

- Department of Neurosurgery, Allegheny General Hospital, Pittsburgh, Pennsylvania, USA
- Department of Neurosurgery, Lariboisière Hospital, Assistance Publique – Hôpitaux de Paris, University of Paris VII-Diderot, Paris, France
Correspondence Address:
Khaled M. Aziz
Department of Neurosurgery, Allegheny General Hospital, Pittsburgh, Pennsylvania, USA
DOI:10.4103/sni.sni_29_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Nouman Aldahak, Derrick Dupre, Mohamed Ragaee, Sebastien Froelich, Jack Wilberger, Khaled M. Aziz. Hydroxyapatite bone cement application for the reconstruction of retrosigmoid craniectomy in the treatment of cranial nerves disorders. 13-Jun-2017;8:115
How to cite this URL: Nouman Aldahak, Derrick Dupre, Mohamed Ragaee, Sebastien Froelich, Jack Wilberger, Khaled M. Aziz. Hydroxyapatite bone cement application for the reconstruction of retrosigmoid craniectomy in the treatment of cranial nerves disorders. 13-Jun-2017;8:115. Available from: http://surgicalneurologyint.com/surgicalint-articles/hydroxyapatite-bone-cement-application-for-the-reconstruction-of-retrosigmoid-craniectomy-in-the-treatment-of-cranial-nerves-disorders/
Date of Submission
21-Jan-2017
Date of Acceptance
07-Apr-2017
Date of Web Publication
13-Jun-2017
Abstract
Background:Retromastoid craniectomy (RSC) is a cardinal surgical approach used to access the posterior fossa. Hydroxyapetite bone cement (HBC) is frequently employed for cranioplasty in efforts to prevent cerebrospinal fluid (CSF) leak, whilst maintaining low complication rates and good cosmetic satisfaction. The authors aim to determine the safety and effectiveness of HBC for reconstruction RSC used for treatment of various cranial nerves disorders.
Methods:The authors conducted a retrospective one-center two surgeons review of 113 patients who underwent RSC filled with HBC for the treatment of cranial nerve disorders. The study period extended from January 2011 through April 2016. Charts were reviewed for documentation of descriptors pertinent to the endpoints described above. Revisions and reoperations were excluded from analysis.
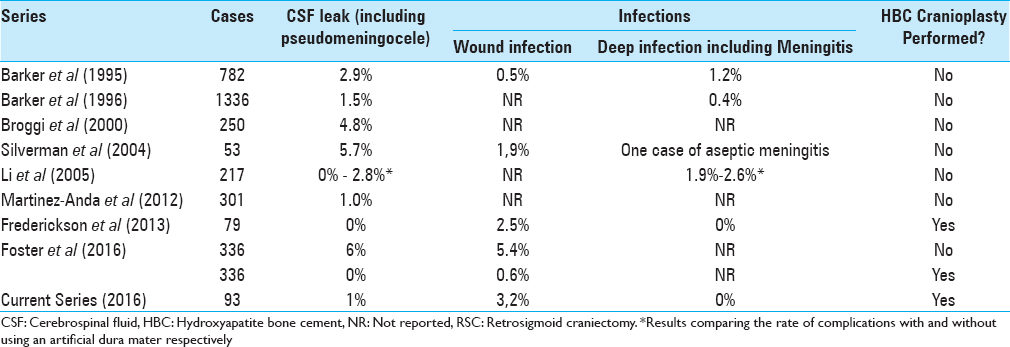
Results:Ninety-three patients met the inclusion criteria; there was one case of postoperative pseudomeningocele, which was considered as CSF leak (1%), 3 (3,2%) superficial infections, and no deep infections. Cosmetic satisfaction was obtained in all but one case (98.9% satisfaction) and long-term incisional pain was problematic in 1 (1.1%) patient. Other complications (serous drainage, headache, ear pain) accounted for three cases (3.2%).
Conclusions:The application of HBC in the reconstruction of RSC for the treatment of cranial nerves disorders is an effective method, yielding good cosmetic results whilst eliminating CSF leak. Additionally, it is safe due to the lack of deep-seated wound infections with low incidence of chronic incisional pain.
Keywords: Calcium phosphate, cerebrospinal fluid leak, hydroxyapatite, microvascular decompression, retrosigmoid craniotomy
INTRODUCTION
Hydroxyapatite bone cement (HBC) is frequently employed in the treatment of cranial bony defects. It has been championed as a viable option for cranial defect reconstruction when cosmetics and fluid hydrostatics are considered. Infratentorial craniotomies or craniectomies have higher rates of cerebrospinal fluid (CSF) leakage than supratentorial defects due to their gravity-dependent nature, lending desire for safe reconstructive options capable of restoring the natural barrier provided by the skull.
HBC is known to have osteoconductive properties, providing for more physiologic restoration of cranial defects.[
Retrosigmoid craniecotomy (RSC) is used to access a wide variety of neurosurgical posterior fossa pathologies and cranial nerves disorders.[
The safety of HBC in cranial surgery has been challenged in recent years, lending reservation to many surgeons. Delayed inflammatory reactions have been suspect in cases where thinning of the skin and breakdown resulted after HBC cranioplasty.[
Previous publications have reported on complication rates associated with HBC for a wide variety of craniotomy types; however, there is currently a paucity of studies demonstrating the results specific to RSC for the treatment of cranial nerve pathologies. The authors aim to determine the effects and complication profile of HBC in this specific setting.
MATERIALS AND METHODS
An institutional review board (IRB) review and approval was obtained to initiate this study. The authors conducted a retrospective analysis of one hundred thirteen cases of retrosigmoid craniotomies performed for microvascular decompression (MVD) in the treatment of various cranial nerves disorders and vestibular nerve sections. The cases were pooled from a prospectively maintained database. Any patient who had a prior surgery at the site of interest was excluded from analysis. Only patients who were operated on by one of the two surgeons (KA and JW) at a single institution (Allegheny General Hospital, Pittsburgh, PA 15212) were included in analysis.
Cosmetic satisfaction was graded as all or none upon follow-up by posing a simple question to the patient at the follow up visit: “Are you satisfied with the cosmetic results of your procedure?” Long-term incisional pain was defined as pain and/or tenderness at the incision requiring pain medication and/or clinical evaluation 3 months (or longer) postoperatively. All other postoperative events were recorded including: superficial or deep infection, CSF leak, headache, ear pain, and serous drainage. RSC (one-inch diameter) was carried out in a standard manner, as previously described.[
RESULTS
Over the 63 months’ study period, 113 patients underwent RSC for MVD or section of cranial nerves. Ninety-three patients met inclusion criteria and were therefore included in analysis. Of those excluded from the series, 8 were revisions, while the rest did not carry adequate documentation and/or follow-up to be included in analysis. Mean age was 51 years (range 31 to 83 years), and there were 52 females and 41 males who underwent RSC for various disorders, including trigeminal neuralgia (TGN, N = 78), glossopharyngeal neuralgia (GPN, N = 1), Ménière's Disease (N = 7), and hemifacial spasm (HFS, N = 7) as a primary diagnosis. Of the 93 patients in the cohort, three carried a diagnosis including more than one of those listed above. Mean follow-up was 9.7 months (range 3 to 39 months). HBC cranioplasty without additional materials was accomplished in all cases.
While there were no deep-seated postoperative infections, three patients developed superficial wound complications requiring revision [
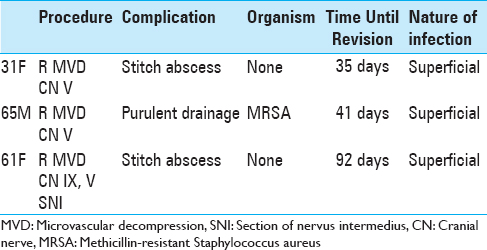
CSF external leak from the wound did not occur in any cases, however, one patient presented a pseudomeningocele 15 days post operatively and underwent a surgical revision after an external lumbar drainage failure; the HBC was changed to a titanium mesh cranioplasty.
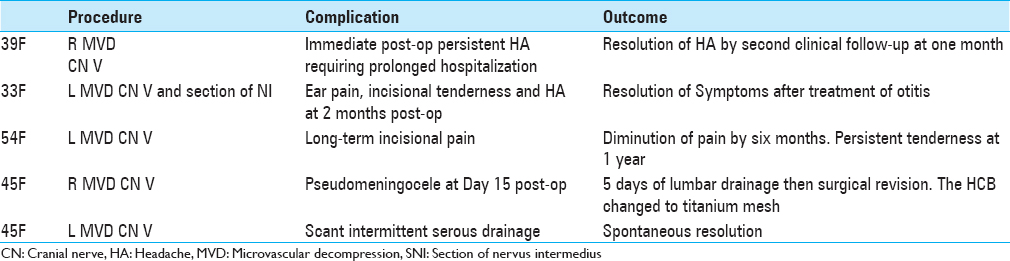
Long-term incisional pain occurred in one case where prescription pain medication was continually requested by the patient. The pain subsided to a low-intensity tenderness at the operative site at 6 months but remained present at one year. At no point was there concern for infection due to the lack of clinical evidence of such, including erythema, dehiscence, drainage or systemic signs of infection. A different patient had persistent pain associated with a headache and earache of gradual onset at two months. Further work-up and neuro-otological evaluation revealed otitis externa, which was treated with antibiotics, resulting in resolution of the headaches, earaches, and incisional tenderness. One patient was hospitalized for 6 days postoperatively due to uncontrollable headaches, which gradually tapered off by the time of clinical follow up. In one case, small amounts of straw-colored fluid drained from the incision was observed; no clinical or biological sign of infection was found, the “leakage” had resolved gradually under a conservative management and observation.
One patient was dissatisfied with the cosmetic results due to the scar, which formed after revision for stitch abscess. There were no complaints of palpable or visible deformities beneath the skin. All other patients stated complete satisfaction with the cosmetic results including the three other patients who underwent revision for superficial wound infection.
DISCUSSION
The HBC cranioplasty used in reconstruction of RSC seems to be a safe method to eliminate the CSF leak and deep wound infections’ it yields a good cosmetic dissatisfaction as well. Our results reaffirm the safety of HBC and its efficacy in providing a water-tight barrier.
Technical nuances employed in the application of HBC likely contribute to the low rate of patient dissatisfaction. Smoothing of the HBC to the contours of the skull with the lowest possible profile without allowing for the uncured cement to sink into the craniectomy is paramount, as HBC cranioplasty may lead to palpable depressions.[
In our series, scar formation was the source of the one instance where cosmetic satisfaction was not attained; therefore, the authors consider this unrelated to the cement cranioplasty but rather attributable to soft tissue wound healing.
Other complications included persistent postoperative incisional pain (N = 1), diffuse headache (N = 1), scant serous wound drainage (N = 1), otitis externa (N = 1), and pseudomeningocel (N = 1).
Persistent postoperative incisional pain has been attributed to damage or irritation of the lesser occipital and/or greater auricular nerves through contact with the underlying cranioplasty.[
Headaches frequently occur after craniotomy due to loss of CSF, therefore, measures aimed at the reduction of CSF loss should be employed. The authors propose that the low incidence of uncontrollable postoperative headaches is partly attributable to the very low incidence of postoperative CSF leakage in the series at hand, as well as to the copious saline irrigation used intraoperatively. Continuous intraoperative irrigation functions not only to replace the lost volume of CSF, but also to wash out any irritants, which may contribute to chemical meningitis, such as bone dust, blood products, or other foreign materials introduced into the arachnoid space.[
In the one case, where small amounts of straw-colored fluid drained from the incision, there were no signs of infection. The patient's temperature and white blood cell count were within normal limits, and there was no surrounding erythema or wound dehiscence. In fact, the drainage was not reproducible at the clinic visit. The authors instructed the patient to place a sterile gauze strip on the wound when and if the drainage reoccurred. The following night the patient presented to the emergency department with a small (1.5 cm) moist spot on the dressing, although the “leakage” had spontaneously resolved. There have been reports of HBC resorption leading to seroma formation after RSC,[
The episode of otitis externa, which occurred in one patient postoperatively, is believed to be unrelated to the HBC, as there were no physical signs of wound healing problems at the incision. Additionally, the patient previously suffered from similar bouts of otitis externa, yet presented to the emergency department out of concern due to the recent surgery.
One patient presented at day 15 postoperatively due to a collection at the operation site without external leakage. The clinical, radiological, and biological investigations revealed a pseudomeningocele without infection signs. An external lumbar drainage was applied for 5 days. Unfortunately; the drain weaning failed, so the patient underwent a surgical local revision and the HBC was changed to a titanium mesh cranioplasty.
Limitations of the current study derive primarily from the retrospective nature of the investigation. Additionally, many patients included in the study reside a considerable distance from the authors’ quaternary referral center, making travel cumbersome. Therefore, telephone interviews accounted for a sizeable proportion of follow-up, making visual inspection impossible. Lastly, the binary nature of the question posed to all patients at follow up (“Are you satisfied with the cosmetic results of your procedure?”) does not allow for in-depth analysis of those responses. While the number of patients included in the current study is sizeable, it is not as robust of a comparison amongst populations undergoing RSC as would be a study comparing RSC utilizing other traditional methods to the method at hand.
CONCLUSIONS
Hydoxyapatite bone cement for retrosigmoid cranioplasty used for the treatment of cranial nerves disorders is an effective method for the prevention of postoperative CSF leaks. Additionally, it is safe due to the lack of deep-seated wound infections and yields good cosmetic results with low incidence of chronic incisional pain. However, this observation reaffirms the necessity for in-depth investigation of the chemical and bio-reactivity properties and differences among available HBC products.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Baird CJ, Hdeib A, Suk I, Francis HW, Holliday MJ, Tamargo RJ. Reduction of cerebrospinal fluid rhinorrhea after vestibular schwannoma surgery by reconstruction of the drilled porus acusticus with hydroxyapatite bone cement. J Neurosurg. 2007. 107: 347-51
2. Bambakidis NC, Munyon C, Ko A, Selman WR, Megerian CA. A novel method of translabyrinthine cranioplasty using hydroxyapatite cement and titanium mesh: A technical report. Skull Base. 2010. 20: 157-61
3. Barker FG, Jannetta PJ, Bissonette DJ, Larkins MV, Jho HD. The long-term outcome of microvascular decompression for trigeminal neuralgia. N Engl J Med. 1996. 334: 1077-83
4. Barker FG, Jannetta PJ, Bissonette DJ, Shields PT, Larkins MV, Jho HD. Microvascular decompression for hemifacial spasm. J Neurosurg. 1995. 82: 201-10
5. Benson AG, Djalilian HR. Complications of hydroxyapatite bone cement reconstruction of retrosigmoid craniotomy: Two cases. Ear Nose Throat J. 2009. 88: E1-4
6. Broggi G, Ferroli P, Franzini A, Servello D, Dones I. Microvascular decompression for trigeminal neuralgia: Comments on a series of 250 cases, including 10 patients with multiple sclerosis. J Neurol Neurosurg Psychiatry. 2000. 68: 59-64
7. Djalilian HR, Benson AG. Complications of hydroxyapatite bone cement reconstruction of retrosigmoid craniotomy. Ear Nose Throat J. 2009. 88: E1-4
8. Dubey A, Sung WS, Shaya M, Patwardhan R, Willis B, Smith D. Complications of posterior cranial fossa surgery - An institutional experience of 500 patients. Surg Neurol. 2009. 72: 369-75
9. Ducic Y. Titanium mesh and hydroxyapatite cement cranioplasty: A report of 20 cases. J Oral Maxillofac Surg. 2002. 60: 272-6
10. Eppley BL, Hollier L, Stal S. Hydroxyapatite cranioplasty: 2. Clinical experience with a new quick-setting material. J Craniofac Surg. 2003. 14: 209-14
11. Foster KA, Shin SS, Prabhu B, Fredrickson A, Sekula RF. Calcium phosphate cement cranioplasty decreases the rate of CSF leak and wound infection compared to titanium mesh cranioplasty: Retrospective study of 672 patients. World Neurosurg. 2016. 95: 414-8
12. Frederickson AM, Sekula RF. The utility of calcium phosphate cement in cranioplasty following retromastoid craniectomy for cranial neuralgias. Br J Neurosurg. 2013. 27: 808-11
13. Fujimaki T, Son J-H, Takanashi S, Ishii T, Furuya K, Mochizuki T. Preservation of the lesser occipital nerve during microvascular decompression for hemifacial spasm.Technical note. J Neurosurg. 2007. 107: 1235-7
14. Jagannath PM, Venkataramana NK, Bansal A, Ravichandra M. Outcome of microvascular decompression for trigeminal neuralgia using autologous muscle graft: A five-year prospective study. Asian J Neurosurg. 2012. 7: 125-30
15. Jannetta PJ, McLaughlin MR, Sekula JR, Jannetta PJ.editors. Microvascular decompression. Trigeminal Neuralgia. New York: Oxford University Press; 2011. p. 192-213
16. Li N, Zhao WG, Pu CH, Shen JK. Clinical application of artificial dura mater to avoid cerebrospinal fluid leaks after microvascular decompression surgery. Minim Invasive Neurosurg. 2005. 48: 369-72
17. Magee WP, Ajkay N, Freda N, Rosenblum RS. Use of fast-setting hydroxyapatite cement for secondary craniofacial contouring. Plast Reconstructive Surg. 2004. 114: 289-97
18. Manjila S, Weidenbecher M, Semaan MT, Megerian CA, Bambakidis NC. Prevention of postoperative cerebrospinal fluid leaks with multilayered reconstruction using titanium mesh-hydroxyapatite cement cranioplasty after translabyrinthine resection of acoustic neuroma. J Neurosurg. 2013. 119: 113-20
19. Marzo SJ, Benscoter B, Leonetti JP. Contemporary options for lateral skull base reconstruction following tumor extirpation. Curr Opin Otolaryngol Head Neck Surg. 2011. 19: 330-4
20. Matic DB, Manson PN. Biomechanical analysis of hydroxyapatite cement cranioplasty. J Craniofac Surg. 2004. 15: 415-22
21. Miller LE, Miller VM. Safety and effectiveness of microvascular decompression for treatment of hemifacial spasm: A systematic review. Br J Neurosurg. 2012. 26: 438-44
22. Moreira-Gonzalez A, Jackson IT, Miyawaki T, Barakat K, DiNick V. Clinical outcome in cranioplasty: Critical review in long-term follow-up. J Craniofac Surg. 2003. 14: 144-53
23. Park JS, Kong DS, Lee JA, Park K. Intraoperative management to prevent cerebrospinal fluid leakage after microvascular decompression: Dural closure with a “plugging muscle” method. Neurosurg Rev. 2007. 30: 139-42
24. Poetker DM, Pytynia KB, Meyer GA, Wackym PA. Complication rate of transtemporal hydroxyapatite cement cranioplasties: A case series review of 76 cranioplasties. Otol Neurotol. 2004. 25: 604-9
25. Ponce-Gómez JA, Martínez-Anda JJ, Barges-Coll J, Perez-Pena N, Revuelta- Gutierrez R. Surgical management of trigeminal neuralgia in elderly patients using a small retrosigmoidal approach: Analysis of efficacy and safety. J Neurol Surg A Cent Eur Neurosurg. 2015. 76: 39-45
26. Shido H, Sakamoto Y, Miwa T, Ohira T, Yoshida K, Kishi K. The RIVET: A novel technique involving absorbable fixation for hydroxyapatite osteosynthesis. J Craniofac Surg. 2013. 24: 946-8
27. Silverman DA, Hughes GB, Kinney SE, Lee JH. Technical modifications of suboccipital craniectomy for prevention of postoperative headache. Skull Base. 2004. 14: 77-84
28. Stoker M, Forbes J, Hanif R, Cooper C, Nian H, Konrad P. Decreased Rate of CSF Leakage Associated with Complete Reconstruction of Suboccipital Cranial Defects. J Neurol Surg B. 2012. 73: 281-6
29. Venkataramana N, Bansal A, Jagannath P, Ravichandra M. Outcome of microvascular decompression for trigeminal neuralgia using autologous muscle graft: A five-year prospective study. Asian J Neurosurg. 2012. 7: 125-
30. Wong RK, Gandolfi BM, St-Hilaire H, Wise MW, Moses M. Complications of hydroxyapatite bone cement in secondary pediatric craniofacial reconstruction. J Craniofac Surg. 2011. 22: 247-51
31. Xia L, Visocchi M, Zhong J, Zhu J, Wang YN, Dou NN. Effectiveness and safety of microvascular decompression surgery for treatment of trigeminal neuralgia: A systematic. J Craniofac Surg. 2014. 25: 1413-7

