

- Department of Surgery, Section of Neurosurgery, Medical College, Aga Khan University, Karachi, Pakistan
- Department of Surgery, Section of Neurosurgery, Aga Khan University Hospital, Karachi, Pakistan
Correspondence Address:
Imtiaz Hashmi
Department of Surgery, Section of Neurosurgery, Aga Khan University Hospital, Karachi, Pakistan
DOI:10.4103/2152-7806.191083
Copyright: © 2016 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Rai HH, Khan MF, Enam SA, Hashmi I. Co-existing spinal intradural ependymal cyst and sacral Tarlov cyst in adult-onset tethered cord syndrome with syringomyelia: Case report and literature review. Surg Neurol Int 22-Sep-2016;7:
How to cite this URL: Rai HH, Khan MF, Enam SA, Hashmi I. Co-existing spinal intradural ependymal cyst and sacral Tarlov cyst in adult-onset tethered cord syndrome with syringomyelia: Case report and literature review. Surg Neurol Int 22-Sep-2016;7:. Available from: http://surgicalneurologyint.com/surgicalint_articles/co%e2%80%91existing-spinal-intradural-ependymal-cyst-sacral-tarlov-cyst-adult%e2%80%91onset-tethered-cord-syndrome-syringomyelia-case-report-literature-review/
Abstract
Background:Synchronous spinal intradural ependymal cysts and sacral Tarlov cysts in adult onset tethered cord syndrome are extremely rare.
Case Description:A 23-year-old male presented with back pain radiating into both lower extremities, accompanied by acute onset of gait difficulty and sphincter dysfunction. Magnetic resonance imaging identified a low lying conus medullaris, syringomyelia with septations extending from T12 to S1, a tethered cord, and a thickened filum terminale with a sacral Tarlov cyst. The patient underwent a L3-4 laminectomy for decompression of syringomyelia and excision/biopsy of a space occupying lesion along with S1-2 laminectomy for cord untethering and Tarlov cyst fenestration. Postoperative histopathology confirmed that the lesion was an ependymal cyst. Clinically, patient showed marked improvement in the neurological status.
Conclusion:Simultaneous decompressive laminectomy of L3-4 and S1-2 effectively decompressed the syringomyelia while allowing for excision/biopsy of a space occupying lesion at the former and untethering and Tarlov cyst fenestration at the latter levels.
Keywords: Adult tethered cord syndrome, ependymal cyst, Tarlov cyst
INTRODUCTION
Tethered cord syndrome (TCS), a form of spinal dysraphism, is defined by a low lying conus medullaris that is tethered by a thickened filum terminale. Because acute symptomatic presentation in adults with TCS is rare, TCS diagnosis is often substantially delayed.
Ependymal cysts, rare benign neuroepithelial congenital lesions that are typically located in the paraventricular white matter (frontal/parietal lobes), are only rarely encountered in the spine. Gross total resection (GTR) may only be possible in 28% of the patients with intramedullary ependymal cysts, and may even be difficult to those located elsewhere.[
Tarlov perineural cysts comprise collections of cerebrospinal fluid (CSF) located between the endoneurium and perineurium of the nerve root sheath near the dorsal root ganglion. Although Tarlov cysts are incidental findings in 4.6–9% of magnetic resonance imaging (MRI) scans, 1% of sacral lesions become symptomatic due to local compression, causing local pain, radiculopathy, and incontinence.[
Here, we present a 23-year-old patient with a thoracolumbar intradural ependymal cyst and sacral Tarlov cyst with adult TCS/syringomyelia, which was treated successfully with microsurgical decompression (e.g. laminectomy L3-4 and S1-2) and shunting.
CASE REPORT
Case presentation, examination, and investigation
A 23-year-old male presented with 2–4 weeks of worsening left greater than right-sided lower back pain, radiating bilaterally into both lower extremities, accompanied by 4 days of urinary overflow incontinence. On neurological examination, the patient exhibited decreased distal strength in both lower extremities (grade 3/5 dorsiflexion, grade 2/5 planterflexion, grade 1/5 inversion and eversion), with decreased sensation in the L5 and S1 distribution and absent Achilles response. A full spine MRI revealed mixed signal abnormalities in the thoracolumbosacral spinal canal representing a T12-S1 syrinx with septations, a tethered cord, and thickened filum terminale [
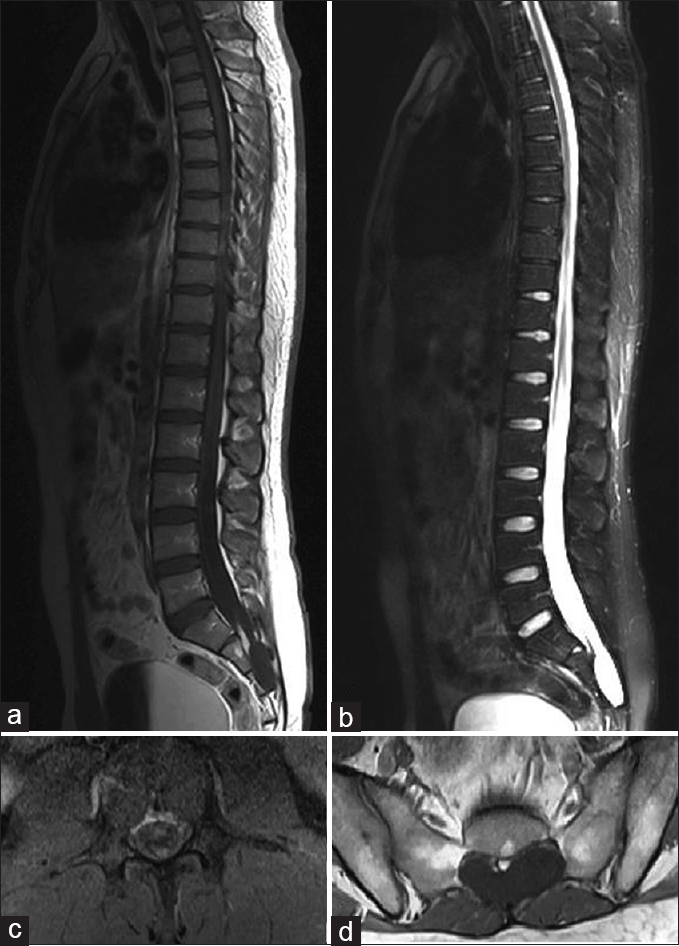
Figure 1
Preoperative (a) T1 and (b) T2-weighted sagittal magnetic resonance imaging (MRI) showing mixed signal abnormalities representing syringomyelia with septations extending from T12 to S1 levels, alongside cord tethering and thickening of the filum terminale at the S2 level. Another signal abnormality seen at S2-3 level causing scalloping of the vertebral bodies – isointense on T1 (a) and hyperintense on T2 (b), representing a Tarlov cyst. T1-weighted axial cuts at the L3-4 level (c) highlighting contrast enhancement of a solid component with gadolinium and enlargement of the spinal canal at the S2 level by the Tarlov cyst (d)
Surgery
During surgery, a L3-4 laminectomy revealed thinned-out dura, and a midline myelotomy decompressed the syringomyelia and revealed a gliotic encysted space occupying lesion that was biopsied [
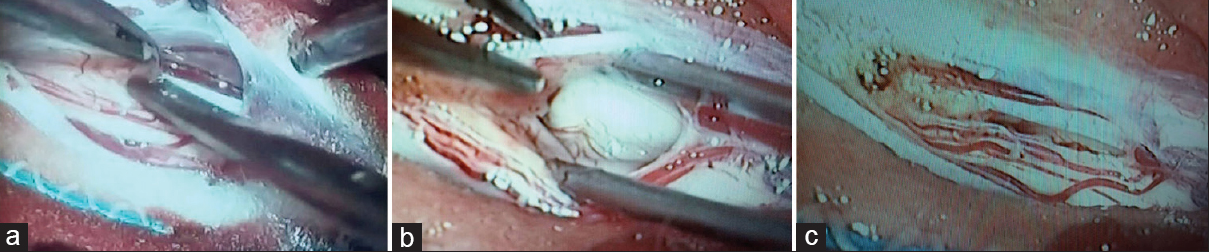

Figure 3
(a) Represents the thickened filum terminale observed after S1-2 laminectomy, which was divided to untether the cord. (b) The picture shows the relation of the Tarlov cyst with the durotomy (proximal) done for un-tethering. (c) Represents the fenestration of the Tarlov cyst with evacuation of fluid and partial removal of the cyst wall
Neurological examination postoperatively
By the 3rd postoperative day, the patient's distal strength improved to the 4−/5 level on the left side and 4+/5 level on the right side; pain was relieved and sphincter control improved. Two weeks later, the patient was ambulated with minimal support, and sphincter function and his neurological exam normalized.
Histopathology
Pathologically, the gliotic space occupying lesion at the L3-4 level was an ependymal cyst. It was lined by cuboidal cells with rounded uniform nuclei, inconspicuous nucleoli, and eosinophilic cytoplasm. Glial tissue was identified just underneath these cells and immunohistochemical stain was positive for S-100 protein and glial fibrillary acidic protein (GFAP), however, it was negative for cytokeratin AE1/AE3 and epithelial membrane antigen.
DISCUSSION
Diagnosis and treatment of tethered cord syndrome
In the absence of any history of spinal dysraphism, adults presenting with TCS are rare. MRI demonstrates a thickened, posteriorly displaced filum terminale (>2 mm), often with a low lying conus usually below the L2 vertebral body.[
Diagnosis and treatment of ependymal cysts
Ependymal cysts and particularly intramedullary spinal cysts are rarely encountered in the adult spine. As in the case presented here, patients may present with pain, motor, sensory, and sphincter dysfunction.[
Tarlov cyst management
The optimal management of symptomatic Tarlov cysts is controversial. Surgical options include lumbar CSF drainage, lumbar peritoneal shunt, cyst subarachnoid shunt, CT-guided percutaneous aspiration of the cyst, with or without infusion of fibrin glue, laminectomy for decompression of cyst, partial cyst removal with neck ligation or wall imbrication, and microsurgical fenestration of cyst to the thecal sac. Varying rates of symptom resolution, cyst recurrence, and postoperative complications have been reported.[
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Acosta FL, Quinones-Hinojosa A, Schmidt MH, Weinstein PR. Diagnosis and management of sacral Tarlov cysts. Case report and review of the literature. Neurosurg Focus. 2003. 15: E15-
2. Lee GY, Paradiso G, Tator CH, Gentili F, Massicotte EM, Fehlings MG. Surgical management of tethered cord syndrome in adults: Indications, techniques, and long-term outcomes in 60 patients. J Neurosurg Spine. 2006. 4: 123-31
3. Park CH, Hyun SJ, Kim KJ, Kim HJ. Spinal intramedullary ependymal cysts: A case report and review of the literature. J Korean Neurosurg Soc. 2012. 52: 67-70
4. Paulsen RD, Call GA, Murtagh FR. Prevalence and percutaneous drainage of cysts of the sacral nerve root sheath (Tarlov cysts). AJNR Am J Neuroradiol. 1994. 15: 293-7
5. Raghavan N, Barkovich AJ, Edwards M, Norman D. MR imaging in the tethered spinal cord syndrome. AJR American journal of roentgenology. 1989. 152: 843-52
6. Saito K, Morita A, Shibahara J, Kirino T. Spinal intramedullary ependymal cyst: A case report and review of the literature. Acta Neurochir. 2005. 147: 443-6

