

- Department of Neurosurgery, Cannizzaro Hospital, Sicily, Italy,
- Department of Neurosurgery, Highly Specialized Hospital and of National Importance “Garibaldi,” Catania, Sicily, Italy,
- Department of Neurosurgery and Institute of Intensive Care Medicine, University Hospital and University of Zürich, Zurich, Switzerland,
- Department of Pathological Anatomy, Cannizzaro Hospital, Catania, Italy.
Correspondence Address:
Giuseppe Emmanuele Umana, Department of Neurosurgery, Cannizzaro Hospital, Via Messina, 829, Catania - 95126, Sicily, Italy.
DOI:10.25259/SNI_504_2021
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Maurizio Passanisi1, Gianluca Scalia2, Paolo Palmisciano1, Daniele Franceschini1, Antonio Crea1, Crescenzo Capone3, Maria Grazia Tranchina4, Giovanni Federico Nicoletti2, Salvatore Cicero1, Giuseppe Emmanuele Umana1. Difficulty differentiating between a posterior extradural lumbar tumor versus sequestered disc even with gadolinum-enhanced MRI. 07-Jun-2021;12:267
How to cite this URL: Maurizio Passanisi1, Gianluca Scalia2, Paolo Palmisciano1, Daniele Franceschini1, Antonio Crea1, Crescenzo Capone3, Maria Grazia Tranchina4, Giovanni Federico Nicoletti2, Salvatore Cicero1, Giuseppe Emmanuele Umana1. Difficulty differentiating between a posterior extradural lumbar tumor versus sequestered disc even with gadolinum-enhanced MRI. 07-Jun-2021;12:267. Available from: https://surgicalneurologyint.com/surgicalint-articles/10860/
Date of Submission
20-May-2021
Date of Acceptance
25-May-2021
Date of Web Publication
07-Jun-2021
Abstract
Background: Differentiating between posterior extradural tumors versus sequestered lumbar disc herniations may be difficult even utilizing contrast-enhanced MR scans.
Case Description: A 49-year-old male acutely presented with an incomplete cauda equine syndrome. When the MRI showed a L4-L5 posterior extradural lesion that enhanced with gadolinium, an urgent left hemilaminectomy was performed. The lesion proved to be a sequestrated disc herniation rather than a tumor. Notably, postoperatively the patient almost completely recovered after 6-month follow-up.
Conclusion: Even on contrast-enhanced MRI studies, posterior extradural sequestered lumbar disc herniations may mimic tumors.
Keywords: Cauda equina, Low back pain, Lumbar disc, Posterior epidural migration, MRI
INTRODUCTION
Posterior extradural sequestered lumbar disc herniations (PESLDH) are rare. As per they typically occur in middle-aged males at the L3-L4 level where they result in cauda equine compression.[
CASE REPORT
Medical history and physical examination
A 49-years-old male, with a history of trauma, had low back pain of 6 months’ duration but presented with 4 weeks of paraparesis (numbness/weakness), and 10 days of bladder dysfunction.
He exhibited an incomplete cauda equine syndrome, 2/5 in the left leg, 3/5 on the right, mild saddle hypoesthesia, and severe bilateral hypoesthesia below L5.
Radiological studies
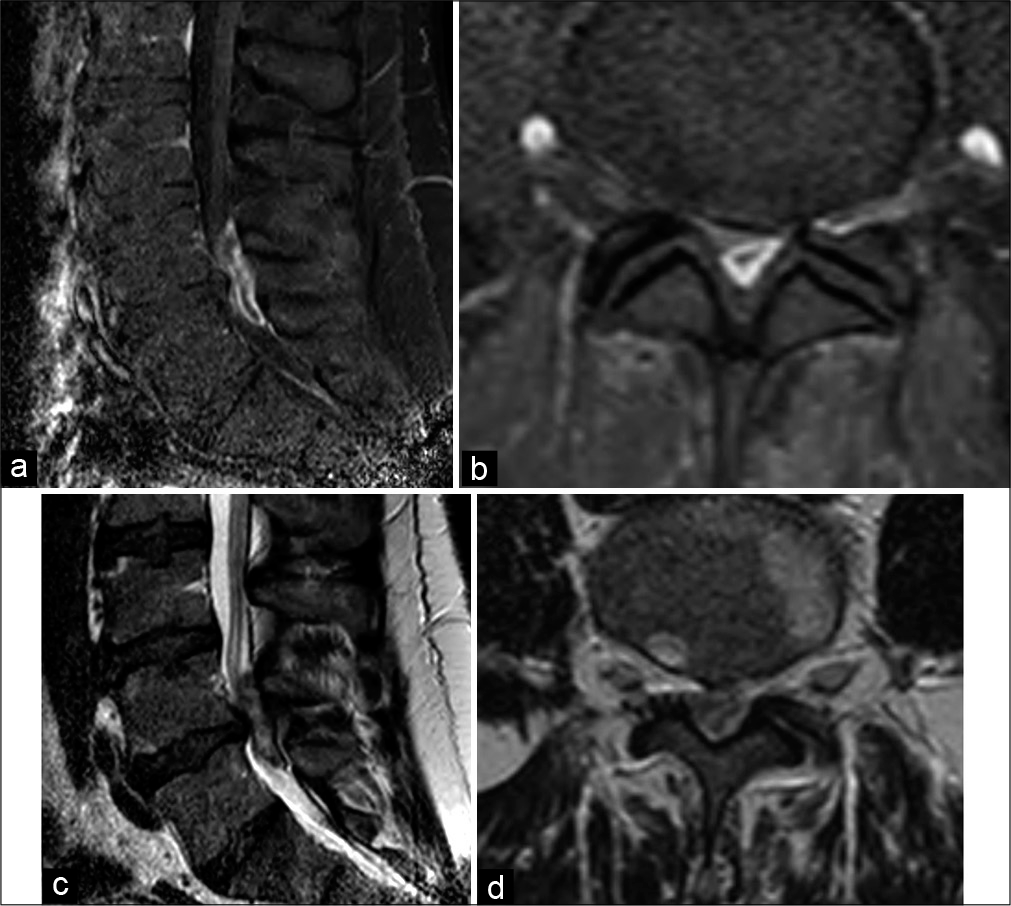
The lumbosacral MR showed a compressive posterior L4-L5 extradural lesion (i.e. iso/hypointense on T1-weighted sequences and hypointense on T2-weighted sequences); it markedly enhanced with contrast (Gadolinium DTPA) [
Surgical procedure and outcome
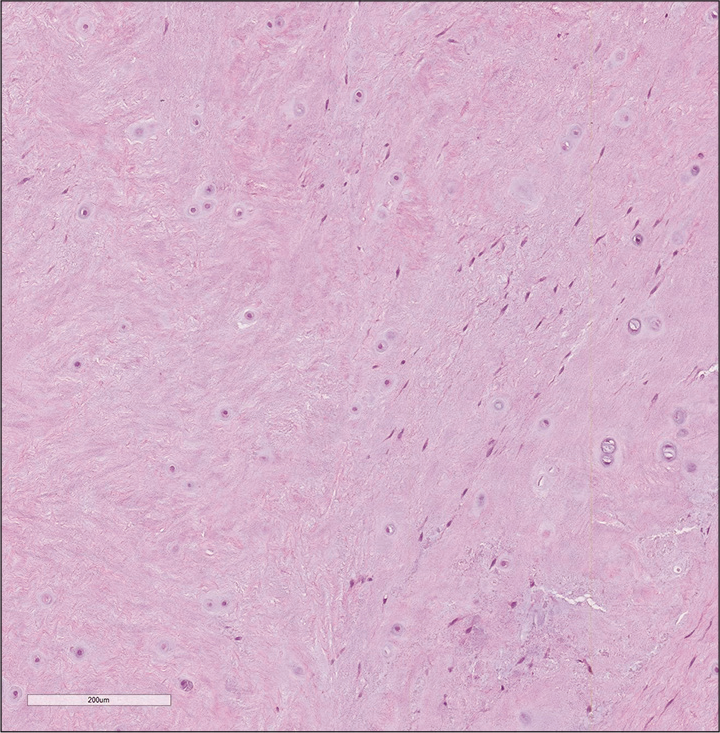
A left-sided hemilaminectomy was performed at the L4-L5 level and revealed atypical, extruded disc fragment that was microsurgically removed [
DISCUSSION
PESLDHs frequently occur in middle-aged males with a chronic history of manual labor, heavy lifting, and/or a recent history of trauma. In 39.2% of cases, the discs are ventrally located at the L3-L4 level; however, posterior herniations are also rarely reported.[
CONCLUSION
Posterior extradural compressive lesions that enhance on contrast MR studies may include tumors, cysts, or sequestered lumbar disc herniations. Based on clinical symptoms, signs, routine decompression, and pathological confirmation of the diagnosis are essential to appropriate management.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Chen CY, Chuang YL, Yao MS, Chiu WT, Chen CL, Chan WP. Posterior epidural migration of a sequestrated lumbar disk fragment: MR imaging findings. AJNR Am J Neuroradiol. 2006. 27: 1592-4
2. Deora H, Prabhuraj AR, Pruthi N. Posterior epidural migration of lumbar disc: Will the real “disc” please stand up?. Surg Neurol Int. 2017. 8: 302
3. Elgamri A, Sami A, Aqqad A, Hilmani S, Ibahioin K, Naja A. Posterior migration of a lumbar disc herniation as a cause of cauda equina syndrome. J Radiol. 2009. 90: 731-3
4. Lombardi V. Lumbar spinal block by posterior rotation of anulus fibrosus. Case report. J Neurosurg. 1973. 39: 642-7
5. Turan Y, Yilmaz T, Gocmez C, Ozevren H, Kemaloglu S, Teke M. Posterior epidural migration of a sequestered lumbar intervertebral disc fragment. Turk Neurosurg. 2017. 27: 85-94

