

- Department of Neurosurgery, Post Graduate Institute of Medical Education and Research, Chandigarh, India
- Department of Histopathology, Post Graduate Institute of Medical Education and Research, Chandigarh, India
Correspondence Address:
Sandeep Mohindra
Department of Histopathology, Post Graduate Institute of Medical Education and Research, Chandigarh, India
DOI:10.4103/2152-7806.183544
Copyright: © 2016 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Mohindra S, Kapoor A, Mitra S, Nahar U. Giant primary calvarial hemangioma over torcula: Radiological features and operative nuances. Surg Neurol Int 03-Jun-2016;7:
How to cite this URL: Mohindra S, Kapoor A, Mitra S, Nahar U. Giant primary calvarial hemangioma over torcula: Radiological features and operative nuances. Surg Neurol Int 03-Jun-2016;7:. Available from: http://surgicalneurologyint.com/surgicalint_articles/giant-primary-calvarial-hemangioma-over-torcula-radiological-features-and-operative-nuances/
Abstract
Background:Although rare, primary calvarial hemangioma is a known entity, surgical excision of which usually results in massive blood loss. Successful total excision of such a lesion remains a challenge, especially when these are in close vicinity of major venous sinuses.
Case Description:Authors describe a rare case of intra-osseous occipital cavernoma along with radiological findings in a 50-year-old male. En bloc resection of tumor was performed using a high-speed pneumatic drill and no recurrence was noted at 6 months of follow-up.
Conclusion:Intra-osseous cavernous hemangiomas have classical radiological features and can be excised completely, even when lying above major venous drainage channels like torcula.
Keywords: Intra-osseous cavernous hemangioma, radiology, total excision
INTRODUCTION
Primary intra-osseous cavernous hemangiomas (PICHs) account for only 0.2% of all bone neoplasms.[
CASE REPORT
A 50-year-old male presented with history of huge swelling at the midline of the back of the head, progressively increasing in size over the past decade. The patient had no other complaints except for the cosmetic deformity due to swelling. On examination, the lesion was 10 cm in diameter, centering at external occipital protuberance. The swelling was firm to hard in consistency, nontender and immobile. Overlying skin was shiny with visible dilated vessels and was freely mobile. There was no bruit heard over the swelling. Neurological examination was unremarkable. Fundoscopy revealed no papilledema. Computed tomography (CT) scan showed an intra-diploic tumor expanding both inner and outer tables, centered over torcula, with a characteristic sunburst pattern with striations radiating from the center. The underlying brain was normal. Magnetic resonance imaging (MRI) scans showed an extra-axial lesion which was iso-intense on T1-weighted imaging (T1WI) and hyper-intense on T2-weighted imaging (T2WI), enhancing brilliantly on contrast administration [Figures
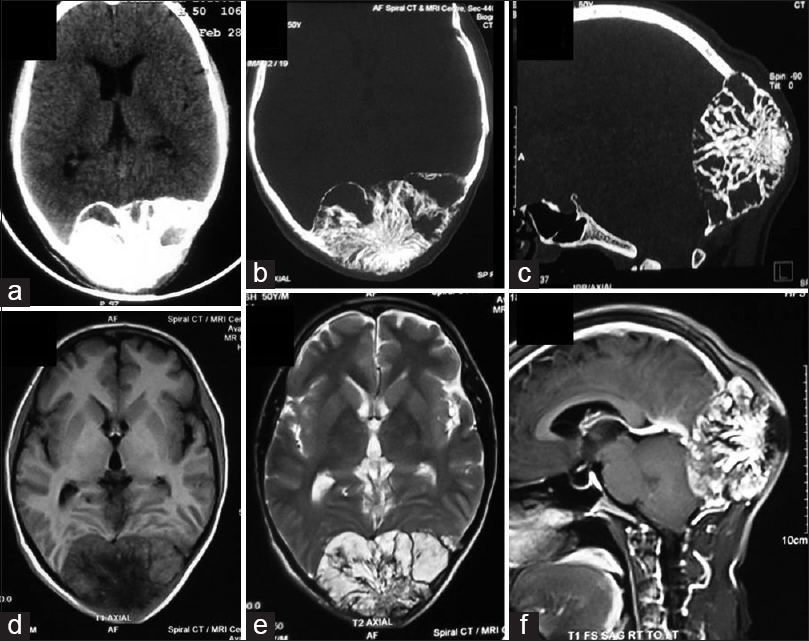
Figure 1
Axial section of computed tomography scan (a) showing an intra-osseous bony neoplasm. Bone window of axial section (b) and sagittal section (c) showing classical sunburst pattern of bony tumor. Expansion and thinning of inner and outer table is obvious. Axial section of magnetic resonance imaging scan showing hypo-intense signal indicating loss of fat on T1-weighted imaging (d) and hyper-intense signal on T2-weighted imaging (e). Sagittal section of contrast-enhanced magnetic resonance imaging scan (f) showing intra-osseous tumor over torcula
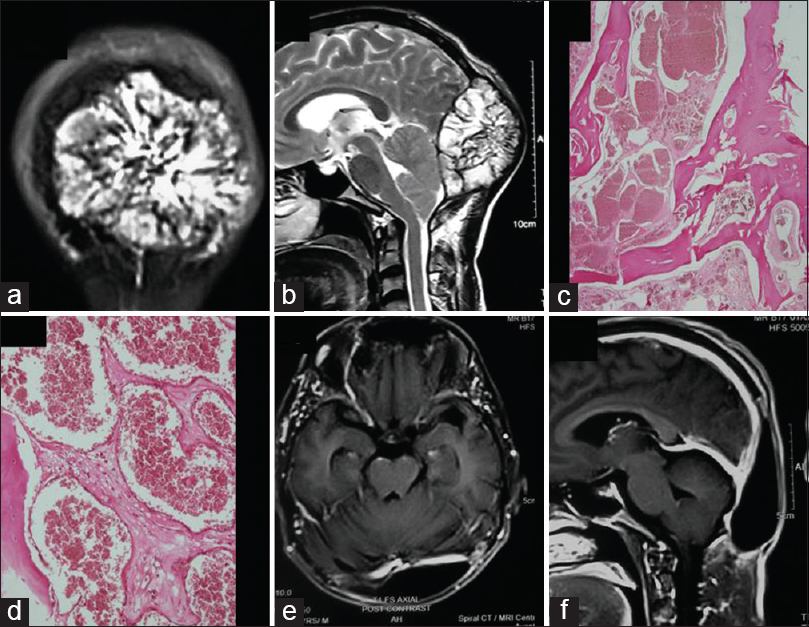
Figure 2
Coronal section of contrast-enhanced magnetic resonance imaging scan (a), sagittal section of T2-weighted imaging scan (b) showing intact inner table and no intradural invasion of tumor. Microphotograph (c) showing cystically dilated blood vessels in the inter-trabecular marrow spaces (H and E, ×40). Higher magnification (d) depicting single layer of endothelial lining (H and E, ×400). Follow-up contrast-enhanced axial (e) and coronal section (f) magnetic resonance imaging scans showing total excision of cavernous hemangioma
With a presumptive diagnosis of intra-osseous cavernous hemangioma, meningioma or metastases, patient underwent surgery in prone position. Whole of the bony mass lesion was exposed by linear skin incision and both outer/inner tables were noted to be thin and papery. After delineating the normal calvarial bone all around the tumor, four burr holes were made over there, encircling the bony tumor using cutting burr of the high-speed pneumatic drill. Further, all four burr holes were connected using high-speed pneumatic craniotome and en bloc tumor was gradually lifted up after peeling of dura from the inner table with a penfield dissector. Multiple venous drainage communications were sealed using gelfoam and there was no injury to major venous sinuses. Estimated blood loss was 750 ml and all cut surfaces of vault were sealed with bone wax to avoid inadvertent air embolism. Tumor, with a rim of normal bone, was excised completely and sent for histopathology which showed large thin-walled vascular channels with small thin walled and angulated capillary sized blood filled vessels, suggestive of a cavernous hemangioma of occipital bone [Figure
DISCUSSION
PICHs are rare, benign, slow-growing skeletal neoplasms and more than half of cases occur in vertebrae or skull.[
Devoid of reactive sclerosis at the margins, these lesions may present as lytic or dense bone expanding masses.[
The literature describes only two cases where such a neoplasm was described just in proximity to torcula.[
CONCLUSION
Calvarial cavernous hemangiomas are benign neoplasms, which are occasionally located in close proximity to venous sinuses. These neoplasms have classical radiological features and if carefully noted, these imaging findings can guide for the bold surgical strategy of total cavernoma excision, even when these lesions are lying above great venous channels of dura.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Banerji D, Inao S, Sugita K, Kaur A, Chhabra DK. Primary intraosseous orbital hemangioma: A case report and review of the literature. Neurosurgery. 1994. 35: 1131-4
2. Martínez-Lage JF, Torroba MA, Cuartero Pérez B, Almagro MJ, López López-Guerrero A, de la Rosa P. Cavernous hemangiomas of the cranial vault in infants: A case-based update. Childs Nerv Syst. 2010. 26: 861-5
3. Muzumdar D, Goel A, Desai K, Bhayani R, Sharma P. Primary hemangioma of the occipital bone in the region of the torcula - Two case reports. Neurol Med Chir (Tokyo). 2002. 42: 27-30
4. Nair P, Srivastava AK, Kumar R, Jain K, Sahu RN, Vij M. Giant primary intraosseous calvarial hemangioma of the occipital bone. Neurol India. 2011. 59: 775-6
5. Nasrallah IM, Hayek R, Duhaime AC, Stotland MA, Mamourian AC. Cavernous hemangioma of the skull: Surgical treatment without craniectomy. J Neurosurg Pediatr. 2009. 4: 575-9
6. Patnaik A, Mishra SS, Mishra S, Deo RC. Intradiploic ossified giant cavernous hemangioma of skull with a dural tail sign mimicking primary calvarial meningioma. Neurol India. 2012. 60: 250-2
7. Peterson DL, Murk SE, Story JL. Multifocal cavernous hemangioma of the skull: Report of a case and review of the literature. Neurosurgery. 1992. 30: 778-81
8. Suzuki Y, Ikeda H, Matsumoto K. Neuroradiological features of intraosseous cavernous hemangioma - Case report. Neurol Med Chir (Tokyo). 2001. 41: 279-82
9. Toynbee J. An account of two vascular tumours developed in the substance of bone. Lancet. 1845. 2: 676-
10. Tyagi DK, Balasubramaniam S, Sawant HV. Giant primary ossified cavernous hemangioma of the skull in an adult: A rare calvarial tumor. J Neurosci Rural Pract. 2011. 2: 174-7
11. Verma SK, Singh PK, Garg K, Satyarthee GD, Sharma MC, Singh M. Giant calvarial cavernous hemangioma. J Pediatr Neurosci. 2015. 10: 41-4
12. Wyke BD. Primary hemangioma of the skull; a rare cranial tumor; review of the literature and report of a case, with special reference to the roentgenographic appearances. Am J Roentgenol Radium Ther. 1949. 61: 302-16

