

- Department of Neurosurgery, Gunma University, Maebashi, Japan.
Correspondence Address:
Shunsuke Nakamura, Department of Neurosurgery, Gunma University, Maebashi, Japan.
DOI:10.25259/SNI_432_2023
Copyright: © 2023 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Shunsuke Nakamura, Tatsuya Shimizu, Haruka Tsuneoka, Takaaki Miyagishima, Yuhei Yoshimoto. Glossopharyngeal neuralgia with repeated cardiac syncope: A case report. 16-Jun-2023;14:208
How to cite this URL: Shunsuke Nakamura, Tatsuya Shimizu, Haruka Tsuneoka, Takaaki Miyagishima, Yuhei Yoshimoto. Glossopharyngeal neuralgia with repeated cardiac syncope: A case report. 16-Jun-2023;14:208. Available from: https://surgicalneurologyint.com/surgicalint-articles/12364/
Date of Submission
19-May-2023
Date of Acceptance
01-Jun-2023
Date of Web Publication
16-Jun-2023
Abstract
Background: Glossopharyngeal neuralgia (GPN) is an uncommon craniofacial pain syndrome. Although rare, it is occasionally associated with cardiac syncope, as vago-glossopharyngeal neuralgia (VGPN).
Case Description: We present the case of a 73-year-old man with VGPN misdiagnosed as trigeminal neuralgia. The patient was diagnosed with sick sinus syndrome, and a pacemaker was introduced. However, syncope still recurred. Magnetic resonance imaging revealed a branch of the right posterior inferior cerebellar artery contacting the root exit zone of the right glossopharyngeal and vagus nerves. We diagnosed VGPN due to neurovascular compression and performed microvascular decompression (MVD). The symptoms disappeared postoperatively.
Conclusion: Diagnosis of VGPN needs appropriate medical interviews and physical examination. MVD is the only curative treatment for VGPN occurring as a neurovascular compression syndrome.
Keywords: Case report, Glossopharyngeal neuralgia, Microvascular decompression, Syncope, Vagoglossopharyngeal neuralgia
INTRODUCTION
Glossopharyngeal neuralgia (GPN) is an uncommon craniofacial pain syndrome characterized by paroxysms of severe stabbing pain unilaterally in the pharynx and ears. Although rare, it is sometimes associated with cardiac syncope and is termed “vago-glossopharyngeal neuralgia” (VGPN). We present a case of GPN with cardiac syncope that was successfully treated by microvascular decompression (MVD).
CASE REPORT
A 73-year-old man presented with an 11-year history of paroxysmal stabbing facial pain. The pain occurred repeatedly and was sometimes associated with loss of consciousness after the pain attack. The patient was referred to a cardiologist for evaluation of the syncope and was diagnosed with sick sinus syndrome. A pacemaker was introduced, although syncope still recurred.
Five years after the first pain episode, the pain progressively worsened. The patient was diagnosed with the right trigeminal neuralgia at a pain clinic and was treated with carbamazepine and nerve block injection. However, the effect of the treatment was limited, with recurrence of the attacks of pain and loss of consciousness. Although magnetic resonance imaging (MRI) was considered, the pacemaker introduced in the patient precluded performance of MRI. However, after his pacemaker was replaced with an MRI-compatible one during the current year, he was referred to our department for further evaluation and treatment of the facial pain.
The patient’s physical/neurological examination revealed no abnormal findings. The pain was located at the right side of the pharynx and the root of the tongue, with radiation to the ipsilateral cheek and ear. It was triggered by swallowing and gargling, with the pain being provoked when food touched his right soft palate while swallowing. The pain was intolerable and lasted for 2–3 min. Chewing or physical stimulation of the face did not cause pain. The patient sometimes lost consciousness after the pain.
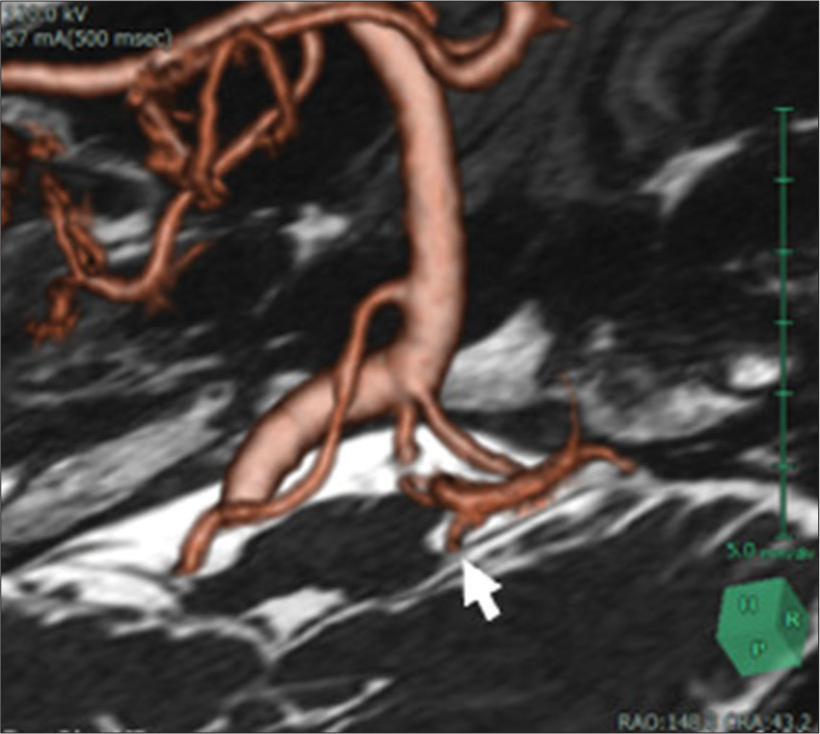
MRI revealed a looped branch of the right posterior inferior cerebellar artery (PICA) contacting the root exit zone (REZ) of the right glossopharyngeal and vagus nerves [
A small 4 cm craniotomy was performed on the right occipital bone with the patient in the park bench position. The looped branch of the PICA was confirmed as compressing the REZ of the glossopharyngeal and vagus nerves from the ventral side [
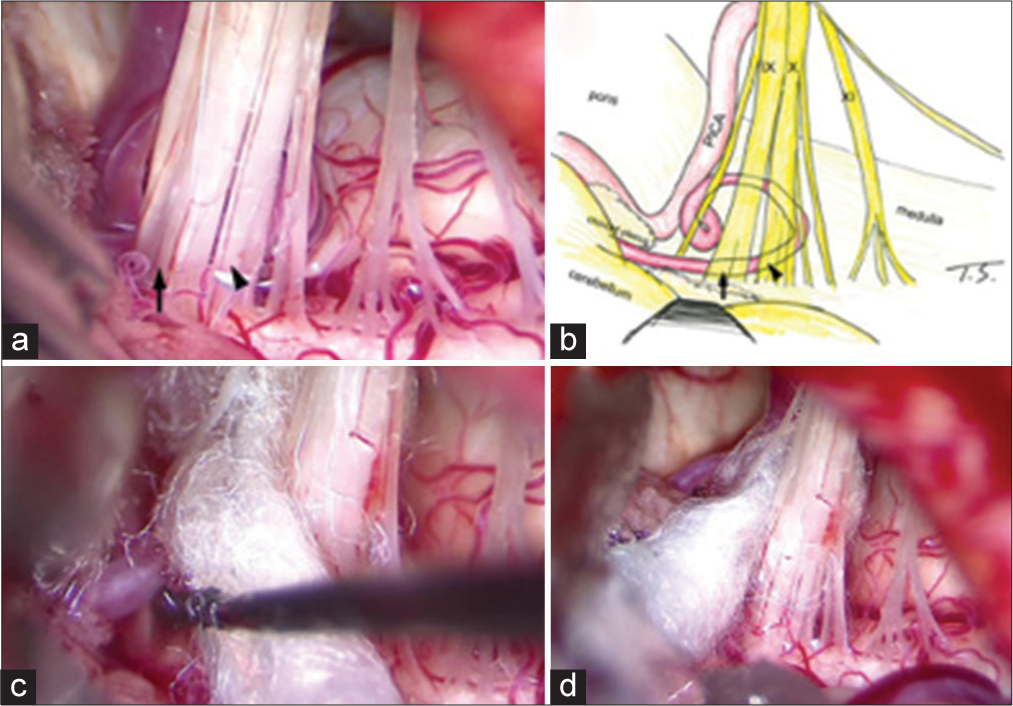
Figure 2:
Intraoperative view and schema. (a and b) A branch of the right posterior inferior cerebellar artery (PICA) formed a loop, contacting anteriorly with the root exit zone of the glossopharyngeal (IX, arrow), vagus nerves (X, arrowhead). XI: accessory nerve. (c) The PICA was transposed with Teflon felts and fixed with fibrin glue. (d) Final view.
DISCUSSION
GPN is a rare disease that accounts for 0.2–1.3% of facial pain. The pain begins unilaterally from the root of the tongue and pharynx and radiates to the tympanic membrane, external auditory canal, and auricular region. These locations of pain differ from trigeminal neuralgia.[
VGPN accounts for 2% of GPN cases and is a very rare condition.[
In any case, the stimulated vagus nerve activates the vagus nerve-carotid baroreceptor pathway, resulting in marked bradycardia (cardioinhibitory effect) and reduction in peripheral vascular resistance (vasodilatory effect), which ultimately provoke syncope.[
In addition, carbamazepine, which is used in the medical treatment of neuralgia, produces side effects such as bradyarrhythmia and atrioventricular block.[
CONCLUSION
MVD is considered to be the only curative treatment for VGPN. Although diagnosis of VGPN is not always easy, early diagnosis by appropriate medical interviews and physical examination is important.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Can I, Tholakanahalli V. Carbamazepine-induced atrioventricular block in an elderly woman. Turk Kardiyol Dern Ars. 2015. 44: 68-70
2. Hie CH, Arnold AE, Ruiter JH. Glossopharyngeal neuralgia with syncope: A case report. Neth Heart J. 2002. 10: 150-3
3. Krasoudakis A, Anyfantakis D, Hadjipetrou A, Kastanakis M, Symvoulakis EK, Marathianos S. Glossopharyngeal neuralgia associated with cardiac syncope: Two case reports and literature review. Int J Surg Case Rep. 2015. 12: 4-6
4. Ozenci M, Karaoguz R, Conkbayir C, Altin T, Kanpolat Y. Glossopharyngeal neuralgia with cardiac syncope treated by glossopharyngeal rhizotomy and microvascular decompression. Europace. 2003. 5: 149-52
5. Savica R, Lagana A, Calabro RS, Casella C, Musolino R. Vagoglossopharyngeal neuralgia: A rare case of sincope responding to pregabalin. Cephalalgia. 2007. 27: 566-7
6. Wallin BG, Westerberg CE, Sundlof G. Syncope induced by glossopharyngeal neuralgia: Sympathetic outflow to muscle. Neurology. 1984. 34: 522-4
7. Xia L, Li YS, Liu MX, Zhong J, Dou NN, Li B. Microvascular decompression for glossopharyngeal neuralgia: A retrospective analysis of 228 cases. Acta Neurochir (Wien). 2018. 160: 117-23

