

- Department of Neurosurgery, Gomez Ulla Central Defence Hospital,
- Department of Neurosurgery, Fundación Jiménez Díaz University Hospital, Madrid, Spain.
Correspondence Address:
Pierre Ferrer, Gomez Ulla Central Defence Hospital, Madrid, Spain.
DOI:10.25259/SNI_656_2021
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Pierre Ferrer1, Ana Sofía Álvarez2, Sara Khalil2. Gastric balloon: A rare cause of lumbar radiculopathy. 09-Aug-2021;12:398
How to cite this URL: Pierre Ferrer1, Ana Sofía Álvarez2, Sara Khalil2. Gastric balloon: A rare cause of lumbar radiculopathy. 09-Aug-2021;12:398. Available from: https://surgicalneurologyint.com/surgicalint-articles/11030/
Date of Submission
30-Jun-2021
Date of Acceptance
17-Jul-2021
Date of Web Publication
09-Aug-2021
Abstract
Background: Factors that are known to cause lumbar epidural venous plexus (EVP) engorgement include inferior vena cava (IVC) obstruction, portal hypertension, vascular agenesis, morbid obesity, and/or hypercoagulable states. Here, we present a 32-year-old female admitted with the new onset of lumbar radiculopathy attributed to a gastric balloon causing compression of the IVC and engorgement of the EVP.
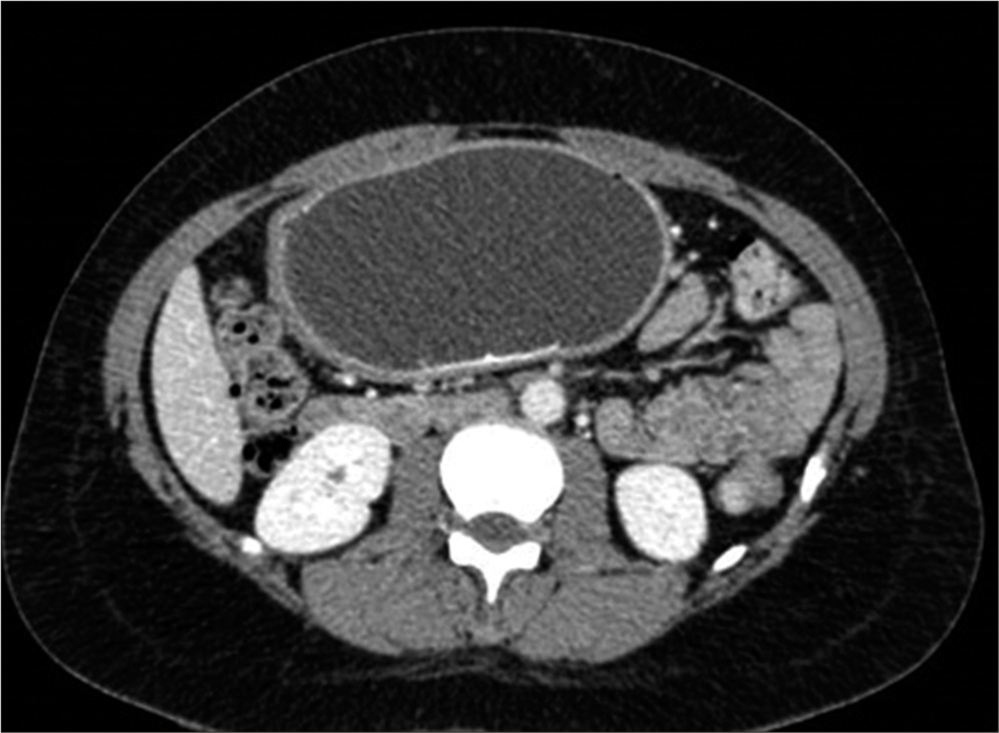
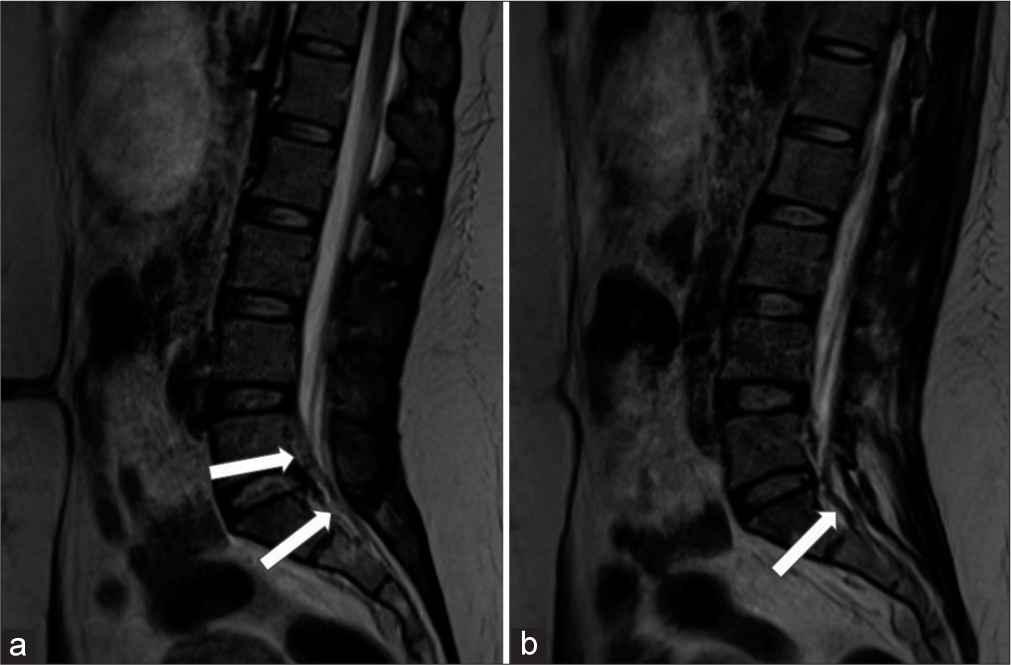
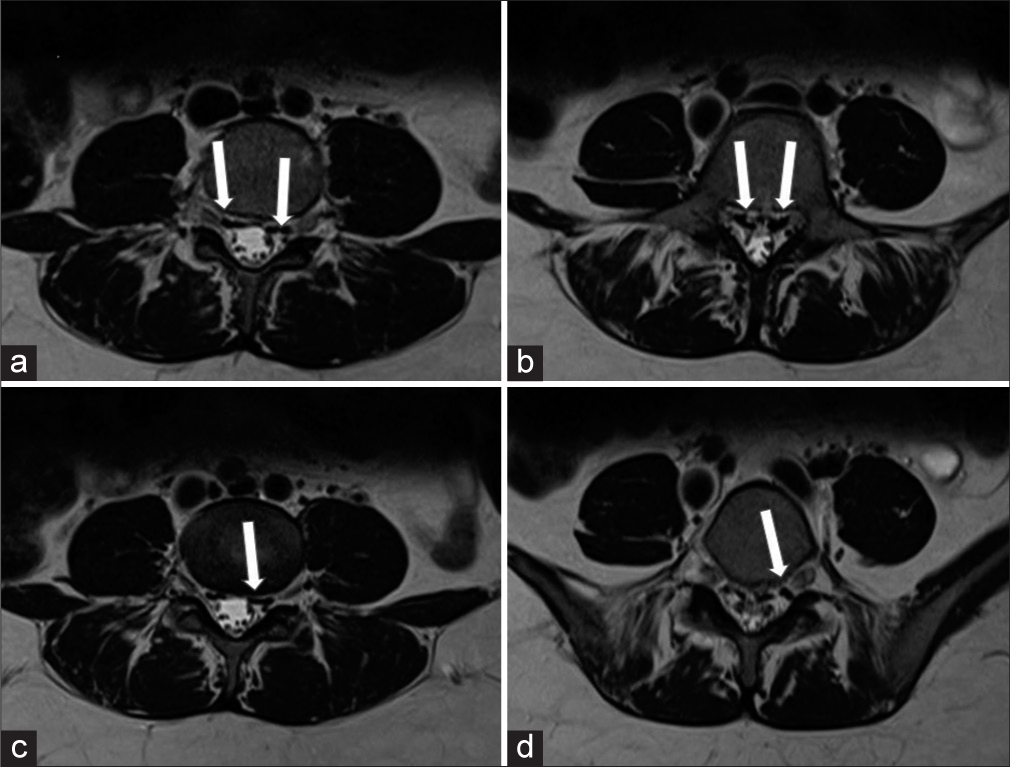
Case Description: A 32-year-old female was admitted with a left L5 radiculopathy. She had a history of morbid obesity and had undergone intragastric balloon insertion 4 months ago. The abdominal/pelvic CT documented an intragastric balloon producing a voluminous gastric mass with resultant compression of the IVC. The lumbar MRI showed the resultant marked multilevel engorgement of the lumbar EVP. Here, following balloon removal, the patient was immediately symptom free and remained asymptomatic over the next postoperative year.
Conclusion: An intragastric balloon can produce a voluminous gastric mass that can result in IVC occlusion and engorgement of the EVP, leading to lumbar radiculopathy. Removal of the balloon results in immediate and permanent resolution of the compressive symptoms.
Keywords: Epidural venous plexus, Gastric balloon, Inferior vena cava compression, Radiculopathy
INTRODUCTION
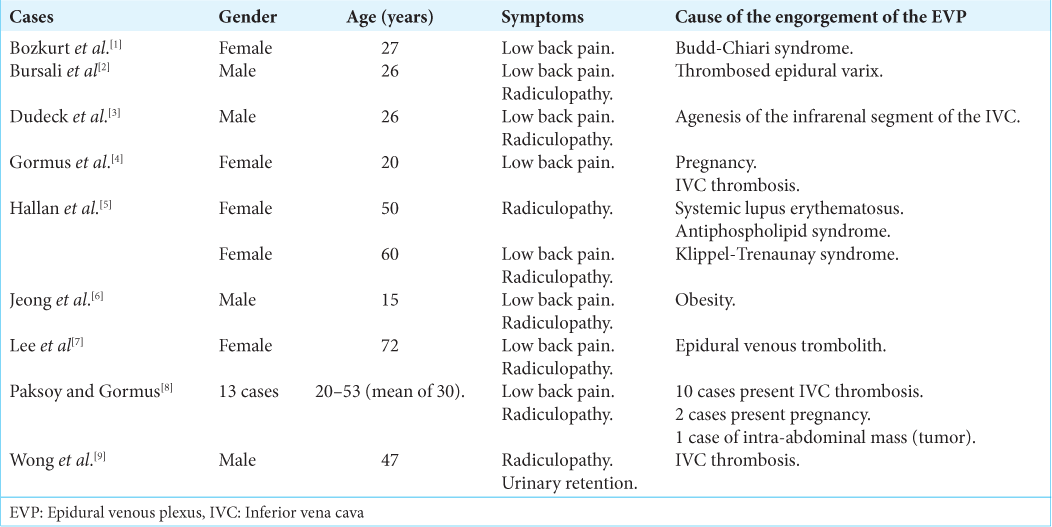
There are multiple causes of engorgement of the lumbar epidural venous plexus (EVP); including inferior vena cava (IVC) obstruction; portal hypertension, vascular agenesis, morbid obesity, pregnancy, intra-abdominal mass, Budd-Chiari syndrome, or hypercoagulable states.[
Gastric balloons should now be added to the list, as they too can lead to marked gastric distention with resultant IVC compression and massive lumbar EVP engorgement resulting in radiculopathy.
CASE DESCRIPTION
A 32-year-old female with morbid obesity had undergone an intragastric balloon insertion 4 months ago. She is now presented with the left L5 distribution leg pain and dysesthesias/ paresthesias of 3 months’ duration, exacerbated in the supine position. On examination, she had 4/5 weakness involving the left L5/S1 distributions (i.e. extensor hallucis longus/dorsiflexors and plantar flexors).
Diagnostic study
The abdominal CT scan and lumbar MRI showed a voluminous gastric mass attributed to the gastric balloon that compressed the IVC [
Following urgent removal of the balloon, the patient was asymptomatic and remained symptoms free 1 year later.
DISCUSSION
Anatomy of Batson’s plexus
A gastric balloon resulting in marked gastric distention can produce IVC obstruction that can trigger engorgement of the EVP, causing root compression and radiculopathy. This is largely attributed to the fact that Batson’s EVP is a valveless network connected to the IVC, pelvic veins, and azygos system through multiple intersegmental branches traversing the intervertebral foramina adjacent to the spinal nerve roots.[
Engorgement of the IVC results in Sciatica
IVC compression (caused by hypercoagulable states, vascular thrombosis, obesity, vascular agenesis, malignant intra-abdominal mass, or pregnancy) or thrombosed epidural varices can compress spinal nerve roots resulting in radiculopathy [
Here, we reported a clear case of IVC obstruction leading to significant engorgement of the lumbar EVP resulting in neurological radiculopathy.
CONCLUSION
Here, we have described a unique iatrogenic complication of gastric balloon placement resulting in compression of the IVC and engorgement of the lumbar EVP responsible for lumbar radiculopathy.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Bozkurt G, Cil B, Akbay A, Türk CC, Palaoğlu S. Intractable radicular and low back pain secondary inferior vena cava stenosis associated with Budd-Chiari syndrome: Endovascular treatment with cava stenting: Case report and review of the literature. Spine (Phila Pa 1976). 2006. 31: E383-6
2. Bursalı A, Akyoldas G, Guvenal AB, Yaman O. Lumbar epidural varix mimicking disc herniation. J Korean Neurosurg Soc. 2016. 59: 410-3
3. Dudeck O, Zeile M, Poellinger A, Kluhs L, Ludwig WD, Hamm B. Epidural venous enlargements presenting with intractable lower back pain and sciatica in a patient with absence of the infrarenal inferior vena cava and bilateral deep venous thrombosis. Spine (Phila Pa 1976). 2007. 32: E688-91
4. Gormus N, Ustun ME, Paksoy Y, Ogun TC, Solak H. Acute thrombosis of inferior vena cava in a pregnant woman presenting with sciatica: A case report. Ann Vasc Surg. 2005. 19: 120-2
5. Hallan DR, McNutt S, Reiter GT, Thamburaj K, Specht CS, Knaub M. Dilated epidural venous plexus causing radiculopathy: A report of 2 cases and review of the literature. World Neurosurg. 2020. 144: 231-7
6. Jeong HJ, Sim WS, Park HJ, Lee SH, Oh MS, Cho MK. Severe lumbar radiculopathy with epidural venous plexus engorgement in a morbidly obese pediatric patient: A case report. Medicine (Baltimore). 2019. 98: e16842
7. Lee YS, Choi ES, Kim JO, Ji JH. A rare calcified thrombosis of the dilated epidural venous plexus presenting with lumbar radiculopathy: A case report. Spine J. 2011. 11: e28-31
8. Paksoy Y, Gormus N. Epidural venous plexus enlargements presenting with radiculopathy and back pain in patients with inferior vena cava obstruction or occlusion. Spine (Phila Pa 1976). 2004. 29: 2419-24
9. Wong TW, Gridley DG, Feiz-Erfan I. Epidural venous plexus engorgement due to inferior vena cava thrombosis resulting in cauda equina syndrome: Case report and literature review. Surg Neurol Int. 2018. 9: 129

