

- Department of Neurosurgery, UPMC, Pittsburgh, Pennsylvania, USA
- Department of Anesthesiology, UPMC, Pittsburgh, Pennsylvania, USA
- Wayne State University School of Medicine, Detroit, Michigan, USA
Correspondence Address:
Matt El-Kadi
Wayne State University School of Medicine, Detroit, Michigan, USA
DOI:10.4103/2152-7806.191075
Copyright: © 2016 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: El-Kadi M, Ibinson J, Donovan E, Sullivan D, Kadi R. Factors influencing the length of stay in patients with lumbar pedicle screw fixation. Surg Neurol Int 22-Sep-2016;7:
How to cite this URL: El-Kadi M, Ibinson J, Donovan E, Sullivan D, Kadi R. Factors influencing the length of stay in patients with lumbar pedicle screw fixation. Surg Neurol Int 22-Sep-2016;7:. Available from: http://surgicalneurologyint.com/surgicalint_articles/factors-influencing-length-stay-patients-lumbar-pedicle-screw-fixation/
Abstract
Background:Current health care practices aim for cost reduction to achieve maximal benefit. Because of the increasing number of spinal fusions, this area has become a target for both hospitals and payment organizations. Length of stay (LOS) is one potentially modifiable variable to help reduce overall cost. Attempting to predict the LOS in spinal surgery based on patient factors has not revealed a set of variables that are consistently associated with increased stay.
Methods:Medical records from all patients who underwent posterior lumbar spinal fusion by a single neurosurgeon at a single facility were retrospectively examined in a blind fashion. Data were obtained including age, gender, body mass index (BMI), American society of Anesthesiologists (ASA) and analyzed to determine a potential relationship with LOS.
Results:A total of 1360 patients were identified for analysis. There were significant but small correlations between age, ASA, BMI, and LOS.
Conclusions:There is an effect of age, ASA, and BMI on LOS. However, the significance of this effect is small. Future studies aiming to identify additional factors, which could potentially be modifiable, in order to work on decreasing LOS in lumbar spinal fusion patients.
Keywords: Age, American society of Anesthesiologists, length of stay, lumbar fusion, obesity
INTRODUCTION
The changing climate in the health care industry is placing more focus on decreasing both the hospital stay and cost. An analysis of national health spending in 2004 found that although the rate of growth for overall spending slightly slowed to 7.9%, hospital spending continued to steadily increase. An analysis by Goz et al. revealed that the numbers of spinal fusion surgeries performed in the United States are increasing over time, with lumbar spinal fusions increasing at the greatest pace.[
The goal of this retrospective analysis was to use our large database to definitively examine age, body mass index (BMI), and American society of Anesthesiologists (ASA) score as preoperative factors associated with an increased LOS in lumbar fusion patients. By definition, ASA score classifies patients into groups based on the overall medical condition. Therefore, our primary hypothesis was that a higher ASA score will be associated with increasing LOS. Secondary hypotheses were that increasing age and BMI may be associated with an increased LOS following lumbar spine fusion.
MATERIALS AND METHODS
Data source
After obtaining the appropriate institutional review board review, the medical records from all patients who underwent posterior instrumented lumbar spinal fusion from January 1, 2008 through July 31, 2014 were examined in a retrospective, blind fashion. All the patients underwent lumbar fusion by a single neurosurgeon at a single facility. Patients who met the criteria were pulled out of the electronic record based on a search by procedure codes. The information was entered by one coinvestigator and coded to maintain its integrity. All patients who met the criteria of undergoing instrumented posterior lumbar fusion were included in the database.
Patient data
Patient data including age, gender, BMI, and medical comorbidities were recorded, along with the ASA class. While the presence or absence of litigation and work injury/motor vehicle accident and variables related to the inpatient stay (including estimated blood loss and postoperative complications) were recorded, only age, BMI, and ASA class were tested to focus on our main hypotheses. LOS was noted for each patient and divided into three categories based on clinical significance and average stay.
Statistical tests
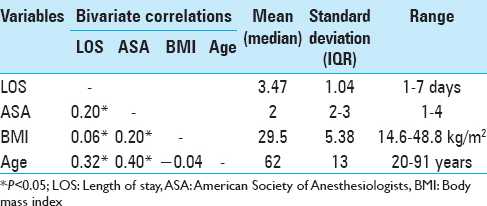
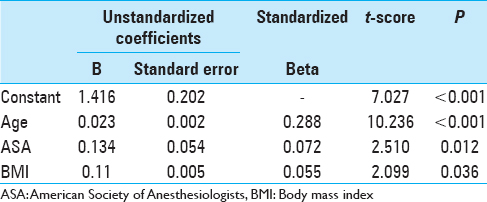
Descriptive statistics are presented using mean and standard deviation for the continuous variables of LOS, age, and BMI. ASA class is presented as median and interquartile range (because it is ordinal data). The presence of a relationship between LOS and age and BMI and ASA class was tested using multiple linear regression. A constant term was included in the model because all patients required some LOS. A forward model building strategy was used with the Probability-of-F-to enter <=0.050 set as the criterion for model entry.
RESULTS
A total of 1360 cases were identified. Descriptive statistics and bivariate correlations are presented in
DISCUSSION
The influence of patient variables on the length of hospital stay has been evaluated in an attempt to reduce the overall financial burden associated with these procedures. In this study, patients underwent lumbar fusion by one surgeon at one facility, thus eliminating some of the possible variability. As
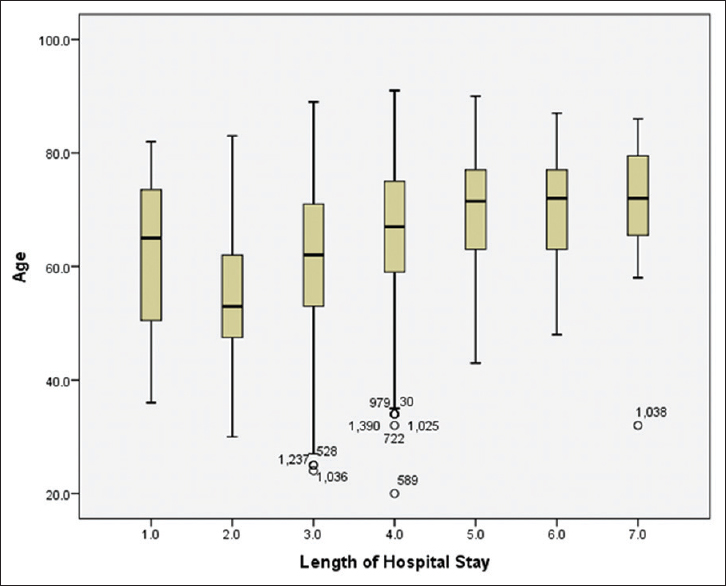
Age
There are conflicting reports in the literature regarding the predictive value of age for LOS following lumbar fusion.[
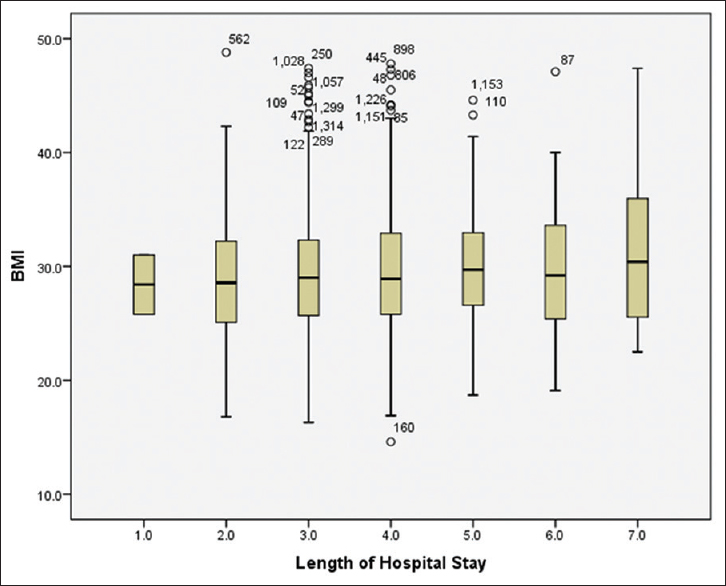
Body mass index
The possible effect of BMI on LOS has also been debated.[
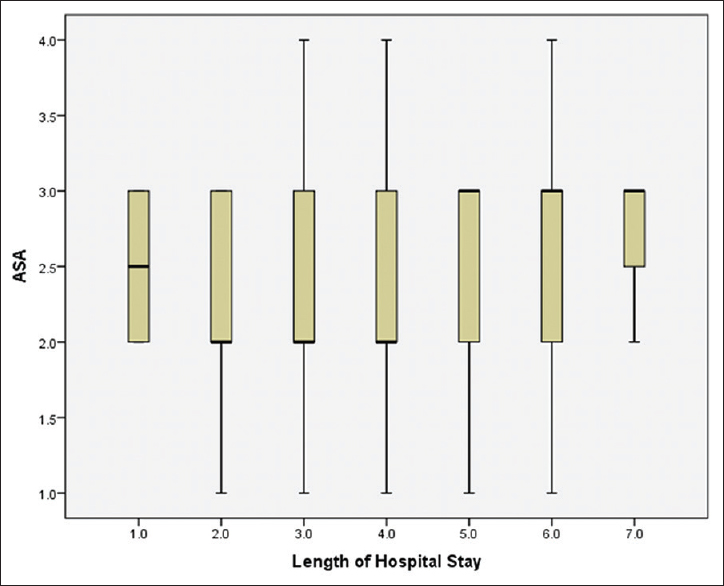
American society of Anesthesiologists
The association between ASA class and LOS has been deliberated, as well as which ASA class may have an effect.[
Additional factors
Given that age, BMI, and ASA class explained only approximately 10% of the variation in LOS, it is likely that intraoperative and/or postsurgical factors would be the logical next targets for analysis. Chief among these may be patient function and walking distance.[
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Cassinelli EH, Eubanks J, Vogt M, Furey C, Yoo J, Bohlman HH. Risk factors for the development of perioperative complications in elderly patients undergoing lumbar decompression and arthrodesis for spinal stenosis: An analysis of 166 patients. Spine. 2007. 32: 230-5
2. De la Garza-Ramos R, Bydon M, Abt NB, Sciubba DM, Wolinsky JP, Bydon A. The impact of obesity on short- and long-term outcomes following lumbar fusion. Spine. 2015. 40: 56-61
3. El-Kadi M, Donovan E, Al Halabi T, Khattar N, El-Kadi M, Macoskey M. Minimizing complications and decreasing hospital stay in obese patients. Contemp Neurosurg. 2013. 23: 1-6
4. Eleswarapu A, Mikhael MM, Koh JL. Number of recent inpatient admissions as a risk factor for increased complications, length-of-stay, and cost in patients undergoing posterior lumbar fusion. Spine. 2014. 39: 2148-56
5. Goz V, Weinreb JH, McCarthy I, Schwab F, Lafage V, Errico TJ. Perioperative complications and mortality after spinal fusions: Analysis of trends and risk factors. Spine. 2013. 38: 1970-6
6. Kanaan SF, Waitman LR, Yeh HW, Arnold PM, Burton DC, Sharma NK. Structural equation model analysis of the length-of-hospital stay after lumbar spine surgery. Spine J. 2015. 15: 612-21
7. Kalanithi PA, Arrigo R, Boakye M. Morbid obesity increases cost and complication rates in spinal arthrodesis. Spine. 2012. 37: 982-8
8. Rosen DS, Ferguson SD, Ogden AF, Huo D, Fessler RG. Obesity and self-reported outcome after minimally invasive lumbar spinal fusion surgery. Neurosurgery. 2008. 63: 956-60
9. Schoenfeld AJ, Carey PA, Cleveland AW, Bader JO, Bono CM. Patient factors, comorbidities, and surgical characteristics that increase mortality and complication risk after spinal arthrodesis: A prognostic study based on 5887 patients. Spine J. 2013. 13: 1171-9
10. Siemionow K, Pelton MA, Hoskins JA, Singh K. Predictive factors of hospital stay in patients undergoing minimally invasive transforminal lumbar interbody fusion and instrumentation. Spine. 2012. 37: 2046-54
11. Yadla S, Malone J, Campbell PG, Maltenfort MG, Sharan AD, Harrop JS. Preoperative diagnosis and early complications in thoracolumbar spine surgery: A single center prospective study. J Spinal Disord Tech. 2011. 24: E16-20
12. Zheng F, Cammisa FP, Sandhu HS, Girardi FP, Khan SN. Factors predicting hospital stay, operative time, blood loss, and transfusion in patient sundergoing revision posterior lumbar spine decompression, fusion, and segmental instrumentation. Spine. 2002. 27: 818-24

