

- Department of Neurosurgery, University of Louisville, 220 Abraham Flexner Way, Suite 1500, Louisville, Kentucky, United States.
DOI:10.25259/SNI_15_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Zaid Aljuboori, William Burke, Kimberly Meyer, Brian Williams. Cost analysis of cordotomy and intrathecal pain pump placement for refractory cancer pain. 18-Apr-2020;11:72
How to cite this URL: Zaid Aljuboori, William Burke, Kimberly Meyer, Brian Williams. Cost analysis of cordotomy and intrathecal pain pump placement for refractory cancer pain. 18-Apr-2020;11:72. Available from: https://surgicalneurologyint.com/surgicalint-articles/9965/
Date of Submission
13-Jan-2020
Date of Acceptance
24-Mar-2020
Date of Web Publication
18-Apr-2020
Abstract
Background: Cancer pain can be debilitating and 10–20% of patients will have refractory pain despite optimal medical management. Here, we present a cost comparison of treating terminal cancer patients with intravenous (IV) narcotics, anterolateral cordotomy, or intrathecal pain pump (ITPP) placement.
Case Description: We evaluated and treated 2 patients with metastatic breast cancer and expected survivals of
Conclusion: The treatment of refractory pain in cancer patients is challenging. It requires invasive procedures such as cordotomy or ITPP. Although procedures may yield comparable pain control, there was a significant cost savings for cordotomy versus ITPP ($57,043 saved).
Keywords: Cancer, Cost, Neuroablation, Neuromodulation, Opioids, Pain
INTRODUCTION
Cancer-related pain represents a challenge to manage medically, and most patients will require higher and higher doses of opioid analgesics due to receptor downregulation, which puts them at risk of opioid addiction and death.[
CASE DESCRIPTION
Case 1
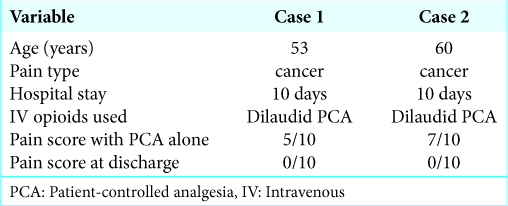
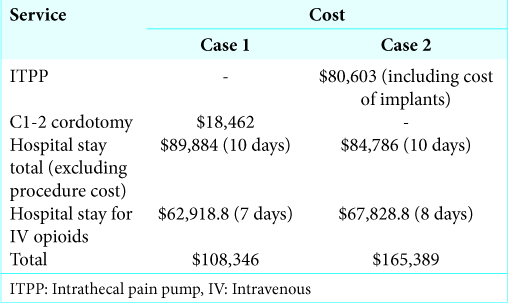
A 53-year-old female with metastatic breast cancer presented with severe pain involving the right chest wall; her n expected survival was <1 year. She had failed oral narcotics and was admitted for 7 days of Dilaudid patient-controlled analgesia (PCA); nevertheless, this left her with a 5/10 residual pain score. She, therefore, underwent a left-sided C1-2 cordotomy which resulted in immediate pain relief. The PCA was weaned over 2 days and she was discharged home in stable condition. The total cost of her care was $108,346; $18,462 for the cordotomy, $89,884 for the hospital stay [
Case 2
A 60-year-old female with metastatic breast cancer and an expected survival of <1 year presented with severe cancer- related pain involving the left knee cap. She failed oral narcotics and local nerve blocks. She was admitted for Dilaudid PCA, but her residual pain was 7/10 on the VAS, so she underwent ITPP placement. Immediately postoperatively she experienced partial pain relief and the PCA was weaned over 7 days (e.g., to titrate the intrathecal opioids), at which point she was discharged home. The total cost of her care totaled $165,389; $80,603 for the ITPP placement procedure (including the implants) and $84,786 for the hospital stay [
DISCUSSION
In 1986, the World Health Organization stated the following “to provide relief from pain to the patient’s satisfaction, so that [they] may function effectively and eventually die free from pain” in regard to cancer-related pain.[
Cost summary
In a cancer patient with expected survivals of <1 year, cordotomy saved about $57,053 in total cost versus ITPP. Therefore, for patients with estimated survivals of under 1 year, cordotomy was the most cost-effective versus ITPP in which is a better option in cancer patients with survival estimated at >1 year.
CONCLUSION
There is an obvious need for cost effective and adequate treatment for cancer-related pain. This study documented the lesser costs but comparable efficacy of utilizing cordotomy to treat patients with estimated survivals of <1 year versus the recommendation to consider ITPP for those with >1 year to live.
Declaration of patient consent
Patient’s consent not required as patient’s identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Brogan SE, Winter NB, Abiodun A, Safarpour R. A cost utilization analysis of intrathecal therapy for refractory cancer pain: Identifying factors associated with cost benefit. Pain Med. 2013. 14: 478-86
2. Burchiel KJ, Raslan AM. Contemporary concepts of pain surgery. J Neurosurg. 2019. 130: 1039-49
3. Collins KL, Patil PG. Flat-panel fluoroscopy O-arm-guided percutaneous radiofrequency cordotomy: A new technique for the treatment of unilateral cancer pain. Neurosurgery. 2013. 72: 27-34
4. de Courcy JG. Interventional techniques for cancer pain management. Clin Oncol (R Coll Radiol). 2011. 23: 407-17
5. Grossman SA, Staats PS. Current management of pain in patients with cancer. Oncology (Williston Park). 1994. 8: 93-107
6. Meyer R, Patel AM, Rattana SK, Quock TP, Mody SH. Prescription opioid abuse: A literature review of the clinical and economic burden in the United States. Popul Health Manag. 2014. 17: 372-87
7. Viswanathan A, Vedantam A, Hess KR, Ochoa J, Dougherty PM, Reddy AS. Minimally invasive cordotomy for refractory cancer pain: A randomized controlled trial. Oncologist. 2019. 24: e590-e6

