

- Department of Neurosurgery, Fuji Brain Institute and Hospital, Fujinomiya, Shizuoka, Japan
- Department of Neurosurgery, NTT Medical Center Tokyo, Tokyo, Japan
- Department of Neurosurgery, The University of Tokyo Hospital, Tokyo, Japan
Correspondence Address:
Hideaki Ono
Department of Neurosurgery, The University of Tokyo Hospital, Tokyo, Japan
DOI:10.4103/sni.sni_178_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Hideaki Ono, Tomohiro Inoue, Naoto Kunii, Takeo Tanishima, Akira Tamura, Isamu Saito, Nobuhito Saito. Giant cavernous carotid aneurysm causing pituitary dysfunction: Pituitary function recovery with high-flow bypass. 09-Aug-2017;8:180
How to cite this URL: Hideaki Ono, Tomohiro Inoue, Naoto Kunii, Takeo Tanishima, Akira Tamura, Isamu Saito, Nobuhito Saito. Giant cavernous carotid aneurysm causing pituitary dysfunction: Pituitary function recovery with high-flow bypass. 09-Aug-2017;8:180. Available from: http://surgicalneurologyint.com/surgicalint-articles/giant-cavernous-carotid-aneurysm-causing-pituitary-dysfunction-pituitary-function-recovery-with-high%e2%80%91flow-bypass/
Date of Submission
05-May-2017
Date of Acceptance
13-Jun-2017
Date of Web Publication
09-Aug-2017
Abstract
Background:Giant internal carotid artery (ICA) aneurysms extending into the sellar region, mimicking pituitary tumors, and causing pituitary dysfunction are relatively rare. Open surgery or endovascular treatment can treat these aneurysms, but achieving recovery of endocrine function is difficult.
Case Description:A 56-year-old man presented with giant aneurysm of the ICA causing pituitary impairment, leading to disturbance of consciousness due to hyponatremia. High-flow bypass from the cervical external carotid artery to the middle cerebral artery and ligation of the ICA at the cervical portion were performed. One year after the operation, his pituitary function recovered well; he was followed up as an outpatient without hormonal replacement therapy for 8 years after the operation.
Conclusion:Giant ICA aneurysm causing pituitary dysfunction is relatively rare, but it is important to consider in the differential diagnosis for hypopituitarism. Treatment with high-flow bypass using radial artery graft can achieve both prevention of aneurysm rupture and recovery of pituitary function.
Keywords: Giant aneurysm, high-flow bypass, internal carotid artery aneurysm, pituitary dysfunction
INTRODUCTION
Giant internal carotid artery (ICA) aneurysms extending into the sellar region, mimicking pituitary tumors, and causing pituitary dysfunction are rare but occasionally reported.[
CASE REPORT
A 56-year-old man with past medical history of dyslipidemia had been complaining of sleep disturbance, loss of motivation and appetite, and had lost 8 kg in weight in the last 6 months. He was diagnosed with depression and began treatment with antidepressant agents, sulpiride 150 mg and paroxetine 10 mg, at a local hospital. His symptoms deteriorated despite treatment, and he was admitted to a local mental hospital. Head computed tomography (CT) disclosed a mass suggestive of tumor near the sellar region and he was referred to our hospital [
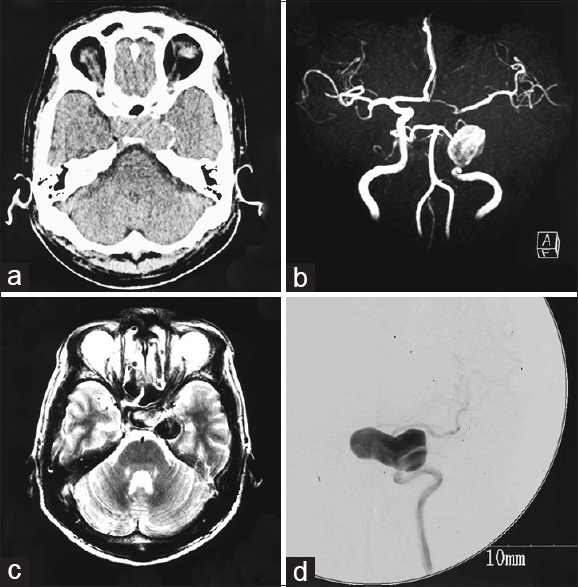
Figure 1
(a) Computed tomography scan showing a mass suggestive of tumor near the sellar region. (b) Magnetic resonance angiogram showing a large aneurysm of the left internal carotid artery (ICA). (c) T2-weighted magnetic resonance image revealing the aneurysm extending to the suprasellar region. (d) Cerebral digital subtraction angiogram of the left ICA revealing a giant aneurysm at the cavernous portion extending in the medial direction
On admission, he was drowsy and biochemistry revealed severe hyponatremia, with serum sodium level of 117 mEq/l. Treatment with intravenous saline and 200 mg hydrocortisone was started immediately. Magnetic resonance (MR) angiography demonstrated a large aneurysm of the left ICA, and T2-weighted MR imaging revealed the aneurysm extending to the suprasellar region [Figure
Several hormone load tests were conducted [
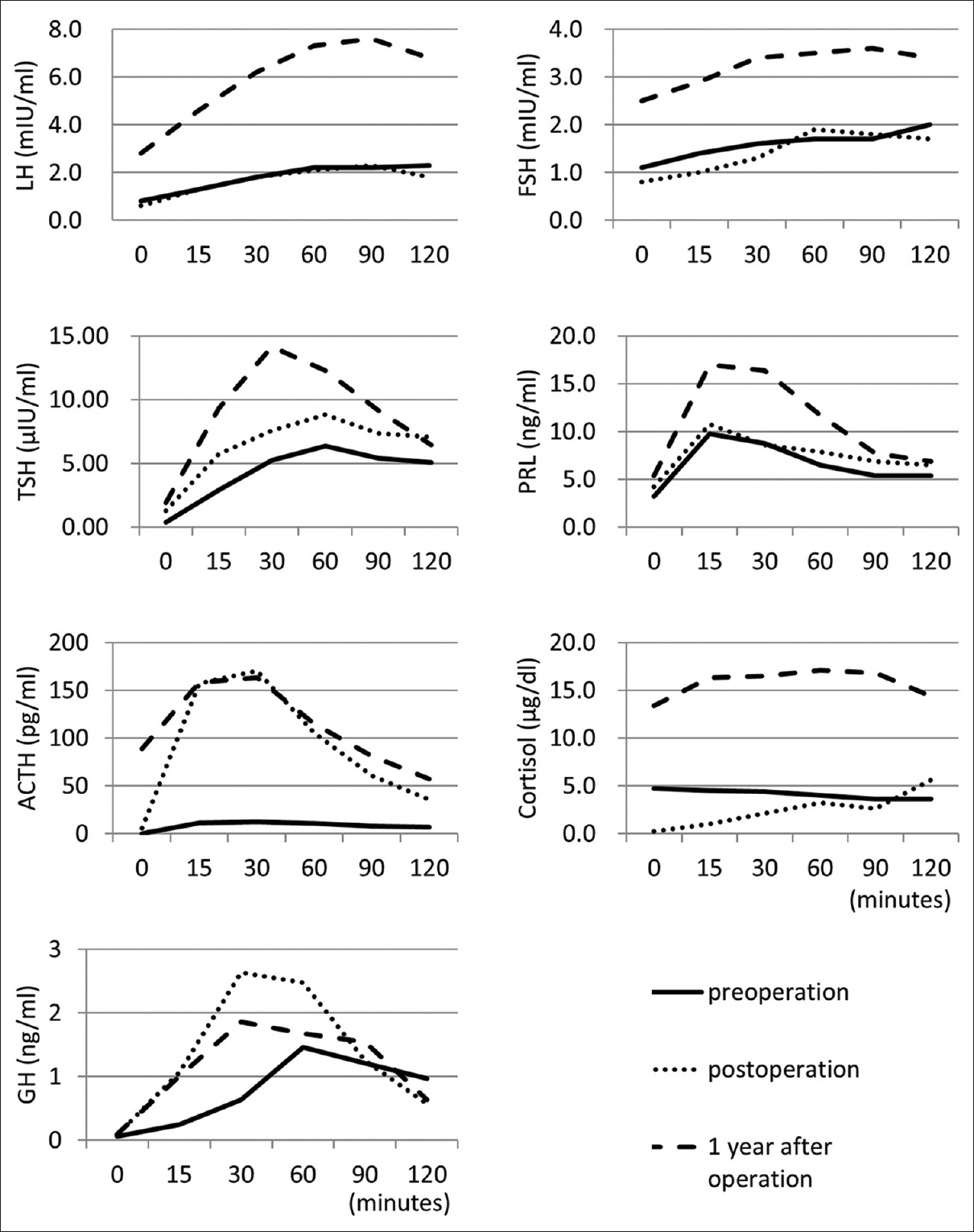
Figure 2
Time-series graphs of hormone load tests. Luteinizing hormone (LH)-releasing hormone load test: after intravenous injection of LH-releasing hormone (0.1 mg), LH and follicle-stimulating hormone (FSH) levels were examined. Thyrotropin-releasing hormone load test: after intravenous injection of thyrotropin-releasing hormone (0.5 mg), thyroid-stimulating hormone (TSH) and prolactin (PRL) levels were examined. Corticotropin-releasing hormone load test: after intravenous injection of corticotropin-releasing hormone (0.1 mg), adrenocorticotrophic hormone (ACTH) and cortisol levels were examined. Growth hormone (GH)-releasing factor load test: after intravenous injection of GH-releasing factor (0.1 mg), GH level was examined. Solid, dotted, and dashed lines indicate the data for preoperation, postoperation (3 weeks after operation), and 1 year after operation
Operation
Operation was conducted as described in our previous report.[
CT obtained on the day after the operation disclosed thrombosis of the aneurysm and cerebral angiography performed at 8 days after the operation demonstrated good patency of the bypasses and disappearance of flow to the aneurysm [Figure
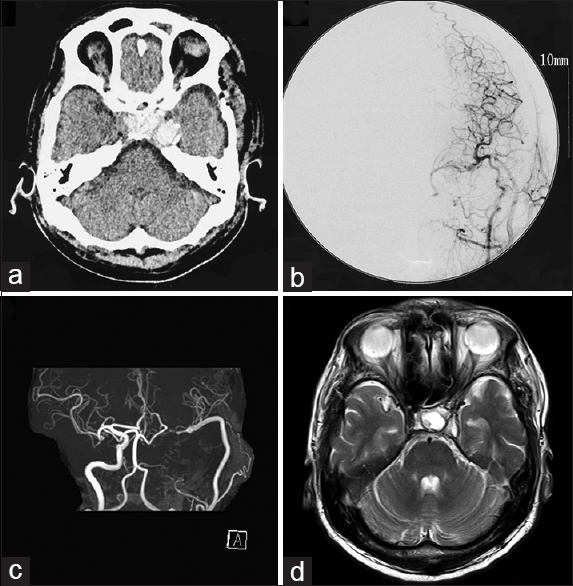
Figure 3
(a) Computed tomography scan on the day after the operation showing thrombosis of the aneurysm. (b) Cerebral angiogram performed at 8 days after the operation demonstrating good patency of the bypasses and disappearance of flow to the aneurysm. (c, d) Magnetic resonance angiogram (c) and image (d) obtained at 8 years after the operation showing good patency of the radial artery graft and shrinkage of the aneurysm
DISCUSSION
Pituitary dysfunction is estimated to have an annual incidence of 4.2 cases per 100,000, and a prevalence of 45.5 per 100,000.[
Endovascular coil embolization with or without stenting for giant aneurysms has unfortunately resulted in high recanalization and re-treatment rates.[
Direct and indirect open surgery methods are available for treating giant ICA aneurysms projecting into the sellar region.[
In this case, proximal ICA ligation was performed at the cervical portion with high-flow bypass using a RAG from the cervical ECA to the MCA, which achieved long-term prevention of aneurysm rupture without ischemic complication. Moreover, the aneurysm shrank and pituitary function recovered completely, making hormone replacement therapy unnecessary.
To assess the tolerance of ligating the ICA, balloon occlusion test (BOT) is commonly used. However, there is still no universal standard of this procedure, the accuracy of this test is complicated and controversial. Sometimes BOT causes complication such as cerebral infarction.[
Duration of pituitary impairment and extent of pituitary compression may also affect endocrine recovery after treatment.[
Giant ICA aneurysm causing pituitary dysfunction is rare and not well characterized, but is important to consider in the differential diagnosis for hypopituitarism. Treatment with high-flow bypass using RAG is effective for achieving both prevention of aneurysm rupture and recovery of pituitary function.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Barnett DW, Barrow DL, Joseph GJ. Combined extracranial-intracranial bypass and intraoperative balloon occlusion for the treatment of intracavernous and proximal carotid artery aneurysms. Neurosurgery. 1994. 35: 92-7
2. Becske T, Kallmes DF, Saatci I, McDougall CG, Szikora I, Lanzino G. Pipeline for uncoilable or failed aneurysms: Results from a multicenter clinical trial. Radiology. 2013. 267: 858-68
3. Becske T, Potts MB, Shapiro M, Kallmes DF, Brinjikji W, Saatci I. Pipeline for uncoilable or failed aneurysms: 3-year follow-up results. J Neurosurg. 2016. p.
4. Cao C, Ang SC, Wolak K, Peeceeyen S, Bannon P, Yan TD. A meta-analysis of randomized controlled trials on mid-term angiographic outcomes for radial artery versus saphenous vein in coronary artery bypass graft surgery. Ann Cardiothorac Surg. 2013. 2: 401-7
5. Ding D, Mehta GU, Liu KC. Pituitary insufficiency from large unruptured supraclinoid internal carotid artery aneurysm. Br J Neurosurg. 2014. 28: 290-2
6. Drake CG, Peerless SJ, Ferguson GG. Hunterian proximal arterial occlusion for giant aneurysms of the carotid circulation. J Neurosurg. 1994. 81: 656-65
7. Fernandez-Real JM, Fernandez-Castaner M, Villabona C, Sagarra E, Gomez-Saez JM, Soler J. Giant intrasellar aneurysm presenting with panhypopituitarism and subarachnoid hemorrhage: Case report and literature review. Clin Investig. 1994. 72: 302-6
8. Field M, Jungreis CA, Chengelis N, Kromer H, Kirby L, Yonas H. Symptomatic cavernous sinus aneurysms: Management and outcome after carotid occlusion and selective cerebral revascularization. AJNR Am J Neuroradiol. 2003. 24: 1200-7
9. Gelber BR, Sundt TM. Treatment of intracavernous and giant carotid aneurysms by combined internal carotid ligation and extra- to intracranial bypass. J Neurosurg. 1980. 52: 1-10
10. Giustina A, Scalvini T, Cerudelli B, Bossoni S, Bodini C, Orlandini A. Hypopituitarism secondary to suprasellar giant carotido-ophthalmic aneurysm. Normalization of the hypophyseal function after neurosurgical depression of the aneurysm. Minerva Endocrinol. 1989. 14: 255-8
11. Gungor A, Gokkaya N, Bilen A, Bilen H, Akbas EM, Karadeniz Y. Pituitary insufficiency and hyperprolactinemia associated with giant intra- and suprasellar carotid artery aneurysm. Case Rep Med 2015. 2015. p.
12. Hall J, Caputo C, Chung C, Holt M, Wang YY. Delayed pan-hypopituitarism as a complication following endovascular treatment of bilateral internal carotid artery aneurysms. A case report and review. Br J Neurosurg. 2015. 29: 303-5
13. Heshmati HM, Fatourechi V, Dagam SA, Piepgras DG. Hypopituitarism caused by intrasellar aneurysms. Mayo Clin Proc. 2001. 76: 789-93
14. Houkin K, Kamiyama H, Kuroda S, Ishikawa T, Takahashi A, Abe H. Long-term patency of radial artery graft bypass for reconstruction of the internal carotid artery. Technical note. J Neurosurg. 1999. 90: 786-90
15. Ishishita Y, Tanikawa R, Noda K, Kubota H, Izumi N, Katsuno M. Universal extracranial-intracranial graft bypass for large or giant internal carotid aneurysms: Techniques and results in 38 consecutive patients. World Neurosurg. 2014. 82: 130-9
16. Kayath MJ, Lengyel AM, Nogueira R, Tella Junior O, Czepielewski MA. Giant aneurysms of the sellar region simulating pituitary adenomas: A diagnosis to be considered. J Endocrinol Invest. 1991. 14: 975-9
17. Lawson EA, Buchbinder BR, Daniels GH. Hypopituitarism associated with a giant aneurysm of the internal carotid artery. J Clin Endocrinol Metab. 2008. 93: 4616-
18. Molyneux AJ, Kerr RS, Yu LM, Clarke M, Sneade M, Yarnold JA. International Subarachnoid Aneurysm Trial (ISAT) Collaborative Group. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: A randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet. 2005. 366: 809-17
19. Ono H, Inoue T, Suematsu S, Tanishima T, Tamura A, Saito I. Middle cerebral artery dissection causing subarachnoid hemorrhage and cerebral infarction: Trapping with high-flow bypass preserving the lenticulostriate artery. Surg Neurol Int Forthcoming. 2017. p.
20. Patel HC, Teo M, Higgins N, Kirkpatrick PJ. High flow extra-cranial to intra-cranial bypass for complex internal carotid aneurysms. Br J Neurosurg. 2010. 24: 173-8
21. Ramanathan D, Temkin N, Kim LJ, Ghodke B, Sekhar LN. Cerebral bypasses for complex aneurysms and tumors: Long-term results and graft management strategies. Neurosurgery. 2012. 70: 1442-57
22. Raymond J, Guilbert F, Weill A, Georganos SA, Juravsky L, Lambert A. Long-term angiographic recurrences after selective endovascular treatment of aneurysms with detachable coils. Stroke. 2003. 34: 1398-403
23. Raymond LA, Tew J. Large suprasellar aneurysms imitating pituitary tumour. J Neurol Neurosurg Psychiatry. 1978. 41: 83-7
24. Schneider HJ, Aimaretti G, Kreitschmann-Andermahr I, Stalla GK, Ghigo E. Hypopituitarism. Lancet. 2007. 369: 1461-70
25. Seok H, Park HN, Kim GH, Son HS, Sohn TS. A giant carotid aneurysm with intrasellar extension: A rare cause of panhypopituitarism. Korean J Intern Med. 2015. 30: 265-6
26. Tan LA, Sandler V, Todorova-Koteva K, Levine L, Lopes DK, Moftakhar R. Recovery of pituitary function following treatment of an unruptured giant cavernous carotid aneurysm using Surpass flow-diverting stents. BMJ Case Rep 2014. 2014. p.
27. Tungaria A, Kumar V, Garg P, Jaiswal AK, Behari S. Giant, thrombosed, sellar-suprasellar internal carotid artery aneurysm with persistent, primitive trigeminal artery causing hypopituitarism. Acta Neurochir (Wien). 2011. 153: 1129-33
28. Verbalis JG, Nelson PB, Robinson AG. Reversible panhypopituitarism caused by a suprasellar aneurysm: The contribution of mass effect to pituitary dysfunction. Neurosurgery. 1982. 10: 604-11

