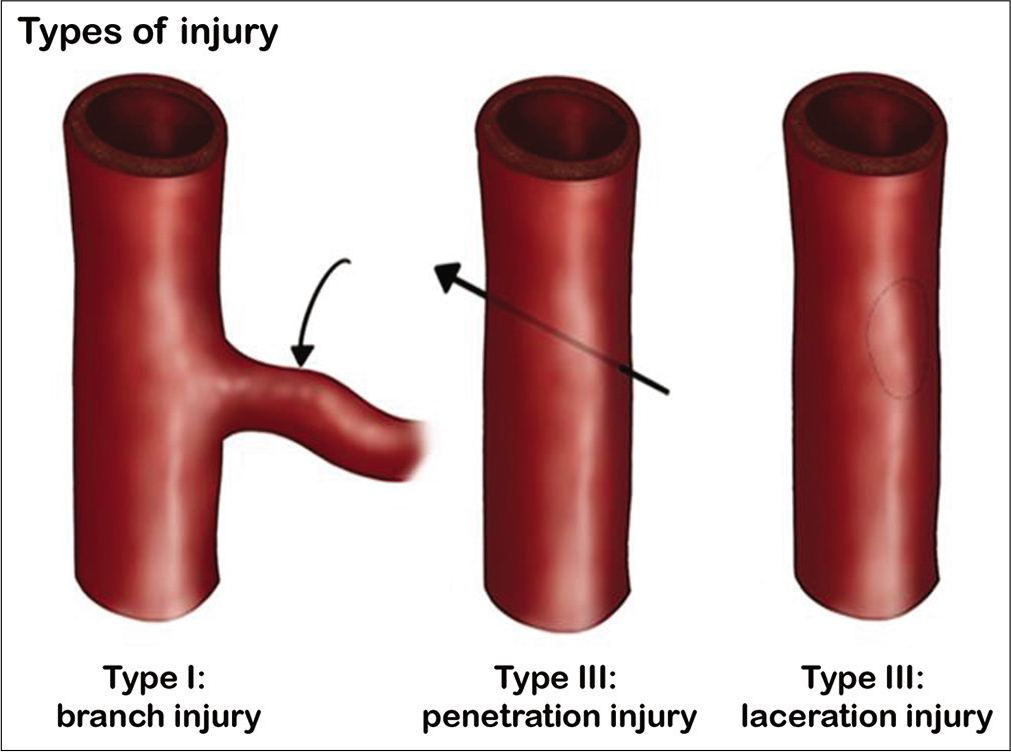
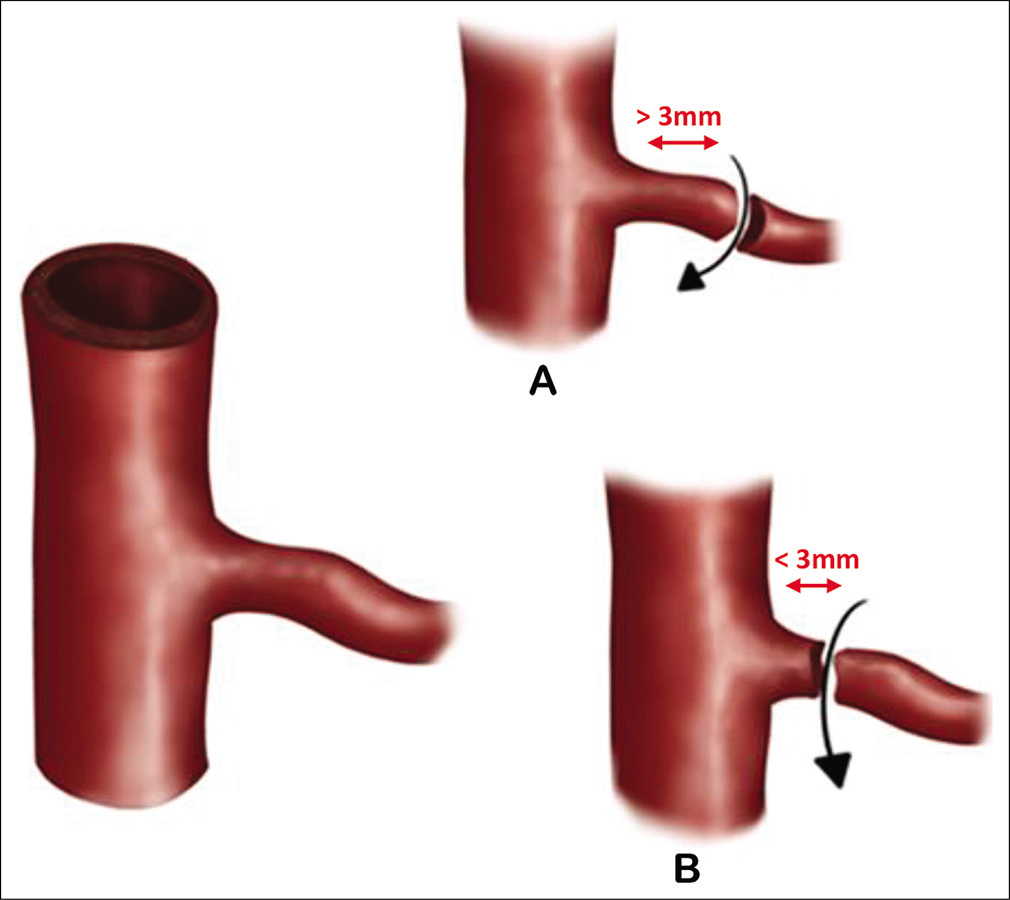
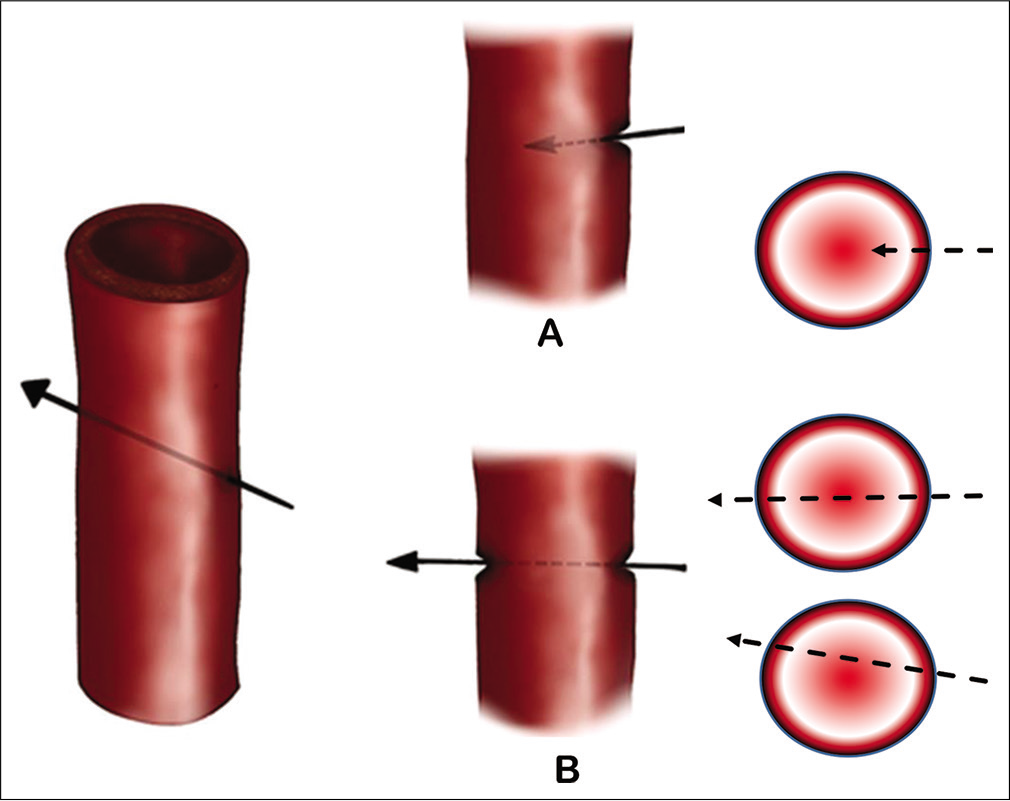
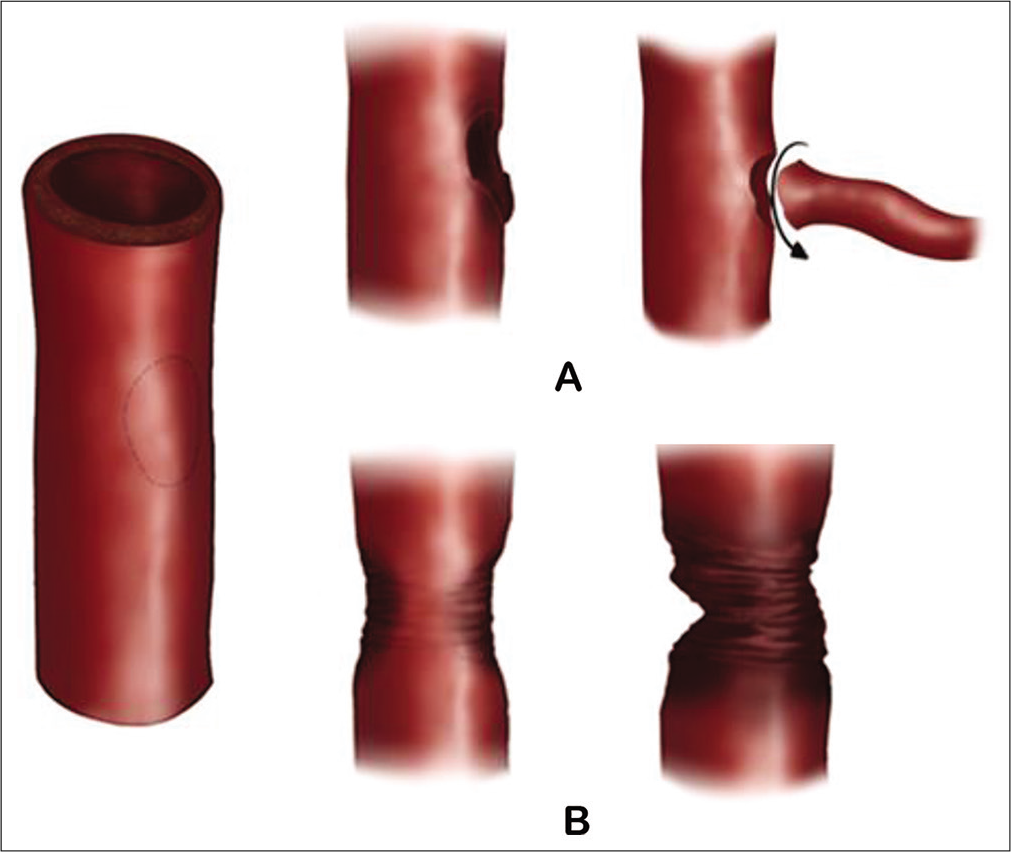
Figure 4:
Laceration injuries of the internal carotid artery (ICA). (A) True laceration typically caused by punch/pituitary instruments or branch avulsion-off the wall of- ICA. (B) Complete laceration that includes transection and fulguration (burn/contusion typically caused by aggressive coagulation of the ICA).
The outcome of the injury based on the proposed classification
The review of the literature revealed 31 papers that reported ICA injuries during EEAs to the ventral skull base. A total of 68 patients were reported in the literature with ICA injuries during EEAs. Type III injury was the most commonly reported in 27 patients and was associated with unfavorable outcomes. In the outcome of these injuries, a total of four patients died and five patients were reported to have neurological deficit, three of them were temporary deficits [
The “enough distance” of the stump is defined around 3 mm as most bipolar tip is around 2 mm, where the stump can be held by the bipolar tip and coagulated relatively safely, however, when the stump is <3 mm the comfort zone of controlling the bleed using bipolar coagulation is narrowed and might need different technique other than coagulation (e.g., aneurysmal clip) or other management such as endovascular intervention (flow diverters) after temporarily backing.
DISCUSSION
Injury to the ICA during EEAs can occur during any step of the procedure. Multiple modes of injury have been reported in the literature. There are no specific data regarding the most frequent mode of injury. However, many studies have reported unexpected bleeding during removal of bony structures, whether by high-speed drilling, Hajek Sphenoid Punch Forceps, or Kerrison Rongeurs during exposure, with mostly reporting laceration injury, or Type III in our classification.[
Although the number of publication on EEAs to the ventral skull-base lesions has increased significantly, ICA injury associated with it is under-reported or not well reported. Five factors can be identified as reasons for not documenting ICA injuries in the literature; first, the ICA injury can happen without been noticed.[
Chin et al. systematically reviewed ICA injuries during EEA. A total of 38 patients reported no neurological deficits on follow-up. Five patients reported neurological deficits; however, only one patient was found to have persistent neurological deficits on follow-up for the ICA injury. Four patients were pronounced dead intraoperatively due to cardiovascular collapse, and one patient passed away 3 days after the injury.[
Cobb et al. presented a technical case report on ICA injury during an EEA. The patient was diagnosed with skull base osteoblastoma. During the surgery, the cavernous segment of the ICA was injured. Postoperatively, the patient’s neurological status remained unchanged.[
Mortimer et al. reported two cases of ICA injury. The first patient remained well 5 years after the surgery, the second patient reported good recovery and remained well 6 months after the operation.[
Gardner et al., in case series, reported the incidence and outcome of ICA injury during EEA. They encountered seven patients with ICA injury, with an incidence of 0.3%. One patient experienced excessive bleeding intraoperatively from the injured ICA during pituitary surgery. The patient died 36 h postoperatively due to cardiac ischemia.[
Golinelli et al. reported two cases of pseudoaneurysm after ICA laceration during endonasal surgery. The first patient had uneventful outcome postoperatively, and the 10-year follow-up revealed no visual or neurological deficits. The second patient developed postoperative right hemispheric stroke, resulting from a thrombus occluding the ICA.[
After maintaining hemostasis, DSA must be performed immediately to evaluate the nature of the injury.[
Gardner et al. described their institutional algorithm for iatrogenic ICA injury in EES, which was practical and helpful at that time.[
Zhang et al. proposed a modified endovascular treatment protocol that demonstrated that covered stent as the ideal management for ICA injuries. Covered stents have the ability to close the injury site while maintaining the patency of the parent vessel. Moreover, with the introduction of the Wilis stent, which has unique enhanced flexibility,[
Many authors have suggested that stent placement should be attempted in all patients before considering ICA sacrifice. Parent artery occlusion is considered if sufficient collateral arterial supply from the contralateral ICA is confirmed by BTO; however, there is still a 5–10% risk of delayed stroke after BTO, and 4.7% of patients develop a permanent deficit.[
The above review of the literature clearly justifies the need for a classification of the ICA injuries with the objectives of better communication, prevention, management, and advancement of the practice and research in this very important complication of the EEAs.
We faced multiple difficulties in creating this classification, including the underreporting of ICA injuries during EEAs in the literature as well as the limitation of mechanism description, the type of injury and the instrument causing the injury. We believe that this classification system will improve communication in clinical practice and scientific publications and provide a better understanding of the prognosis of these injuries; furthermore, this system should help with the progression from a subjective opinion of surgeons to objective and measurable data that can be documented easily and followed effectively. Despite these limitations, we emphasize the importance of and the need for further anatomical and clinical studies to validate the classification system and modify it accordingly.
CONCLUSION
This is a novel classification system for ICA injuries during extended endonasal endoscopic approaches. This classification system defines the patterns of injuries and the relationship between the injury and the complication’s mortality and functional neurological outcome. Although it is still need to be validated, we strongly believe. It will lead to better recognition of the ICA injuries during EEAs, which will be the first step toward creating protocols for perioperative management of these injuries.
Declaration of patient consent
Institutional Review Board permission obtained for the study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. AlQahtani AA, Castelnuovo P, Nicolai P, Prevedello DM, Locatelli D, Carrau RL. Injury of the internal carotid artery during endoscopic skull base surgery: Prevention and management protocol. Otolaryngol Clin North Am. 2016. 49: 237-52
2. Berker M, Hazer DB, Yü cel T, Gürlek A, Cila A, Aldur M. Complications of endoscopic surgery of the pituitary adenomas: Analysis of 570 patients and review of the literature. Pituitary. 2012. 15: 288-300
3. Biswas D, Daudia A, Jones NS, McConachie NS. Profuse epistaxis following sphenoid surgery: A ruptured carotid artery pseudoaneurysm and its management. J Laryngol Otol. 2009. 123: 692-4
4. Briganti F, Cirillo S, Caranci F, Esposito F, Maiuri F. Development of de novo aneurysms following endovascular procedures. Neuroradiology. 2002. 44: 604-9
5. Cathelinaud O, Bizeau A, Rimbot A, Arteaga C, Verdalle P. Endoscopic endonasal surgery complication: New methods of intracavernous internal carotid artery injury treatment. Rev Laryngol Otol Rhinol (Bord). 2009. 129: 305-8
6. Chin OY, Ghosh R, Fang CH, Baredes S, Liu JK, Eloy JA. Internal carotid artery injury in endoscopic endonasal surgery: A systematic review. Laryngoscope. 2016. 126: 582-90
7. Cobb MP, Nimjee S, Gonzalez LF, Jang DW, Zomorodi A. Direct repair of iatrogenic internal carotid artery injury during endoscopic endonasal approach surgery with temporary endovascular balloon-assisted occlusion: Technical case report. Neurosurgery. 2015. 11: E483-6
8. Del Carmen A, Romero B, Gangadharan JL, Bander ED, Gobin YP, Anand VK. Managing arterial injury in endoscopic skull base surgery: Case series and review of the literature. Oper Neurosurg (Hagerstown). 2017. 13: 138-49
9. Duek I, Sviri G, Amit M, Gil Z. Endoscopic endonasal repair of internal carotid artery injury during endoscopic endonasal surgery. J Neurol Surg Reports. 2017. 78: e125-8
10. Fukushima T, Maroon JC. Repair of carotid artery perforations during transsphenoidal surgery. Surg Neurol. 1998. 50: 174-7
11. Gardner PA, Tormenti MJ, Pant H, Fernandez-Miranda JC, Snyderman CH, Horowitz MB. Carotid Artery injury during endoscopic endonasal skull base surgery. Oper Neurosurg. 2013. 73: 261-70
12. Gardner PA, Tormenti MJ, Pant H, Fernandez-Miranda JC, Snyderman CH, Horowitz MB. Carotid artery injury during endoscopic endonasal skull base surgery: Incidence and outcomes. Neurosurgery. 2013. 73: 261-9
13. Giorgianni A, Pozzi F, Pellegrino C, Padovan S, Karligkiotis A, Castelnuovo P. Emergency placement of a flow diverter stent for an iatrogenic internal carotid artery injury during endoscopic pituitary surgery. World Neurosurg. 2019. 122: 376-9
14. Golinelli G, Toso A, Taranto F, Aluffi P, Pia F. Delayed carotid pseudoaneurysm: A life-threatening complication after endoscopic sinus surgery. J Craniofac Surg. 2012. 23: 1822-4
15. Haralampaki P, Ayyad A, Kockro RA, Perneczky A. Surgical complications after endoscopic transsphenoidal pituitary surgery. J Clin Neurosci. 2009. 16: 786-9
16. Hudgins PA, Browning DG, Gallups J, Gussack GS, Peterman SB, Davis PC. Endoscopic paranasal sinus surgery: Radiographic evaluation of severe complications, in. AJNR American Journal of Neuroradiology. 1992. 13: 1161-7
17. Inamasu J, Guiot BH. Iatrogenic carotid artery injury in neurosurgery. Neurosurg Rev. 2005. 28: 239-47
18. In-Ping Huang Cobb M, Nimjee S, Gonzalez LF, Jang DW, Zomorodi A. Direct repair of iatrogenic internal carotid artery injury during endoscopic endonasal approach surgery with temporary endovascular balloon-assisted occlusion: Technical case report. Clin Neurosurg. 2015. 11: E483-6
19. Isenberg SF, Scott JA. Management of massive hemorrhage during endoscopic sinus surgery. Otolaryngol Head Neck Surg. 1994. 111: 134-6
20. Karadag A, Kinali B, Ugur O, Oran I, Middlebrooks EH, Senoglu M. A case of pseudoaneurysm of the internal carotid artery following endoscopic endonasal pituitary surgery: Endovascular treatment with flow-diverting stent implantation. Acta Medica (Hradec Kralove). 2017. 60: 89-92
21. Karadag A, Kinali B, Ugur O, Oran I, Middlebrooks EH, Senoglu M. A case of pseudoaneurysm of the internal carotid artery following endoscopic endonasal pituitary surgery: Endovascular treatment with flow-diverting stent implantation. Acta Medica (Hradec Kralove). 2017. 60: 89-92
22. Karaman E, Isildak H, Haciyev Y, Kaytaz A, Enver O. Carotid-cavernous fistula after functional endoscopic sinus surgery. J Craniofac Surg. 2009. 20: 556-8
23. Koitschev A, Simon C, Löwenheim H, Naegele T, Ernemann U. Management and outcome after internal carotid artery laceration during surgery of the paranasal sinuses. Acta Otolaryngol. 2006. 126: 730-8
24. Labib MA, Prevedello DM, Carrau R, Kerr EE, Naudy C, Abou Al-Shaar H. A road map to the internal carotid artery in expanded endoscopic endonasal approaches to the ventral cranial base. Neurosurgery. 2014. 10: 448-71
25. Linskey ME, Jungreis CA, Yonas H, Hirsch WL, Sekhar LN, Horton JA. Stroke risk after abrupt internal carotid artery sacrifice: Accuracy of preoperative assessment with balloon test occlusion and stable xenon-enhanced CT. AJNR Am J Neuroradiol. 1994. 15: 829-43
26. Lippert BM, Ringel K, Stoeter P, Hey O, Mann WJ. Stentgraftimplantation for treatment of internal carotid artery injury during endonasal sinus surgery. Am J Rhinol. 2007. 21: 520-4
27. Little AS, Kelly DF, White WL, Gardner PA, Fernandez-Miranda JC, Chicoine MR. Results of a prospective multicenter controlled study comparing surgical outcomes of microscopic versus fully endoscopic transsphenoidal surgery for nonfunctioning pituitary adenomas: The transsphenoidal extent of resection (TRANSSPHER) study. J Neurosurg. 2019. 132: 1-11
28. Lum SG, Gendeh BS, Husain S, Gendeh HS, Ismail MR, Toh CJ. Internal carotid artery injury during endonasal sinus surgery: Our experience and review of the literature. Acta Otorhinolaryngol Ital. 2019. 39: 130-6
29. Mathis JM, Barr JD, Jungreis CA, Yonas H, Sekhar LN, Vincent D. Temporary balloon test occlusion of the internal carotid artery: Experience in 500 cases. AJNR Am J Neuroradiol. 1995. 16: 749-54
30. Mortimer AM, Klimczak K, Nelson RJ, Renowden SA. Endovascular management of cavernous internal carotid artery pseudoaneurysms following transsphenoidal surgery: A report of two cases and review of the literature. Clin Neuroradiol. 2015. 25: 295-300
31. Nariai Y, Kawamura Y, Takigawa T, Hyodo A, Suzuki K. Pipeline embolization for an iatrogenic intracranial internal carotid artery pseudoaneurysm after transsphenoidal pituitary tumor surgery: Case report and review of the literature. Interv Neuroradiol. 2020. 26: 74-822019
32. Nerva JD, Morton RP, Levitt MR, Osbun JW, Ferreira MJ, Ghodke B V. Pipeline embolization device as primary treatment for blister aneurysms and iatrogenic pseudoaneurysms of the internal carotid artery. J Neurointerv Surg. 2015. 7: 210-6
33. Ozgur Z, Celik S, Govsa F, Aktug H, Ozgur T. A study of the course of the internal carotid artery in the parapharyngeal space and its clinical importance. Eur Arch Otorhinolaryngol. 2007. 264: 1483-9
34. Paiva WS, De Andrade AF, Beer-Furlan A, Neville IS, Noleto GS, Bernardo LS. Traumatic carotid-cavernous fistula at the anterior ascending segment of the internal carotid artery in a pediatric patient. Child’s Nerv Syst. 2013. 29: 2287-90
35. Park AH, Stankiewicz JA, Chow J, Azar-Kia B. A protocol for management of a catastrophic complication of functional endoscopic sinus surgery: Internal carotid artery injury. Am J Rhinol. 1998. 12: 153-8
36. Pepper JP, Wadhwa AK, Tsai F, Shibuya T, Wong BJF. Cavernous carotid injury during functional endoscopic sinus surgery: Case presentations and guidelines for optimal management. Am J Rhinol. 2007. 21: 105-9
37. Prevedello DM, Doglietto F, Jane JA, Jagannathan J, Han J, Laws ER. History of endoscopic skull base surgery: Its evolution and current reality. J Neurosurg. 2007. 107: 206-13
38. Rangel-Castilla L, McDougall CG, Spetzler RF, Nakaji P. Urgent cerebral revascularization bypass surgery for iatrogenic skull base internal carotid artery injury. Neurosurgery. 2014. 10: 640-7
39. Reich O, Ringel K, Stoeter P, Maurer J. Verletzung der ACI bei nasennebenhöhlenoperation und management durch endovaskuläre stentapplikation. Laryngorhinootologie. 2009. 88: 322-6
40. Renn WH, Rhoton AL. Microsurgical anatomy of the sellar region. J Neurosurg. 2009. 43: 288-98
41. Shakir HJ, Garson AD, Sorkin GC, Mokin M, Eller JL, Dumont TM. Combined use of covered stent and flow diversion to seal iatrogenic carotid injury with vessel preservation during transsphenoidal endoscopic resection of clival tumor. Surg Neurol Int. 2014. 5: 81
42. Smith TR, Hulou MM, Huang KT, Nery B, de Moura SM, Cote DJ. Complications after transsphenoidal surgery for patients with Cushing’s disease and silent corticotroph adenomas. Neurosurg Focus. 2015. 38: E12
43. Tan HQ, Li MH, Li YD, Fang C, Wang JB, Wang W. Endovascular reconstruction with the willis covered stent for the treatment of large or giant intracranial aneurysms. Cerebrovasc Dis. 2011. 31: 154-62
44. Trivelato FP, Rezende MTS, Ulhôa AC, Giannetti AV. Endovascular treatment of a traumatic carotid artery aneurysm after endoscopic arachnoid cyst fenestration. Child’s Nerv Syst. 2011. 27: 1329-32
45. Valentine R, Wormald PJ. Carotid artery injury after endonasal surgery. Otolaryngol Clin North Am. 2011. 44: 1059-79
46. Weidenbecher M, Huk WJ, Iro H. Internal carotid artery injury during functional endoscopic sinus surgery and its management. Eur Arch Oto-rhino-laryngology. 2005. 262: 640-5
47. Willinsky RA, Taylor SM, TerBrugge K, Farb RI, Tomlinson G, Montanera W. Neurologic complications of cerebral angiography: Prospective analysis of 2,899 procedures and review of the literature. Radiology. 2003. 227: 522-8
48. Zhang HK, Ma N, Sun XC, Wang DH. Endoscopic repair of the injured internal carotid artery utilizing oxidized regenerated cellulose and a free fascia lata graft. J Craniofac Surg. 2016. 27: 1021-4
49. Zhang Y, Tian Z, Li C, Liu J, Zhang Y, Yang X. A modified endovascular treatment protocol for iatrogenic internal carotid artery injuries following endoscopic endonasal surgery. J Neurosurg. 2019. 132: 343-50

