

- Adjunct Clinical Professor of Neurological Surgery School of Medicine State University of N.Y. at Stony Brook.
DOI:10.25259/SNI_113_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Nancy E Epstein. Incidence of Major Vascular Injuries with Extreme Lateral Interbody Fusion (XLIF). 18-Apr-2020;11:70
How to cite this URL: Nancy E Epstein. Incidence of Major Vascular Injuries with Extreme Lateral Interbody Fusion (XLIF). 18-Apr-2020;11:70. Available from: https://surgicalneurologyint.com/surgicalint-articles/9967/
Date of Submission
21-Mar-2020
Date of Acceptance
21-Mar-2020
Date of Web Publication
18-Apr-2020
Abstract
Background: Extreme lateral interbody fusions (XLIF) and minimally invasive (MI) XLIF theoretically offer wide access to the lumbar disc space. The theoretical advantages of XLIF include; minimally disturbing surrounding structures (e.g. neural, vascular, soft-tissue), while offering stability. In addition to the well-known increased frequency of neurological deficits attributed to XLIF, here we explored how often major vascular injures occur with XLIF/MI XLIF procedures.
Methods: In 13 XLIF/MI XLIF studies, we evaluated the frequency of major vascular injuries.
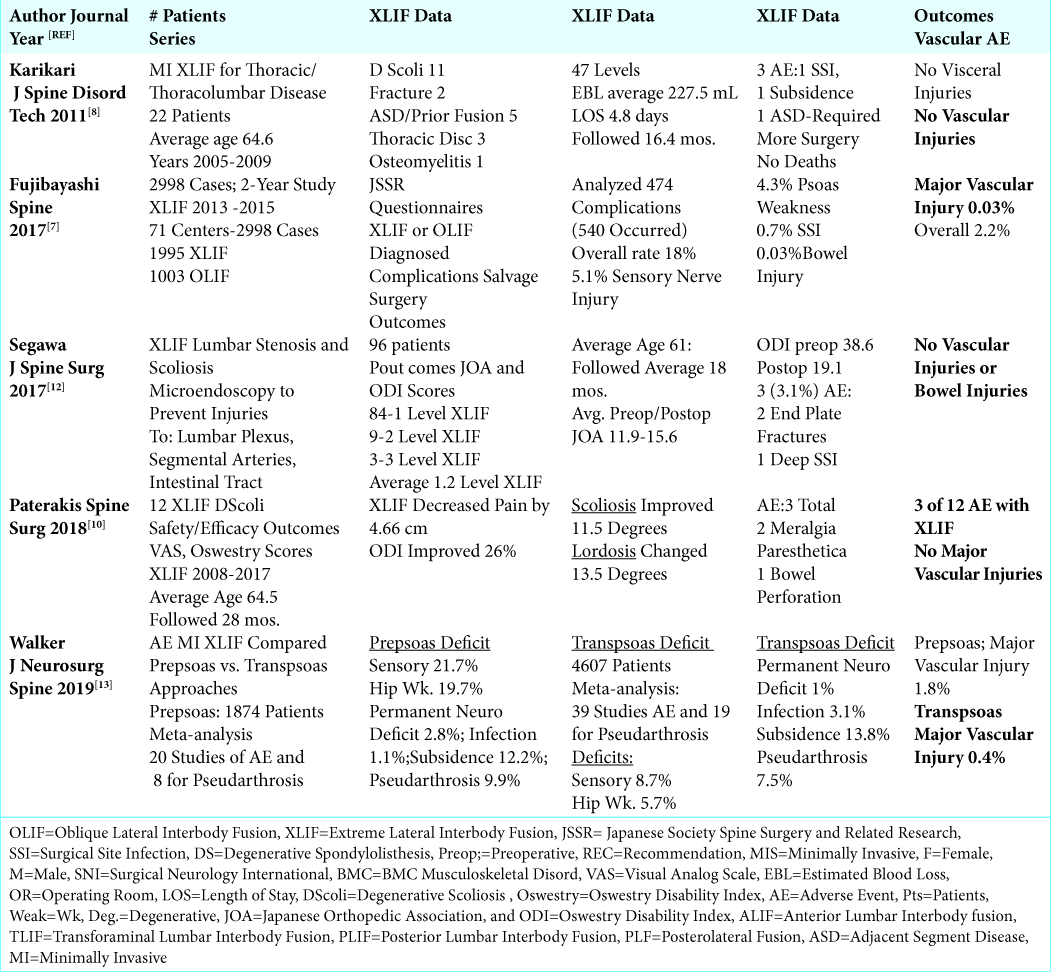
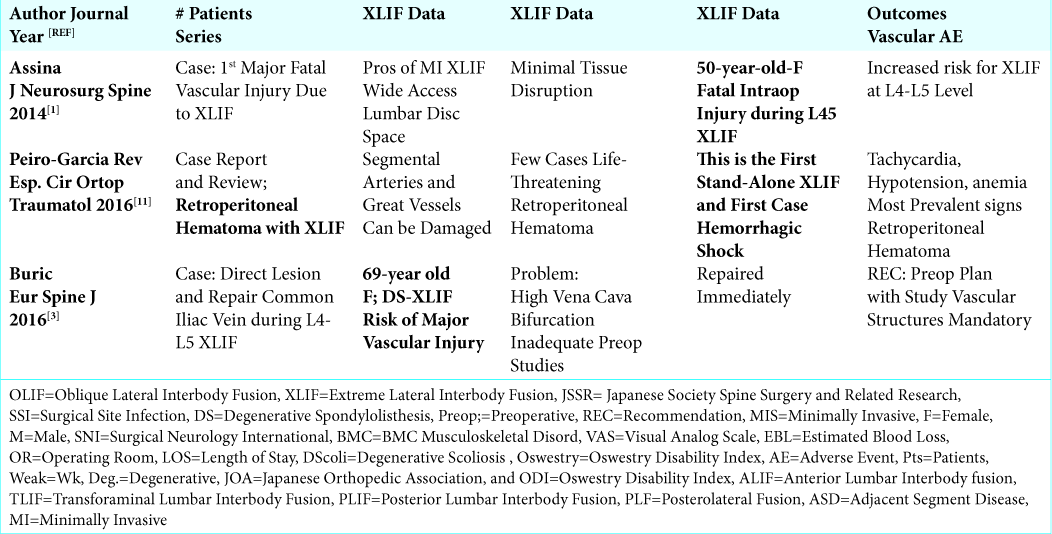
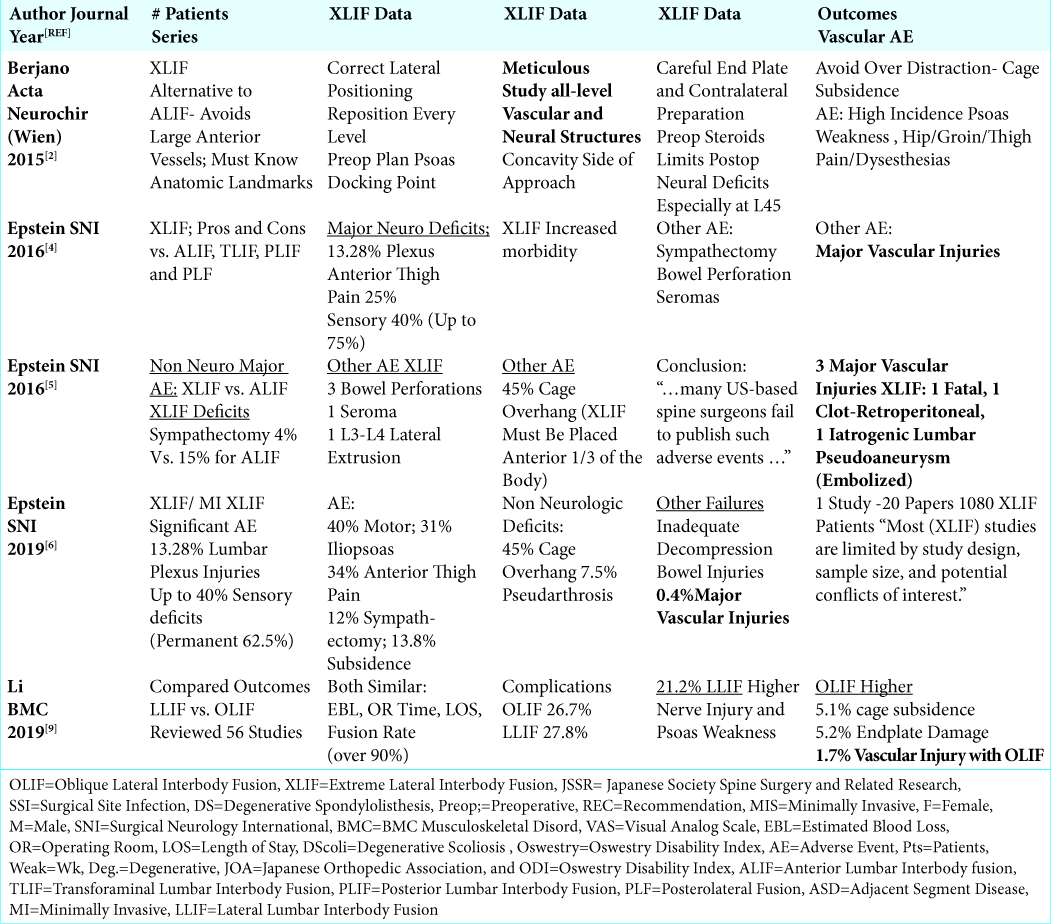
Results: The studies citing the different frequencies of vascular injuries associated with XLIF/MI XLIF were broken down into three categories. Of the 5 small and larger case series, involving a total of 6,732 patients (e.g. range of 12 to 4,607 patients/study), the incidence of vascular injuries ranged from 0% (3 studies) up to 0.4%. Three case reports presented major vascular injuries attributed to XLIF/MI XLIF. Two involved the L4-L5 level. The three complications included: one fatal injury, one, a retroperitoneal hematoma with hemorrhagic shock, and one major vascular injury. For the 5 review articles, major vascular complications were just discussed in 2, one study cited 3 specific major vascular injuries (e.g. 1 fatal, 1 life threating, and 1 lumbar artery pseudoaneurysm requiring embolization), while 2 other studies stated the frequency of these injuries was 0.4% for XLIF, and 1.7 % for OLIF (Oblique Lumbar Interbody Fusion).
Conclusions: According to 5 small and larger case series, 3 case reports, and 5 review articles, the incidence of major vascular injuries occurring during XLIF/MI XLIF ranges from 0 to 0.03% to 0.4%.
Keywords: Extreme Lateral, Interbody, Fusion, Vascular Injuries, XLIF
INTRODUCTION
Extreme lateral interbody fusions (XLIF) and minimally invasive (MI) XLIF theoretically offer wide access to the lumbar disc space with the advantages of minimally disturbing surrounding structures (e.g. neural, vascular, soft-tissue), and providing stability. However, in addition to the already known high incidence of neurological deficits attributed to XLIF/MI XLIF procedures, here we analyzed the various frequencies of attendant major vascular injures. Thirteen XLIF/ MI XLIF studies were broken down into three categories; small/large series (5 studies; total of 6,732 patients), case reports (3 studies), and review articles (5 studies) The overall incidence of major vascular injuries occurring with XLIF/MI XLIF ranged from 0% to 0.03% to 0.4% [
Major Vascular Complications in Small/Larger Case Series of XLIF/MI XLIF
The incidence of major vascular injuries occurring for transpsoas XLIF/MI XLIF performed in the 5 small and larger case series involving a total of 6,732 patients (range from 12 to 4,607 patient/series) ranged from 0% (3 studies) to 0.03% (1 study) to 0.4% (1 study) [
Case Reports of XLIF/MI XLIF Involving Major Vascular Complications
There were 3 case reports of major vascular injuries occurring during XLIF/MI XLIF: two occurred during L4-L5 level procedures [
Review Articles on XLIF/MI XLIF Involving Major Vascular Complications
Five review articles reviewed the frequency of major vascular complications occurring during XLIF/MI XLIF [
DISCUSSION
Previous studies recognized the high incidence of neurological complications associated with XLIF/MI XLIF procedures [
Here, we focused on the frequency of major vascular injuries attributed to XLIF/MI XLIF [
Critical Need for Preoperative Studies to Document Location of Major Vessels
Obtaining preoperative diagnostic studies to visualize the location of the major vessels was critical to XLIF/MI XLIF operative planning e.g. for choosing the best and safest docking point(s) for the XLIF/MI XLIF devices.[
Need for Intraoperative Recognition of Major Vascular Injury for XLIF/MI XLIF
It is imperative to immediately recognize an intraoperative major vascular injury while performing XLIF/MI XLIF. This allows for the immediate initiation of acute resuscitative measures. This includes recognizing a misplaced anterior screw on intraoperative films, excessive bleeding from screw holes (with/without removal of the screw), and/or seeing acute changes in vital signs (acute anemia, tachycardia, cardiovascular collapse, and cardiac arrest). Singly or together, these findings may indicate that a major vascular injury has occurred during the XLIF/MI XLIF procedures.
CONCLUSION
An analysis of 5 small and larger case series, 3 case reports, and 5 review articles, revealed the incidence of major vascular injuries occurring during XLIF/MI XLIF ranges from 0 to 0.03% to 0.4%. When choosing to perform XLIF/MI XLIF, preoperative documentation of the location of the major vessels, and intraoperative acknowledgement of the signs of a major vascular injury are critical to operative success.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Assina R, Majmundar NJ, Herschman Y, Heary RF. First report of major vascular injury due to lateral transpsoas approach leading to fatality. J Neurosurg Spine. 2014. 21: 794-8
2. Berjano P, Gautschi OP, Schils F, Tessitore E. Extreme lateral interbody fusion (XLIF®): how I do it. Acta Neurochir (Wien). 2015. 157: 547-51
3. Buric J, Bombardieri D. Direct lesion and repair of a common iliac vein during XLIF approach. Eur Spine J. 2016. 25: 89-93
4. Epstein NE. Extreme lateral lumbar interbody fusion: Do the cons outweigh the pros?. Surg Neurol Int. 2016. 7: S692-S700
5. Epstein NE. Non-neurological major complications of extreme lateral and related lumbar interbody fusion techniques. Surg Neurol Int. 2016. 7: S656-S659
6. Epstein NE. Review of Risks and Complications of Extreme Lateral Interbody Fusion (XLIF). Surg Neurol Int. 2019. 10: 237-
7. Fujibayashi S, Kawakami N, Asazuma T, Ito M, Mizutani J, Nagashima H. Complications Associated With Lateral Interbody Fusion: Nationwide Survey of 2998 Cases During the First 2 Years of Its Use in Japan. Spine (Phila Pa 1976). 2017. 42: 1478-1484
8. Karikari IO, Nimjee SM, Hardin CA, Hughes BD, Hodges TR, Mehta AI. Extreme lateral interbody fusion approach for isolated thoracic and thoracolumbar spine diseases: initial clinical experience and early outcomes. J Spinal Disord Tech. 2011. 24: 368-75
9. Li HM, Zhang RJ, Shen CL. Differences in radiographic and clinical outcomes of oblique lateral interbody fusion and lateral lumbar interbody fusion for degenerative lumbar disease: a meta-analysis. BMC Musculoskelet Disord. 2019. 20: 582-
10. Paterakis KN, Brotis AG, Paschalis A, Tzannis A, Fountas KN. Extreme lateral lumbar interbody fusion (XLIF) in the management of degenerative scoliosis: a retrospective case series. J Spine Surg. 2018. 4: 610-615
11. Peiró-García A, Domínguez-Esteban I, Alía-Benítez J. Retroperitoneal hematoma after using the extreme lateral interbody fusion (XLIF) approach: Presentation of a case and a review of the literature. Rev Esp Cir Ortop Traumatol. 2016. 60: 330-4
12. Segawa T, Inanami H, Koga H. Clinical evaluation of microendoscopy-assisted extreme lateral interbody fusion. J Spine Surg. 2017. 3: 398-402
13. Walker CT, Farber SH, Cole TS, Xu DS, Godzik J, Whiting AC. Complications for minimally invasive lateral interbody arthrodesis: a systematic review and meta-analysis comparing prepsoas and transpsoas approaches. J Neurosurg Spine. 2019. p. 1-15

