

- Neurosurgery Department, Unidade Local de Saúde de São João (ULS São João), Oporto, Portugal
- Faculty of Medicine, Oporto University, Oporto, Portugal
- RISE-Health, Portugal
Correspondence Address:
João Meira Gonçalves, Department of Neurosurgery, Unidade Local de Saúde de São João (ULS São João), Porto, Portugal.
DOI:10.25259/SNI_391_2024
Copyright: © 2024 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: João Meira Gonçalves1,2, António Vilarinho1,2,3, Vasco Carvalho1,2, Patrícia Polónia1,2, Pedro Alberto Silva1,2,3. Delayed cyst formation after radiosurgery for arteriovenous malformation: A case report and critical review. 11-Oct-2024;15:371
How to cite this URL: João Meira Gonçalves1,2, António Vilarinho1,2,3, Vasco Carvalho1,2, Patrícia Polónia1,2, Pedro Alberto Silva1,2,3. Delayed cyst formation after radiosurgery for arteriovenous malformation: A case report and critical review. 11-Oct-2024;15:371. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=13144
Date of Submission
21-May-2024
Date of Acceptance
10-Sep-2024
Date of Web Publication
11-Oct-2024
Abstract
Background: Stereotactic radiosurgery (SRS) is a validated treatment option for cerebral arteriovenous malformations (AVMs), even if a greater knowledge of its potential delayed complications is still being acquired.
Case Description: A 49-year-old man suffered multiple episodes of cerebral hemorrhage in an approximate 10-year follow-up interval in the context of a left central core AVM with deep venous drainage into the internal cerebral veins (Spetzler Martin Grade 4) despite being treated with gamma knife radiosurgery at two separate timepoints, and with an almost complete obliteration confirmed. Approximately 10 years after the first radiosurgery treatment, he developed severe motor aphasia, Grade 3 right hemiparesis, progressive confusion, and memory deficits. Cerebral imaging revealed cystic degeneration in the AVM’s periphery. Cyst fenestration and cystoperitoneal shunt were attempted. The treatments were temporarily effective, but a progressive cyst enlargement recurred with clinical deterioration. The patient was therefore proposed for surgical mass and cyst excision through an interhemispheric transcallosal approach. The postoperative magnetic resonance imaging showed complete removal of the lesion, and an uneventful post-operative course ensued. At the 6-month follow-up, our patient experienced a noticeable improvement in his speech, power, dexterity and was able to walk autonomously.
Conclusion: Cystic degeneration of AVMs is a possible long-term complication after SRS. Long-term follow-up and data on such patients remain crucial, even with evidence of complete nidal obliteration.
Keywords: Arteriovenous malformation (AVM), Chronic encapsulated expanding hematomas (CEEH), Delayed Cyst (DC), Radiosurgery (RS)
INTRODUCTION
Stereotactic radiosurgery (SRS) has become a commonly used and recognized treatment modality for cerebral arteriovenous malformation (AVM). As an increasing number of patients with AVMs undergo the procedure,[
Cyst formation after SRS is a rare entity, and the time progression of cyst enlargement is characteristically longer than that of more normally witnessed adverse events after SRS.[
The majority of radiation-induced complications will manifest symptoms or signs within 3 years of SRS. Radiation-induced complications presenting beyond 3 years are less well comprehended.[
We present a case of delayed cystic formation with an unusually prolonged latency period of 10 years after the first exposure to SRS. We also discuss the possible etiology of the cystic lesion as well as the relevance of long-term follow-up using magnetic resonance imaging (MRI) for these patients, even when complete nidus obliteration is achieved.
CASE REPORT
A 49-year-old male began experiencing an intense headache in 2009. The neurologic examination was unremarkable, but magnetic resonance (MR) and MR angiography imaging revealed a left-sided basal ganglia/thalamic AVM without evidence of previous hemorrhage associated. Angiography confirmed it was supplied mainly by perforating branches arising from the left proximal anterior, middle, and posterior cerebral arteries. The venous drainage was through an internal cerebral vein (varicose dilation). The nidal dimensions were 2.2 × 1.0 × 3.0 cm (Spetzler–Martin grade IV), it was compact, and no intranidal aneurysms were found. Still, during the workup, the patient suffered an event of severe headaches and transient loss of consciousness. The urgent scan revealed a subarachnoid hemorrhage and minimal intraventricular bleeding. He was discharged a week later without new neurological findings.
After a multidisciplinary debate, radiosurgery was favored as a treatment modality (given the specific anatomical location and neurological status). High-resolution axial plane imaging was performed to facilitate dose planning. The SRS dose margin covered the entire AVM nidus volume, with a prescribed dosage of 22 Gray delivered in a single treatment fraction.
During follow-up, as the patient’s headache significantly improved, there was evidence of repeated minor lesional hemorrhages that were managed conservatively, given their reduced volume and given the fact that there was no significant worsening of the neurological condition [

In 2016, a new digital subtraction angiography (DSA) showed preservation of some of the previously identified feeders and a new dilation of the left Trollard, fronto-orbital, and middle cerebral veins suggesting a pattern of redesigned venous drainage for the AVM [

Figure 2:
Digital subtraction angiography (DSA) images: Selective left vertebral artery catheterization (left side: Lateral view) + (right side: Anterior-posterior view) - Posttreatment DSA picture reveals an arteriovenous malformation that is supplied by the left posterior cerebral artery, namely the posteromedial choroidal artery. Venous drainage was via the left internal cerebral vein (varicose vein).
Taking into consideration the previous failure of radiosurgery on this still active AVM, its remoteness in time, and also both the neurological preservation and lack of a safe alternative, the patient was accepted for a second Gamma Knife treatment. The prescribed radiation dose was reduced in an attempt to minimize the chance of radiation-related complications.
One year after the second GKR, the patient experienced a recurrence of headaches. MRI displayed a novel cystic mass lesion with signs of perilesional hemorrhage congruent with the area of previous AVM [

A repeated DSA demonstrated complete occlusion of the AVM with no remaining arteriovenous shunt or nidus. Minimal angioid tissue was visible but definitely no evidence of early venous drainage could be observed as the patient reported significant improvement in headaches.
Eight months later, he developed right hemiparesis (grade 4/5), motor aphasia, and an inability to walk autonomously. He was admitted to the neurosurgery ward, where an MRI [
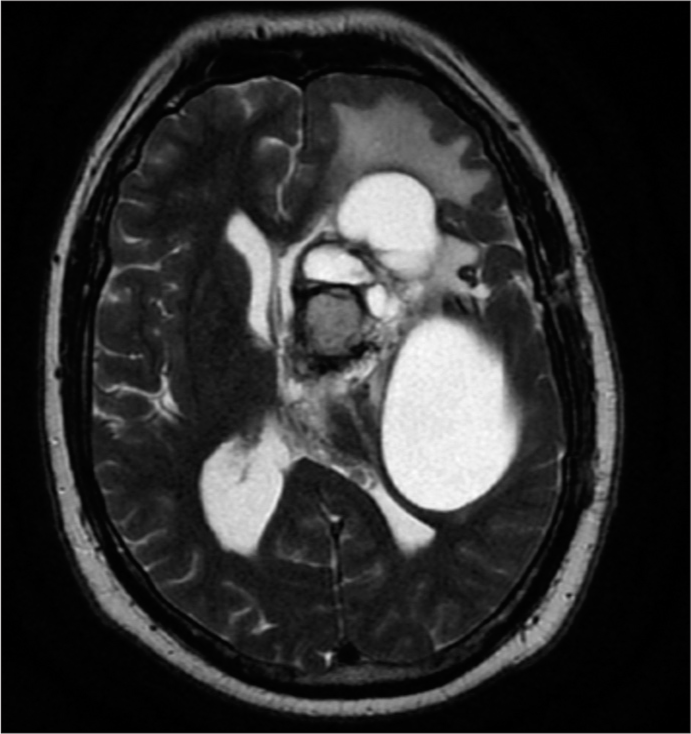
He underwent surgical fenestration of the larger (posterior) cyst and displayed immediate neurological improvement. A post-operative computed tomography brain scan demonstrated a successful collapse of the temporal cyst while the two anterior ones persisted. Unfortunately, 3 months later, both the complaints and the cyst recurred, and a cystoperitoneal shunt was proposed. After this procedure, the patient experienced only a slight improvement in his expressive aphasia and motor function. He was discharged on postoperative day 14 for early outpatient rehabilitation.
One year after that second surgery, in 2021, he again manifested progressive neurological deterioration. The patient and his family members noted that he was more forgetful about recent events, and he was having difficulty walking suffering multiple falls. He had severe impairment of his functionality with right hemiparesis and disorientation.
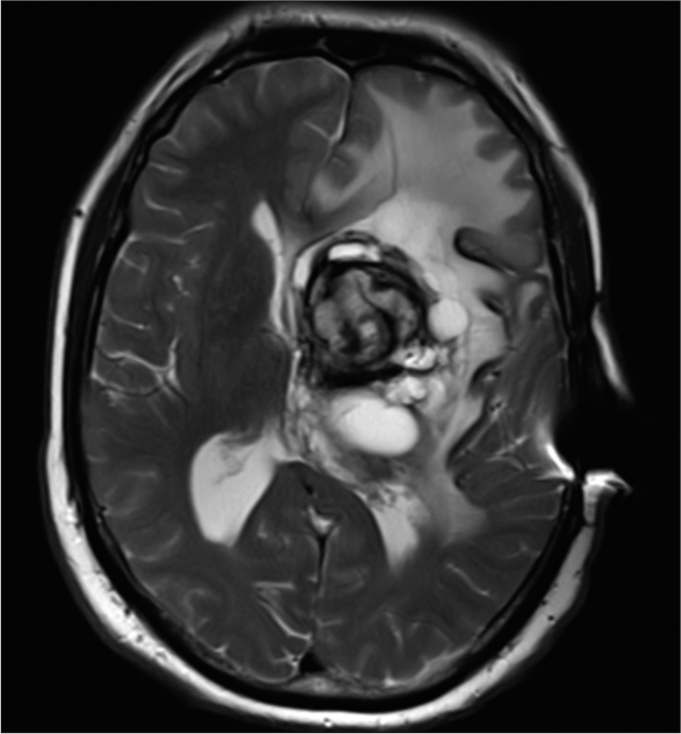
There was severe worsening of his speech, and MRI showed lesion progression with intralesional hemorrhage and an increased mass effect [
An interhemispheric transcallosal approach was performed, and total gross excision of the lesion was accomplished. The mass was very organized and solid, while residual tortuous feeders were identified in its periphery. A histopathological examination revealed the presence of gliosis and blood vessels with hyalinized walls with no evidence of necrosis or malignancy. There were signs of both recent and remote bleeding.
A complete resection of the cyst was confirmed on postoperative MRI [
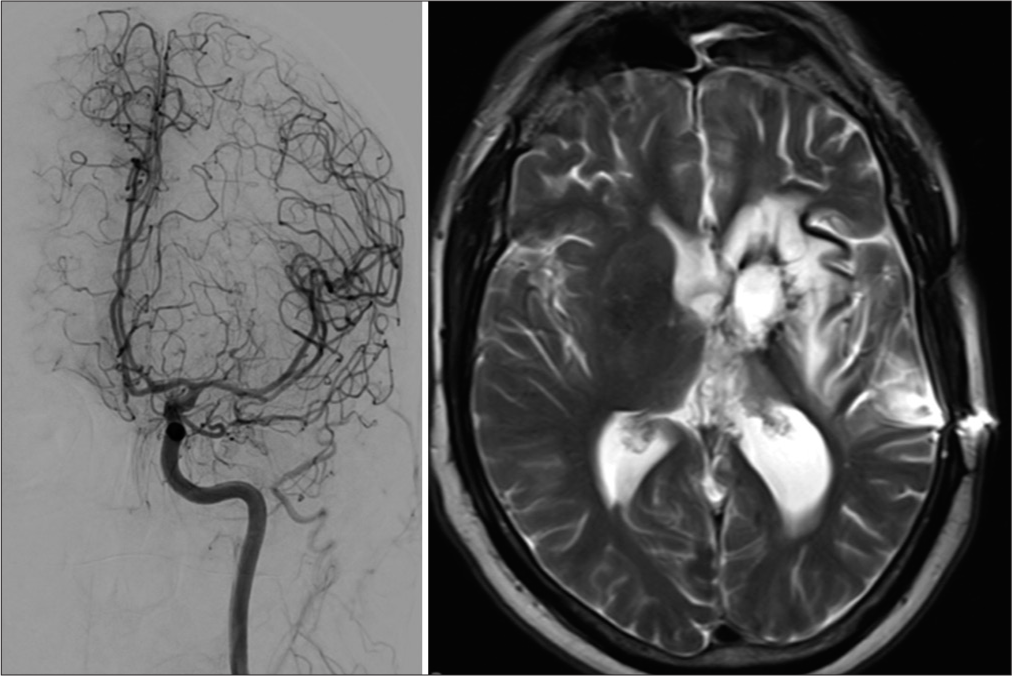
Figure 6:
Left digital subtraction angiography image (left internal carotid artery catheterization) – Complete obliteration of the arteriovenous malformation with minimal angioid tissue without early venous drainage. Right - T2-weighted axial image: No obvious mass component at the site of surgery due to residual or recurrence of the known cysts.
Our patient experienced improvement in his speech, power, and dexterity and was able to walk autonomously. He had mild right hemiparesis (Grade 4) with reduced dexterity and was able to walk with an assistive device, such as a cane. Finally, there was mild expressive aphasia.
DISCUSSION
In the management of cerebral AVMs, several treatment modalities have been implemented, each with its inherent advantages and restraints.
When indicated, SRS has been established as a generally secure and effective treatment technique for cerebral AVMs.[
We present here an unusual type of lesion that progressed at the site of a completely obliterated AVM following SRS. This cystic/hemorrhagic degeneration had a gradual clinical onset through self-perpetuating minor hemorrhages. In this particular case, the possibility cannot be excluded that unceasing minor bleeding from the residuary nidus resulted in the hematoma’s progressive enlargement and may have contributed to new cysts formation. This evokes two potentially inextricable entities described in the literature - chronic encapsulated expanding hematomas (CEEH) and delayed cyst formation.
Delayed cyst formation and/or CEEH have episodically been described following SRS-induced AVM obliteration, though uncommonly.[
There are several reports of cysts adjacent to the hematoma, which has been portrayed in 1–3% after SRS for AVM.[
Several hypotheses for the pathogenesis of these lesions have been suggested. Some chronic encapsulated intracerebral hematomas without a clear source of bleeding were related to vascular malformations that were damaged or clotted during bleeding episodes. Abou-Al-Shaar et al. highlighted that occult “self-destroying” AVM was responsible for the first hemorrhage.[
On the other hand, for cyst formation, blood vessels exposed to a high dosage of radiation may acquire increased permeability, consequently allowing fluid to be liberated from the vasculature into the parenchyma. This can be the source of the accumulation of an exudative fluid and subsequent cyst development.[
This case hints that rebleeding during the latency interval between SRS and DSA cure could occur differently from the original bleedings.
Some factors may lead to the development of these lesions, such as incomplete obliteration of an AVM nidus, SRS maximum dose, higher AVM size, and lobar nidus location.[
Patients with incidentally discovered cysts can be followed initially with surveillance imaging. There is no agreement concerning the optimal timing or even frequency for the follow-up. However, those who develop subacute or late radiation effects should undergo follow-up imaging more regularly.[
Various therapeutic alternatives may be used for cyst management. An Ommaya reservoir can offer instant symptomatic relief, and recurrent aspirations can be used to control cyst development. Cystoperitoneal shunting can be a good option for cysts with simple anatomy or patients with various comorbidities.[
In line with what is described in the literature and within our case, we think that excision or removal of the lesion can ultimately be more definitive than repeated drainages. Surgical excision, while more aggressive, may offer the prospect of cure and, when feasible, should be offered, particularly if the lesion is enhanced on imaging, accompanied by repetitive hemorrhages and patients with cysts that persistently fill despite other treatments.[
The management of deep-seated lesions such as the one presented still poses a challenge to neurosurgeons. Our choice of approach, for instance, presents inherent risks for cerebrospinal fluid diversion, transient hemiparesis, infection, post-operative seizures, and memory disturbance.[
CONCLUSION
Following SRS for AVM, the development of delayed complications is possible, and a chronic encapsulated hematoma may be responsible for a new onset of focal neurological syndromes. Given CEEH’s and delayed cyst latency to presentation, long-term imaging follow-up of AVM patients who undergo SRS is recommended, particularly in deep and/or larger AVMs. Clinicians in this field may benefit from being aware of this clinical behavior and radiological findings of this rather rare disorder.
The ideal management for symptomatic lesions is still to be defined. Shunting the cyst may remain an option but sometimes can work only as a short-term measure, and surgical excision may be the best treatment.
Author’s contributions
JMG wrote the manuscript and reviewed the literature, VC reviewed the literature, AV revised the manuscript and performed the surgeries, PP, AV, and PAS revised the manuscript.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Abou-Al-Shaar H, Faramand A, Zhang X, Mallela AN, Branstetter BF, Wiley CA. Chronic encapsulated expanding hematomas after stereotactic radiosurgery for intracranial arteriovenous malformations. J Neurosurg. 2021. 136: 492-502
2. Al Hinai Q, Tampieri D, Souhami L, Sadikot A, Sinclair D, Leblanc R. Cyst formation following radiosurgery for AVMs: Report of 3 cases. Can J Neurol Sci. 2011. 38: 734-40
3. Aryan HE, Ozgur BM, Jandial R, Levy ML. Complications of interhemispheric transcallosal approach in children: Review of 15 years experience. Clin Neurol Neurosurg. 2006. 108: 790-3
4. Byun J, Kwon DH, Lee DH, Park W, Park JC, Ahn JS. Radiosurgery for cerebral arteriovenous malformation (AVM): Current treatment strategy and radiosurgical technique for large cerebral AVM. J Korean Neurosurg Soc. 2020. 63: 415-26
5. Choi MS, Joo M, Choi CY. Chronic encapsulated expanding hematoma after stereotactic radiosurgery of cerebral arteriovenous malformation. J Cerebrovasc Endovasc Neurosurg. 2019. 21: 152-7
6. Kahrom A, Grimley R, Jeffree RL. A case of delayed cyst formation post brain AVM stereotactic radiosurgery for arteriovenous malformation: Case report. J Clin Neurosci. 2021. 87: 17-9
7. Kano H, Kondziolka D, Flickinger JC, Yang HC, Flannery TJ, Awan NR. Stereotactic radiosurgery for arteriovenous malformations, Part 3: Outcome predictors and risks after repeat radiosurgery. J Neurosurg. 2012. 116: 21-32
8. Kurita H, Sasaki T, Kawamoto S, Taniguchi M, Kitanaka C, Nakaguchi H. Chronic encapsulated expanding hematoma in association with gamma knife stereotactic radiosurgery for a cerebral arteriovenous malformation. Case report. J Neurosurg. 1996. 84: 874-8
9. Pollock BE, Link MJ, Stafford SL, Parney IF, Garces YI, Foote RL. The risk of radiation-induced tumors or malignant transformation after single-fraction intracranial radiosurgery: Results based on a 25-year experience. Int J Radiat Oncol Biol Phys. 2017. 97: 919-23
10. Pomeraniec IJ, Ding D, Starke RM, Liu KC, Mrachek EK, Lopes MB. Delayed cyst formation after stereotactic radiosurgery for brain arteriovenous malformations. J Neurosurg. 2018. 129: 937-46
11. Stapf C, Mast H, Sciacca RR, Choi JH, Khaw AV, Connolly ES. Predictors of hemorrhage in patients with untreated brain arteriovenous malformation. Neurology. 2006. 66: 1350-5
12. Wolak ML, Murphy EC, Powell SZ. Tumefactive cyst with a vascular blush as a late complication after combined embolization and stereotactic radiosurgery treatments for a cerebral arteriovenous malformation. Acta Neurochir. 2007. 149: 705-12

