

- Department of Neurosurgery, Nara Medical University, Nara, Japan
Correspondence Address:
Ichiro Nakagawa
Department of Neurosurgery, Nara Medical University, Nara, Japan
DOI:10.4103/2152-7806.168066
Copyright: © 2015 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Okamoto A, Nakagawa I, Matsuda R, Nishimura F, Motoyama Y, Park Y, Nakamura M, Nakase H. Intracranial capillary hemangioma in an elderly patient. Surg Neurol Int 23-Oct-2015;6:
How to cite this URL: Okamoto A, Nakagawa I, Matsuda R, Nishimura F, Motoyama Y, Park Y, Nakamura M, Nakase H. Intracranial capillary hemangioma in an elderly patient. Surg Neurol Int 23-Oct-2015;6:. Available from: http://surgicalneurologyint.com/surgicalint_articles/intracranial-capillary-hemangioma-in-an-elderly-patient/
Abstract
Background:Capillary hemangiomas are neoplasms involving skin and soft tissue in infants. These lesions rarely involved an intracranial space and reported age distribution ranges from infancy to middle age. We report an extremely rare case of rapidly rising intracranial capillary hemangioma in an elderly woman.
Case Description:The 82-year-old woman presented with vomiting, reduced level of consciousness, and worsening mental state. Computed tomography showed a contrast-enhanced extra-axial lesion in the left frontal operculum, although no intracranial mass lesion was identifiable from magnetic resonance imaging taken 2 years earlier. Complete surgical excision was performed and histopathological examination diagnosed benign capillary hemangioma consisting of a variety of dilated capillary blood vessels lined by endothelial cells.
Conclusion:This is the first description of rapid growth of an intracranial capillary hemangioma in an elderly woman. These lesions are exceedingly rare in the elderly population, but still show the capacity for rapid growth. Complete excision would prevent further recurrence.
Keywords: Capillary hemangioma, elderly, intracranial
INTRODUCTION
Capillary hemangiomas are benign vascular tumors that involve skin and soft tissues. Although usually located on the face or scalp, they may appear anywhere in the body. These lesions often occur at birth or in early infancy. When located in the intracranial space, they usually manifest in infancy to childhood in males or adolescence to adulthood in females.[
CLINICAL REPORT
An 82-year-old woman presented with vomiting, reduced level of consciousness, and worsening mental state. Mini-mental state examination (MMSE) score was 4/30, and the revised Hasegawa's Dementia Scale (HDS-R) score was 2/30 on admission to our department. The HDS-R stresses the weight of memory and verbal fluency more than the MMSE and is superior to the MMSE for cognitive screening of early Alzheimer's disease. Computed tomography (CT) showed an iso-dense mass lesion without calcification or hemorrhagic changes, and contrast enhancement demonstrated a lesion about 40 mm in diameter in the left frontal operculum. On magnetic resonance imaging (MRI), the lesion appeared hypointense on T1-weighted imaging [
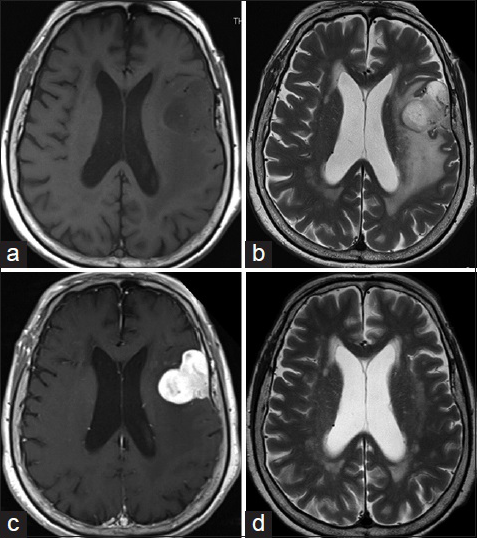
Figure 1
On magnetic resonance imaging, the lesion appears hypointense on T1-weighted imaging (a) and hyperintense with surrounding perifocal edema on T2-weighted imaging (b). Homogeneous enhancement with dural tail sign is seen on T1-weighted imaging (c). Axial T2-weighted imaging 2 years before admission did not suggest any mass lesion in the left frontal operculum (d)
Intraoperatively, the tumor appeared reddish, presented with a rubbery consistency, and was highly vascularized [
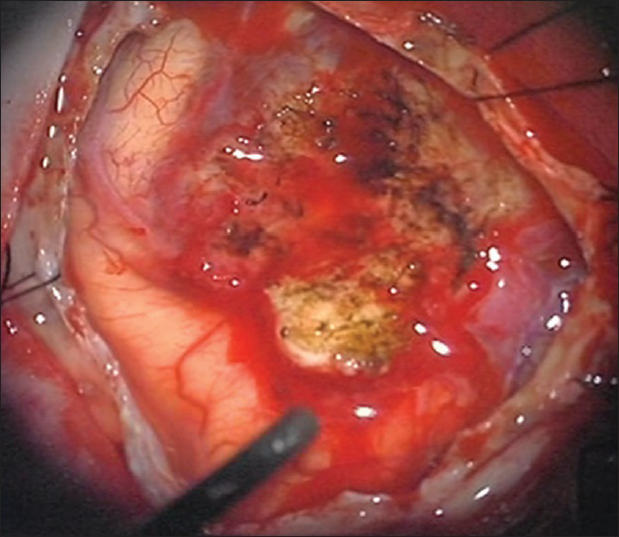
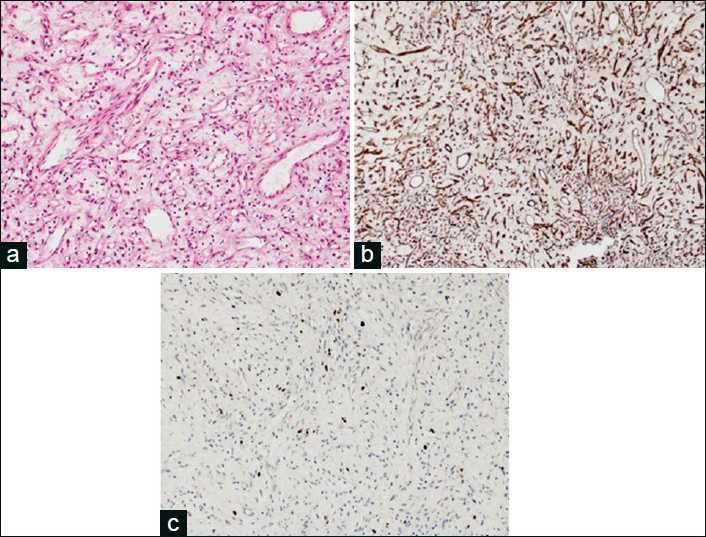
Figure 3
Pathological examination with H and E reveals no nuclear atypia, significant mitotic activity in many capillary vessels and no necrosis (a). Positive results for vascular antigens CD31 (b). CD34 and smooth muscle antigen, and CD163 led to the diagnosis of capillary hemangioma. Ki-67 was about 7% (c). Magnification, ×400
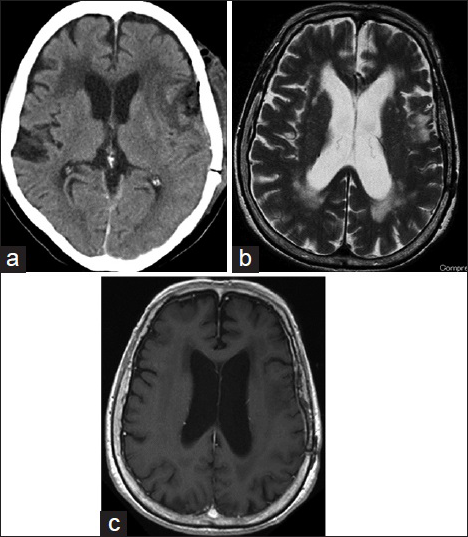
Postoperative CT showed no hemorrhage [
DISCUSSION
This is the first report of intracranial capillary hemangioma developing rapidly in an elderly woman. Capillary hemangioma is considered to be a hamartomatous lesion, that is, commonly found in the skin and soft tissues of infants.[
Radiologically, capillary hemangiomas present as circumscribed hypervascular lesions that resemble meningioma, hemangiopericytoma, and highly vascular metastatic lesions. Meningiomas show some radiological features in common with intracranial capillary hemangiomas. Both present as low-intensity areas on T1-weighted imaging and high-intensity areas on T2-weighted imaging, with intense gadolinium enhancement, whereas multiple flow-voids, intralesional hemorrhage, and the absence of a dural tail or bone changes are described as typical findings in capillary hemangiomas.[
The diagnosis of intracranial capillary hemangiomas is based on histochemical staining or in combination with immunostaining for vascular antigen CD34, CD31, F-γ-related antigen, vascular endothelial growth factor, and smooth muscle antigen. Negative immunostaining for epithelial and melanocytic markers excludes metastases, and immunostaining for estrogen and progesterone receptors also yield negative results. In this case, testing was conducted for CD34, CD31, and smooth muscle antigen. Strong positive results were seen for CD34 and smooth muscle antigen, identifying vascular endothelial cells. Numerous capillary vessels were found and showed oval cells. CD163 also displayed positive results, so almost of the oval cells may have been histiocytes.
The majority of common cutaneous capillary hemangiomas spontaneously regress around school age, so treatment can be reserved for large, disfiguring, or symptomatic lesions. In intracranial capillary hemangiomas, complete resection is central to the treatment of symptomatic lesions, and use of adjuvant radiotherapy should be considered for unresectable or incompletely resected lesions.[
CONCLUSIONS
This is the first description of rapid growth of an intracranial capillary hemangioma in an elderly woman. These lesions are exceedingly rare in the elderly population, but still show the capacity for rapid growth. Complete excision seems most likely to prevent further recurrence.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Mirza B, Shi WY, Phadke R, Holton JL, Turner C, Plant GT. Strawberries on the brain – Intracranial capillary hemangioma: Two case reports and systematic literature review in children and adults. World Neurosurg. 2013. 80: 900.e13-21
2. Morace R, Marongiu A, Vangelista T, Galasso V, Colonnese C, Giangaspero F. Intracranial capillary hemangioma: A description of four cases. World Neurosurg. 2012. 78: 191.E15-21
3. Phi JH, Kim SK, Cho A, Kim DG, Paek SH, Park SH. Intracranial capillary hemangioma: Extra-axial tumorous lesions closely mimicking meningioma. J Neurooncol. 2012. 109: 177-85
4. Simon SL, Moonis G, Judkins AR, Scobie J, Burnett MG, Riina HA. Intracranial capillary hemangioma: Case report and review of the literature. Surg Neurol. 2005. 64: 154-9

