

- Department of Neurosurgery, Aga Khan University, Karachi, Pakistan,
- Medical College, University of Western Australia, Crawley, Perth, Australia.
Correspondence Address:
Ehsan Bari, Department of Neurosurgery, Aga Khan University, Karachi, Pakistan.
DOI:10.25259/SNI_793_2022
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Quratulain Tariq1, Mishaal Ather1, Ahmer Nasir Baig1, Amman Bari2, Ehsan Bari1. Developmental delay in a patient with single cerebral varix. 02-Dec-2022;13:559
How to cite this URL: Quratulain Tariq1, Mishaal Ather1, Ahmer Nasir Baig1, Amman Bari2, Ehsan Bari1. Developmental delay in a patient with single cerebral varix. 02-Dec-2022;13:559. Available from: https://surgicalneurologyint.com/surgicalint-articles/12041/
Date of Submission
29-Aug-2022
Date of Acceptance
11-Nov-2022
Date of Web Publication
02-Dec-2022
Abstract
Background: Cerebral varices are intracranial venous anomalies that are characterized as thin-walled vessels, with a single layer of endothelium lining it and a thin lamina or fibrous connective tissue surrounding it. These varices are usually associated with vascular abnormalities such as arteriovenous malformations or developmental venous anomalies, but may rarely be found as isolated lesions as well. Diagnosis of these isolated lesions on imaging is a challenge, because it is a rare entity and can mimic a space occupying lesion in the brain. The patients with isolated cerebral varix can present with neurological symptoms; however, majority are asymptomatic with the diagnosis made incidentally.
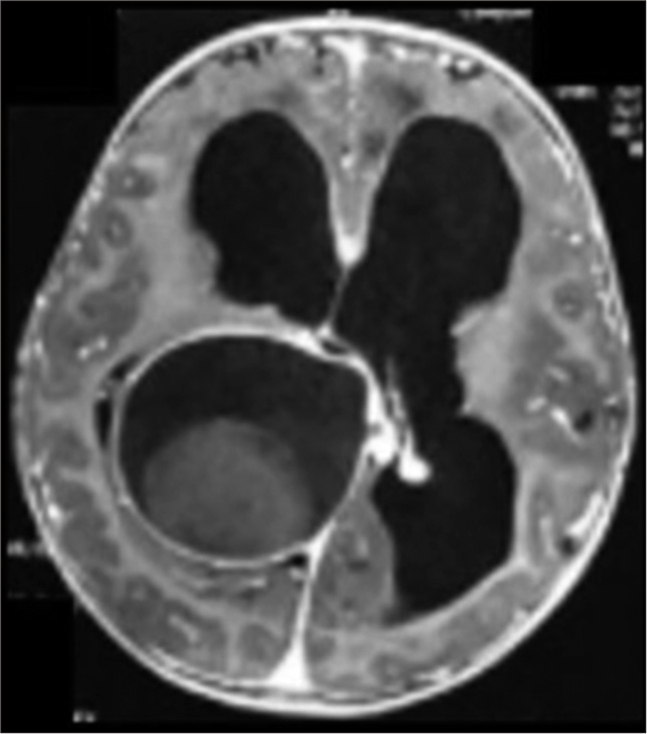
Case Description: The aim of this study is to report a case of a 21-month-old boy who was diagnosed with an isolated cerebral varix and had presented with delayed milestones in addition to seizures. His MRI scans showed a solid-cum-cystic lesion with contrast enhancing walls that was excised through craniotomy. Postoperatively, he regained his milestones.
Conclusion: The patients with isolated cerebral varix can present with neurological symptoms; however, majority are asymptomatic with the diagnosis made incidentally. These patients have a low risk of bleeding and are treated conservatively, with surgical intervention indicated only in symptomatic patients.
Keywords: AV malformations, Cerebral varix, Delayed milestones, Developmental venous anomalies
INTRODUCTION
Cerebral varices are intracranial venous anomalies that are histologically characterized as thin-walled vessels, with a single layer of endothelium lining it and a thin lamina or fibrous connective tissue surrounding it.[
CASE REPORT
A 21-month-old baby boy presented with delayed milestones for 2 months, fever and left-sided seizures with mild hemiparesis for 8 months. The patient underwent an MRI scan that demonstrated a solid cum cystic lesion with only contrast enhancing cyst wall [

The patient underwent right frontal extraventricular drain placement and excision of the right parietal space occupying lesion. The intraoperative findings were large and well-encapsulated lesion in the right parietotemporal region which was adherent tentorium cerebelli and medially to midbrain [

A large abnormal thrombosed cortical vein was ending into the cystic part of the lesion, with the lumen filled with a clot [

Postoperatively, the patient did well and discharged on 4th postoperative day. After surgery, he started to regain his milestones, and on 2 years follow-up, he can walk with little assistance and can communicate well with his family. Repeat CT scan [

DISCUSSION
Cerebral varices are vascular anomalies that can originate from arteriovenous malformations or DVAs. It has been postulated that the difference in the intravascular pressures in arteriovenous shunts leads to changes in vessel walls with time resulting in subsequent formation of varices, whereas the congenital abnormality in cases of DVAs predisposes the formation of varices. It may also present as isolated cerebral varices, the first of which was reported in 1887 by Pfennenstiel.[
Multiple cases have thereafter been reported, with patients noted to have neurological symptoms or associated anomalies and patients who are asymptomatic and have been diagnosed incidentally. Other studies have shown the varices to be associated with sinus and venous anomalies and neurocutaneous abnormalities. However, most of these patients were managed conservatively with no neurological consequences.[
The initial diagnosis of cerebral varix is a challenge, particularly in patients with isolated cerebral varix, since it can be easily misdiagnosed as an intracranial tumor.[
In this case study, the MRI scan showed a lesion with peripheral enhancing wall. In lieu of the patients presenting symptoms, the patient was planned for surgery with the impression of a space-occupying lesion. On intraoperative observation, however, the space occupying lesion was found to be a cystic dilation of a vein, which was subsequently confirmed on the tissue biopsy.
Even though, the preoperative imaging was misleading, this patient was a candidate for surgery regardless due to his clinical symptoms as suggested by previous studies.[
CONCLUSION
Cerebral varices have a variable clinical course and are subject to misdiagnosis resulting in unnecessary surgical interventions. Diagnosis of cerebral varices is difficult due to similar characteristics as that of a tumor on imaging. MRI scans and CT scans are the first modalities for diagnosis, but imaging with MR and CT angiography can confirm diagnosis and help guide the further course of treatment.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Dietrich U, Forsting M. Isolated venous aneurysm (cerebral varicose vein)--a rare differential diagnosis. Rofo. 1998. 169: 441-3
2. Gomez DF, Mejia JA, Murcia DJ, Useche N. Isolated giant cerebral varix-a diagnostic and therapeutic challenge: A case report. Surg Neurol Int. 2016. 7: S156-9
3. Hoell T, Hohaus C, Beier A, Holzhausen HJ, Meisel HJ. Cortical venous aneurysm isolated cerebral varix. Interv Neuroradiol. 2004. 10: 161-5
4. Kazumata K, Fujimoto S, Idosaka H, Kuroda S, Nunomura M, Houkin K. Multiple varices in the unilateral cerebral venous system. AJNR Am J Neuroradiol. 1999. 20: 1243-4
5. Kim HS, Park SC, Ha EJ, Cho WS, Kim SK, Kim JE. Clinical outcome of nonfistulous cerebral varices: The analysis of 39 lesions. J Korean Neurosurg Soc. 2018. 61: 485-93
6. Lasjaunias P, Terbrugge K, Rodesch G, Willinsky R, Burrows P, Pruvost P. True and false cerebral venous malformations. Venous pseudo-angiomas and cavernous hemangiomas. Neurochirurgie. 1989. 35: 132-9
7. Noran HH. Intracranial vascular tumors and malformations. Arch Pathol. 1945. 39: 393-416
8. Ozturk M, Aslan S, Ceyhan Bilgici M, Idil Soylu A, Aydin K. Spontaneous thrombosis of a giant cerebral varix in a pediatric patient. Childs Nerv Syst. 2017. 33: 2193-5
9. Shibata Y, Hyodo A, Tsuboi K, Yoshii Y, Nose T. Isolated cerebral varix with magnetic resonance imaging findings-case report. Neurol Med Chir (Tokyo). 1991. 31: 156-8
10. Tan ZG, Zhou Q, Cui Y, Yi L, Ouyang Y, Jiang Y. Extra-axial isolated cerebral varix misdiagnosed as convexity meningioma: A case report and review of literatures. Medicine (Baltimore). 2016. 95: e4047
11. Tanohata K, Maehara T, Noda M, Katoh H. Isolated cerebral varix of superficial cortical vein: CT demonstration. J Comput Assist Tomogr. 1986. 10: 1073-4
12. Tyson GW, Jane JA, Strachan WE. Intracerebral hemorrhage due to ruptured venous aneurysm. Report of two cases. J Neurosurg. 1978. 49: 739-43
13. Viñuela F, Drake CG, Fox AJ, Pelz DM. Giant intracranial varices secondary to high-flow arteriovenous fistulae. J Neurosurg. 1987. 66: 198-203

