

- Department of Surgery, Federal Teaching Hospital, Ido Ekiti/Afe Babalola University, Ado Ekiti, Nigeria.
- Department of Anaesthesia, Federal Teaching Hospital, Ido Ekiti/Afe Babalola University, Ado Ekiti, Nigeria.
- Department of Medicine, Federal Teaching Hospital, Ido Ekiti, Nigeria.
- Department of Orthopaedic Surgery and Trauma, Afe Babalola University, Ado Ekiti, Nigeria.
Correspondence Address:
Abiodun Idowu Okunlola
Department of Orthopaedic Surgery and Trauma, Afe Babalola University, Ado Ekiti, Nigeria.
DOI:10.25259/SNI_840_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Abiodun Idowu Okunlola1, Tesleem Olayinka Orewole2, Cecilia Kehinde Okunlola3, Olakunle Fatai Babalola1, Akinola Akinmade4. Epidural lipomatosis in elderly patient: A rare cause of cauda equina compression. 05-Jan-2021;12:7
How to cite this URL: Abiodun Idowu Okunlola1, Tesleem Olayinka Orewole2, Cecilia Kehinde Okunlola3, Olakunle Fatai Babalola1, Akinola Akinmade4. Epidural lipomatosis in elderly patient: A rare cause of cauda equina compression. 05-Jan-2021;12:7. Available from: https://surgicalneurologyint.com/surgicalint-articles/10508/
Date of Submission
22-Nov-2020
Date of Acceptance
15-Dec-2020
Date of Web Publication
05-Jan-2021
Abstract
Background: The most common cause of cauda equina compression in the elderly is lumbar spinal stenosis. Epidural lipomatosis is an additional known but rare cause of cauda equina compression readily diagnosed on MR studies. Notably, spinal canal decompression and direct excision of the epidural fat effectively manage this combined pathology.
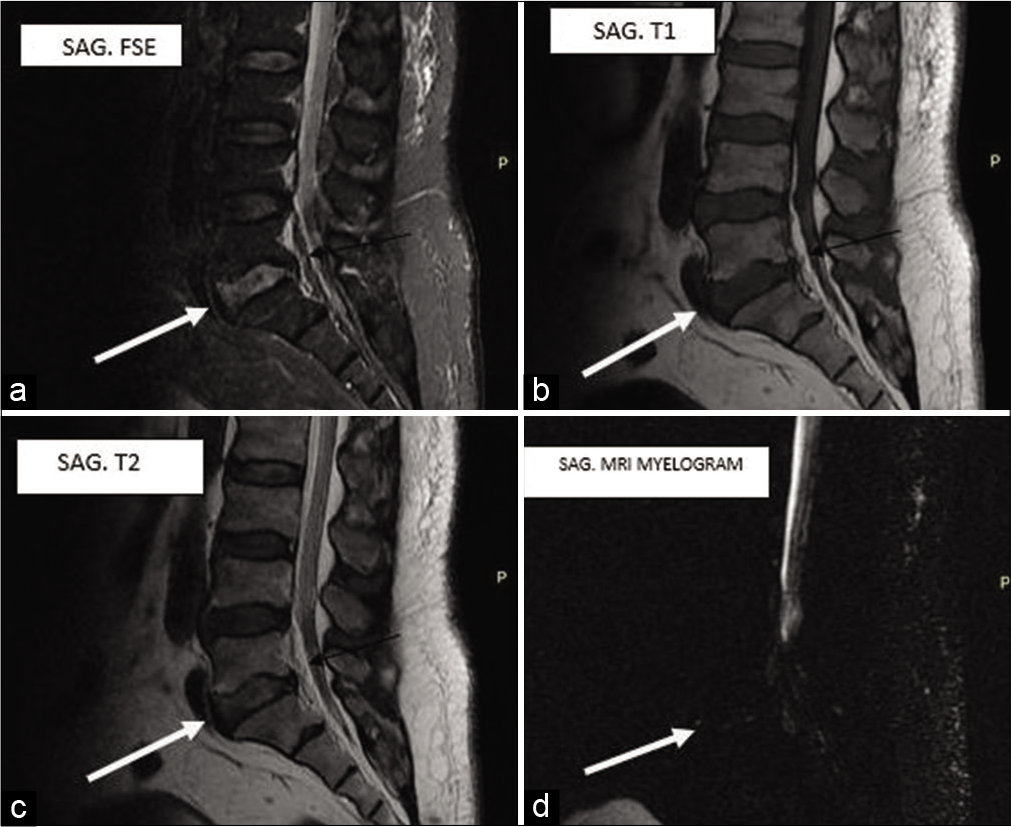
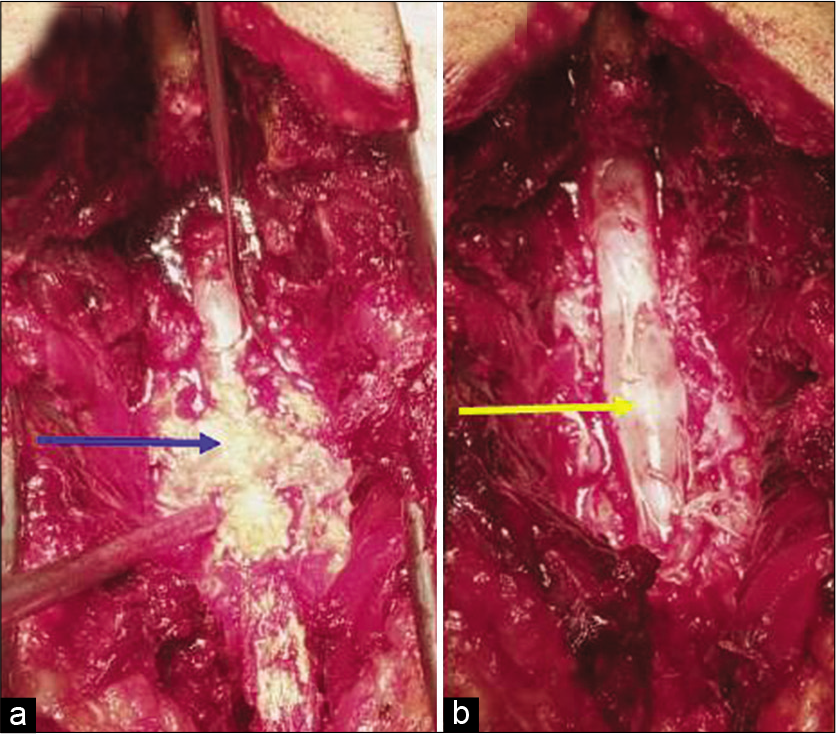
Case Description: A 70-year-old male presented with progressive truncal obesity associated with refractory lumbar neurogenic claudication. The lumbar magnetic resonance imaging (MRI) showed excessive epidural fat extending from L4 to S2 resulting in thecal sac compression; this was confirmed on the MRI myelogram study. Following a decompressive laminectomy, the patient’s cauda equina syndrome resolved.
Conclusion: Recent weight gain with increased neurogenic claudication and the onset of a cauda equina syndrome may herald the presence of significant lumbar epidural lipomatosis. Here, laminectomy for excision of the excessive epidural fat resolved the patient’s symptomatic spinal stenosis.
Keywords: Cauda equina compression, Epidural fat, Low back pain, Neurogenic claudication
INTRODUCTION
Symptomatic cauda equina compression secondary to excessive epidural fat is occasionally seen in elderly patients and is readily documented on MR studies.[
CASE REPORT
A 70-year-old male presented with 6 years of increased weight gain, progressive low back pain with bilateral radiculopathy, and the newer exacerbation of neurogenic claudication. On examination, he had marked truncal obesity (body mass index = 35 Kg/m2 and waist–hip ratio of 1), straight leg raising was limited to 50° bilaterally, motor function remained intact in both lower extremities (e.g., 5/5 bilaterally), bilateral Achilles responses were absent, and he exhibited no focal sensory deficit.
The lumbosacral magnetic resonance imaging (MRI) showed excessive epidural fat with significant thecal sac compression extending from L4 to S2; this was further confirmed on the MRI myelogram [
DISCUSSION
In this case study, a 70-year-old male presented with the recent rapid onset of weight gain, lumbar radiculopathy and progressive neurogenic claudication.[
Notably, in Zevgaridis et al. study, MRI readily documented the presence of epidural lipomatosis/lumbar thecal sac compression, making obtaining a myelo-CT study unnecessary.[
In the majority of cases, surgical excision of epidural lipomatosis in conjunction with decompressing lumbar spinal stenosis is the treatment of choice to relieve cauda equina compression.
CONCLUSION
Recent weight gain associated with lumbar stenosis and progressive neurogenic claudication attributed to MR documented epidural lipomatosis may be effectively relieved with a decompressive laminectomy.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Fogel GR, Cunningham PY, Esses SI. Spinal epidural lipomatosis: Case reports, literature review and meta-analysis. Spine J. 2005. 5: 202-11
2. Kim K, Mendelis J, Cho W. Spinal Epidural lipomatosis: A review of pathogenesis, characteristics, clinical presentation, and management. Global Spine J. 2019. 9: 658-65
3. Malone JB, Bevan PJ, Lewis TJ, Nelson AD, Blaty DE, Kahan ME. Incidence of spinal epidural lipomatosis in patients with spinal stenosis. J Orthop. 2018. 15: 36-9
4. Park SK, Han JM, Lee K, Cho WJ, Oh JH, Choi YS. The clinical characteristics of spinal epidural lipomatosis in the lumbar spine. Anesth Pain Med. 2018. 8: e83069
5. Reina MA, Franco CD, López A, dé Andrés JA, van ZundertA. Clinical implications of epidural fat in the spinal canal. A scanning electron microscopic study. Acta Anaesthesiol Belg. 2009. 60: 7-17
6. Walker MA, Younan Y, de la Houssaye C, Reimer N, Robertson DD, Umpierrez M. Volumetric evaluation of lumbar epidural fat distribution in epidural lipomatosis and back pain in patients who are obese: Introducing a novel technique (Fat Finder algorithm). BMJ Open Diabetes Res Care. 2019. 7: e000599
7. Yasuda T, Suzuki K, Kawaguchi Y, Seki S, Makino H, Watanabe K. Clinical and imaging characteristics in patients undergoing surgery for lumbar epidural lipomatosis. BMC Musculoskelet Disord. 2018. 19: 66
8. Zevgaridis D, Nanassis K, Zaramboukas T. Lumbar nerve root compression due to extradural, intraforaminal lipoma, An underdiagnosed entity? Case report. J Neurosurg Spine. 2008. 9: 408-10

