

- Department of Neurosurgery, Shinshu University School of Medicine, Matsumoto, Japan
- Unit of Neurosurgery, Memfys Hospital for Neurosurgery, Enugu, Nigeria
Correspondence Address:
Tetsuyoshi Horiuchi
Unit of Neurosurgery, Memfys Hospital for Neurosurgery, Enugu, Nigeria
DOI:10.4103/sni.sni_81_18
Copyright: © 2018 Surgical Neurology International This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.How to cite this article: Sunday Nkwerem, Tetsuyoshi Horiuchi, Akihiro Nishikawa, Kiyoshi Ito, Kazuhiro Hongo, Samuel Ohaegbulam. Diploic mature teratoma originating from the orbital roof: An extremely rare case report. 26-Jul-2018;9:151
How to cite this URL: Sunday Nkwerem, Tetsuyoshi Horiuchi, Akihiro Nishikawa, Kiyoshi Ito, Kazuhiro Hongo, Samuel Ohaegbulam. Diploic mature teratoma originating from the orbital roof: An extremely rare case report. 26-Jul-2018;9:151. Available from: http://surgicalneurologyint.com/surgicalint-articles/diploic-mature-teratoma-originating-from-the-orbital-roof-an-extremely-rare-case-report/
Date of Submission
13-Mar-2018
Date of Acceptance
27-Jun-2018
Date of Web Publication
26-Jul-2018
Abstract
Background:Orbital mature teratoma is a rare congenital tumor.
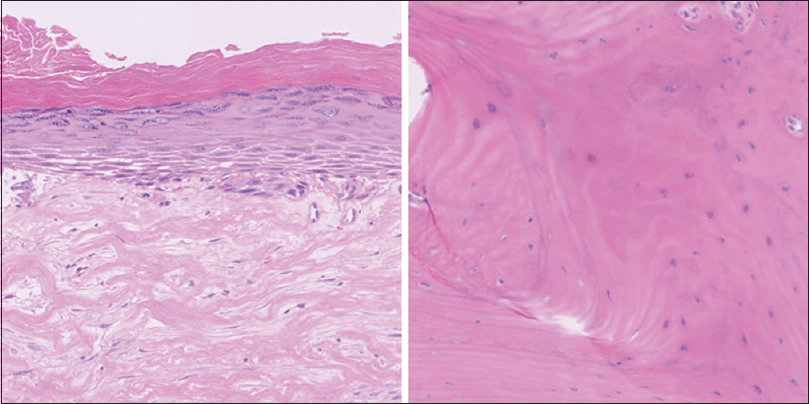
Case Description:A 37-year-old woman presented with ophthalmalgia predated by years of progressive incongruous right eye position, diplopia, and restricted extraocular movement. Neuroimages revealed a right orbital mass originating from the orbital roof. After resection, histopathology revealed the mature teratoma.
Conclusion:To the authors’ best knowledge, this is the first documented diploic origin of mature teratoma at the orbital roof.
Keywords: Diplopic origin, orbit, teratoma
INTRODUCTION
Craniofacial teratomas are rare tumors and they are believed to be congenital lesions due to the abnormal distribution of germ cells during the 3rd to 5th weeks of gestation.[
Orbital teratomas account for 1% of all orbital tumors in childhood and are usually localized within orbit and without bony involvement.[
CASE HISTORY
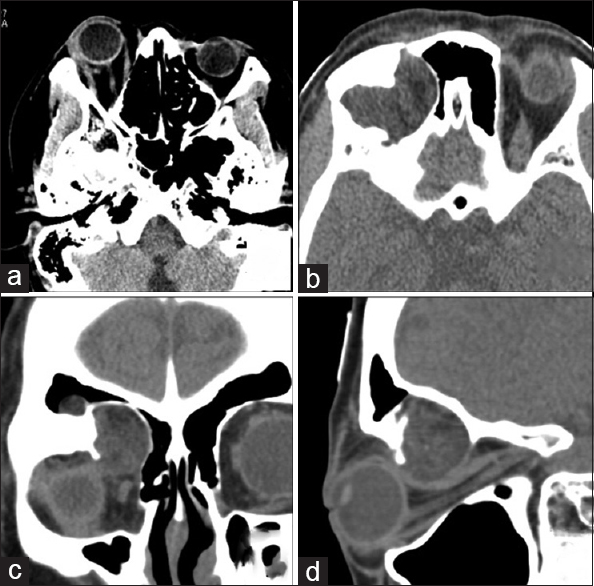
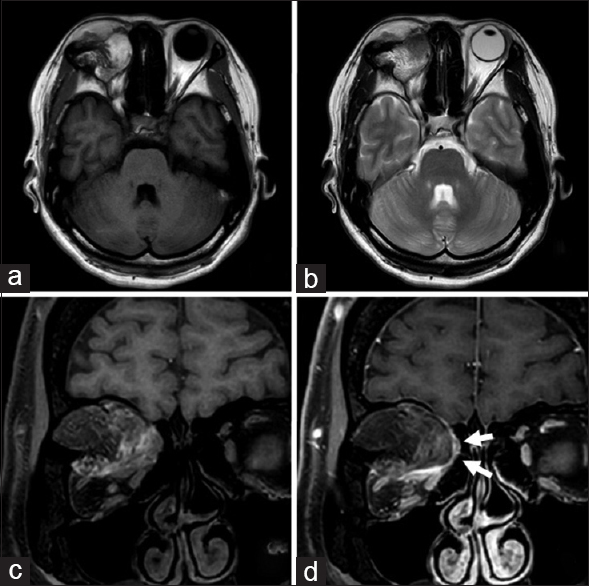
A 37-year-old woman presented with a history of right eye pain of few days duration. There was, however, a background history of incongruous position of her eyes and diplopia of over 10 years duration. The protrusion was noted to have worsened weeks leading to presentation to a hospital where cranial computed tomography (CT) and magnetic resonance imaging (MRI) showed a right orbital mass causing exophthalmos. The mass was partly enhanced and it was predominantly intraosseous located at the orbital roof [Figures
DISCUSSION
Here, we report a rare case of mature teratoma that originated from the diploic orbital roof. Orbital teratomas are rare, usually presenting with unilateral proptosis of eyeball in neonates.[
In general, orbital mature teratomas are purely orbital location without intracranial involvement.[
The mature teratoma usually consists of solid tissues with encapsulated cyst. Radiologic features of mature teratoma are nonspecific because they depend on containing different well-differentiated components such as soft tissue, cartilage, or bone. Therefore, mature teratomas have mixed density and intensity on computed tomography and magnetic resonance imaging, respectively, whereas contrast enhancement is variable.[
Complete resection for mature teratoma leads to a surgical cure and prognosis is good.[
CONCLUSION
An extremely rare case of diploic mature teratoma arising from the orbital roof was presented.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Anderson PJ, David DJ. Teratomas of the head and neck region. J Craniomaxillofac Surg. 2003. 31: 369-77
2. Grube-Pagola P, Hobart-Hernandez RI, Martinez-Hernandez MA, Gomez-Dorantes SM, Alderete-Vazquez G. Congenital proptosis secondary to orbital teratoma. Clinicopathological study. Arch Soc Esp Oftalmol. 2013. 88: 153-6
3. Kharosekar HU, Jasmit S, Velho V, Palande DA. Congenital orbital teratoma up to posterior fossa. J Pediatr Neurosci. 2014. 9: 182-4
4. Lloret I, Server A, Taksdal I. Calvarial lesions: A radiological approach to diagnosis. Acta Radiol. 2009. 50: 531-42
5. Morris DS, Fayers T, Dolman PJ. Orbital teratoma: Case report and management review. J AAPOS. 2009. 13: 605-7
6. Selcuki M, Attar A, Yuceer N, Tuna H, Cakiroglu E. Mature teratoma of the lateral ventricle: Report of two cases. Acta Neurochir (Wien). 1998. 140: 171-4
7. Zhao J, Wang H, Yu J, Zhong Y, Ge P. Cerebral falx mature teratoma with rare imaging in an adult. Int J Med Sci. 2012. 9: 269-73

