

- Department of Neurosurgery, Keck School of Medicine, University of Southern California, Los Angeles, California, USA
- Department of Neurosurgery, Temple University School of Medicine, Philadelphia, PA, USA
- Department of Pathology, Keck School of Medicine, University of Southern California, Los Angeles, California, USA
Correspondence Address:
Martin H. Pham
Department of Neurosurgery, Keck School of Medicine, University of Southern California, Los Angeles, California, USA
DOI:10.4103/2152-7806.182542
Copyright: © 2016 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Pham MH, Cohen J, Tuchman A, Commins D, Acosta FL. Large solitary osteochondroma of the thoracic spine: Case report and review of the literature. Surg Neurol Int 17-May-2016;7:
How to cite this URL: Pham MH, Cohen J, Tuchman A, Commins D, Acosta FL. Large solitary osteochondroma of the thoracic spine: Case report and review of the literature. Surg Neurol Int 17-May-2016;7:. Available from: http://surgicalneurologyint.com/surgicalint_articles/large-solitary-osteochondroma-of-the-thoracic-spine-case-report-and-review-of-the-literature/
Abstract
Background:Spinal osteochondromas are typically benign tumors, but patients may present with myelopathy and neurologic deficits if there is tumor encroachment within the spinal canal.
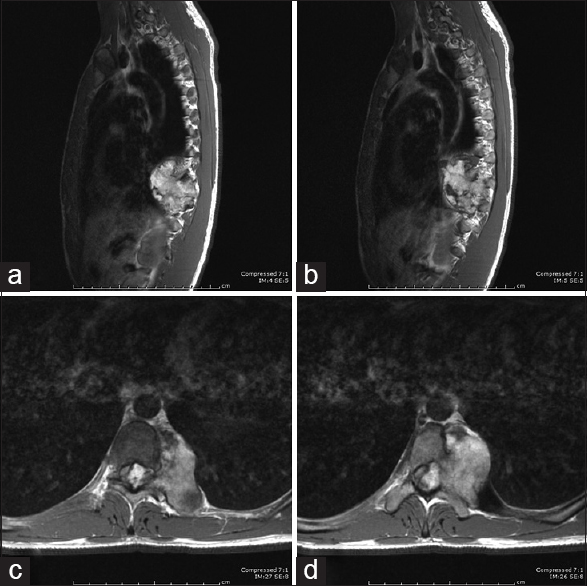
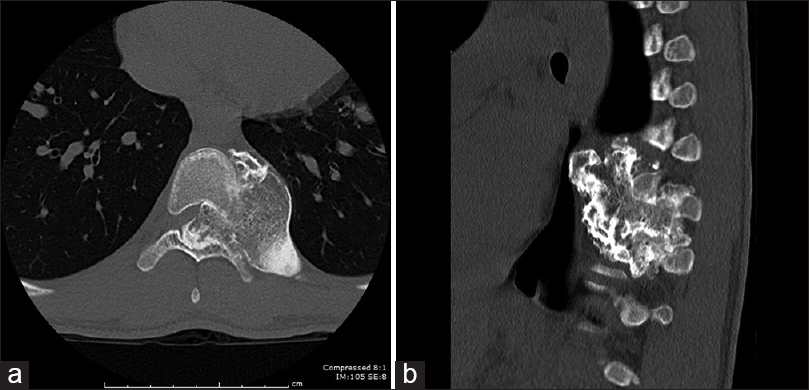
Case Description:We report here a case of a large solitary osteochondroma originating from the posterior vertebral body of T9 causing spinal cord compression and myelopathy. A 17-year-old man presented with 3 months of bilateral feet numbness and gait difficulty. Imaging demonstrated a large left-sided 5.9 cm × 5.0 cm × 5.4 cm osseous mass arising from the T9 vertebra consistent with an osteochondroma. He underwent bilateral costotransversectomies, and a left two-level lateral extracavitary approach for three partial corpectomies to both safely decompress the spinal canal as well as obtain a gross total resection of the tumor. Use of the O-arm intraoperative stereotactic computed tomographic navigation system assisted in delineating the osseous portions of the tumor for surgical removal. He experienced complete neurologic recovery after operative intervention.
Conclusion:Careful surgical planning is needed to determine the best approach for spinal cord decompression and resection of this tumor, especially taking into account the bony elements from which it arises. We present this case, to highlight the feasibility of a single-stage posterior approach to the ventral thoracic spine for the resection of a large solitary thoracic osteochondroma causing cord compression.
Keywords: Costotransversectomy, lateral extracavitary, osteochondroma, thoracic vertebrae
INTRODUCTION
Osteochondroma, known otherwise as “osteocartilaginous exostosis,” is the most common benign tumor of the long bone, and results from abnormal endochondral ossification.[
CASE REPORT
Presentation
A 17-year-old male presented with numbness in both his feet for 3 months duration. His physical examination demonstrated full strength in the lower extremities, but hyperactive ankle knee jerk and ankle jerk reflexes of 3+ (with sustained ankle clonus), and bilateral Babinski responses. Sensory exam showed decreased sensation from the umbilicus down. He had difficulty with tandem gait testing.
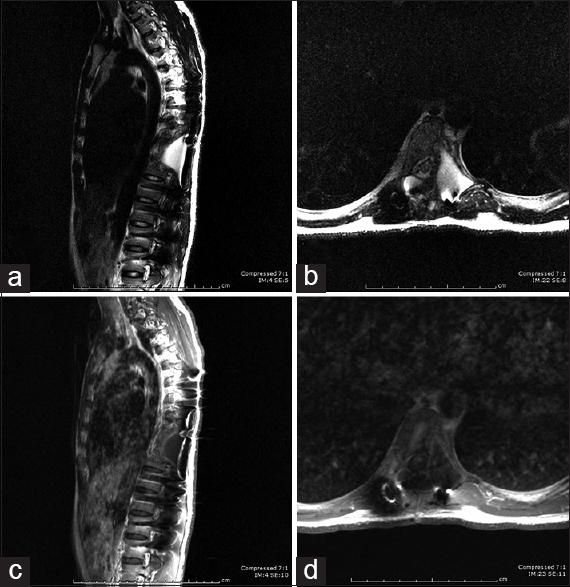
Thoracic magnetic resonance imaging (MRI) showed a large 5.9 cm × 5.0 cm × 5.4 cm mass emanating from the T9–T10 level with severe cord compression [
Operative resection and pathology
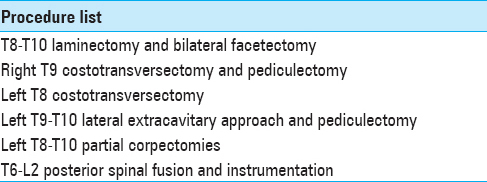
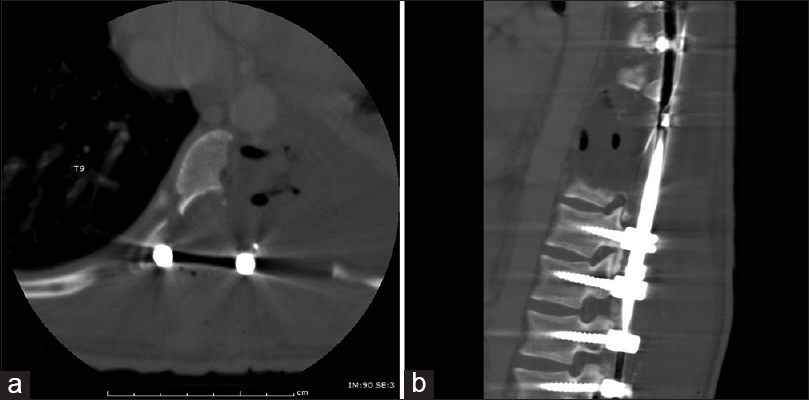
A wide laminectomy and bilateral facetectomy were performed at the T8–T10 levels followed by a right-sided costotransversectomy at T9. A left-sided T8 costotransversectomy and T9–T10 lateral extracavitary approach was now performed, and the lateral borders of the tumor were identified with the assistance of the stereotactic CT navigation system. A partial left-sided T8, T9, and T10 corpectomy was then performed to further decompress the thecal sac and remove the rest of the medial portion of the tumor. Gross total resection of the tumor was achieved and confirmed with the assistance of the stereotactic CT navigation system [
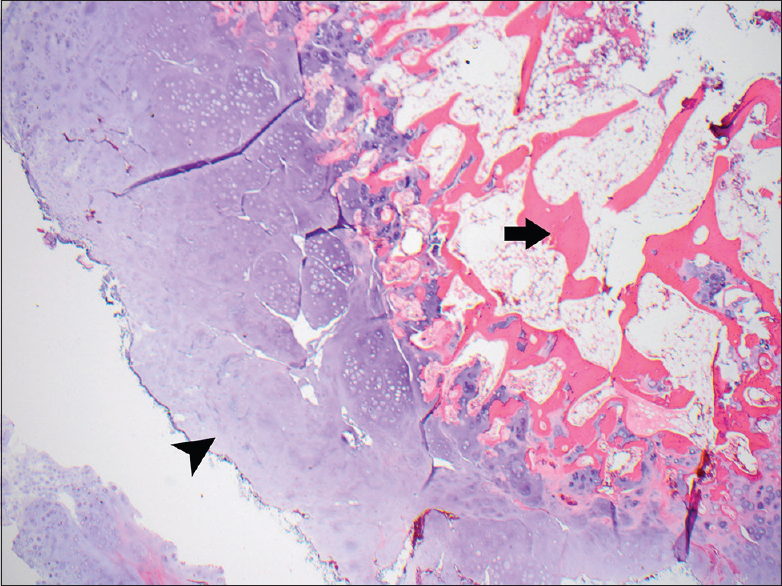
Pathologically, the lesion was noted to have a cartilaginous cap centered by trabecular bone with endochondral ossification at the bone-cartilage interface [
Postoperative care and clinical follow-up
A postoperative CT scan obtained while he was still an inpatient showed gross total resection of the tumor as well as appropriate positioning of the hardware [
DISCUSSION
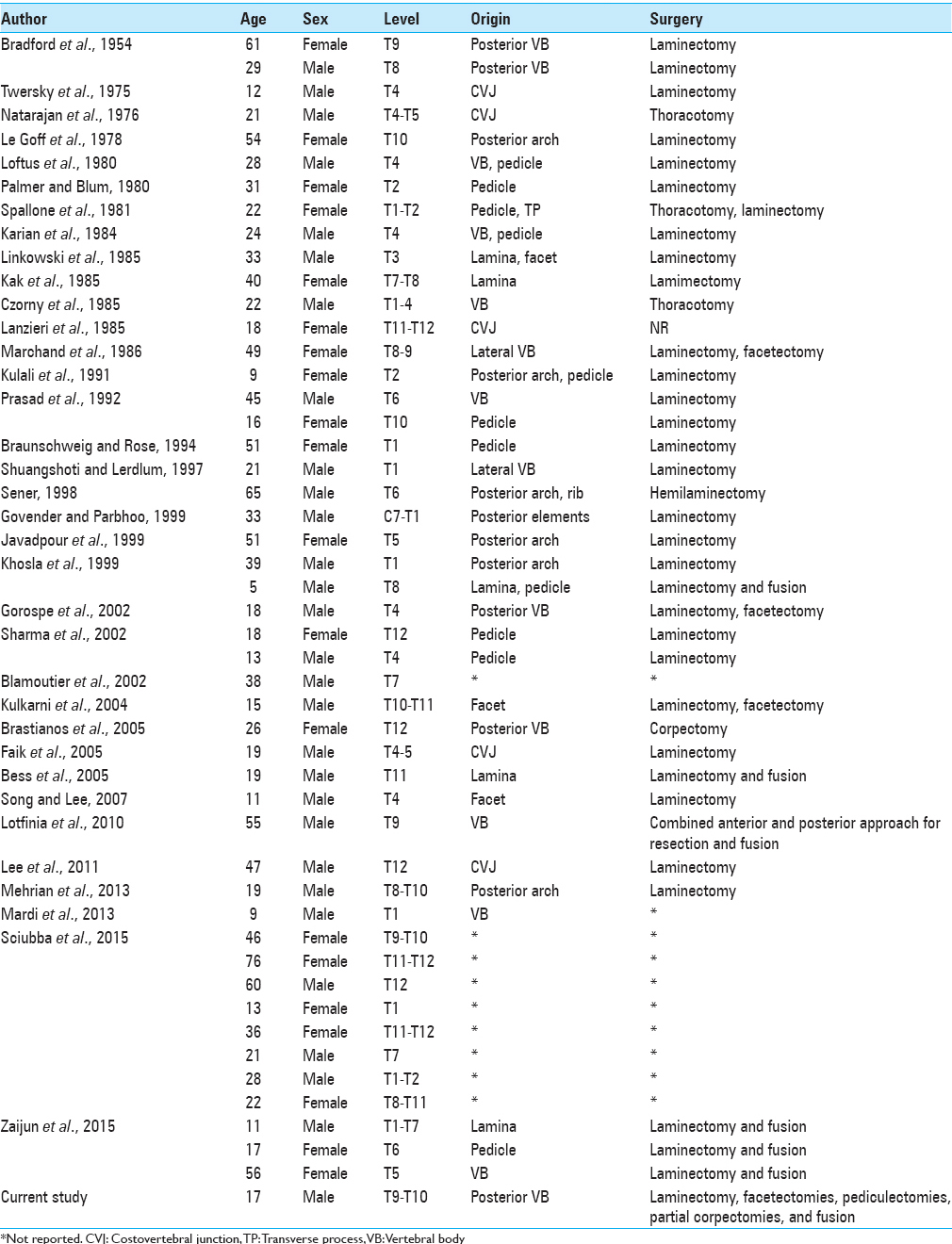
A review of the English-language literature demonstrated 49 cases of solitary thoracic osteochondromas presenting with myelopathy, the majority of which underwent laminectomy for decompression and excision of tumor [
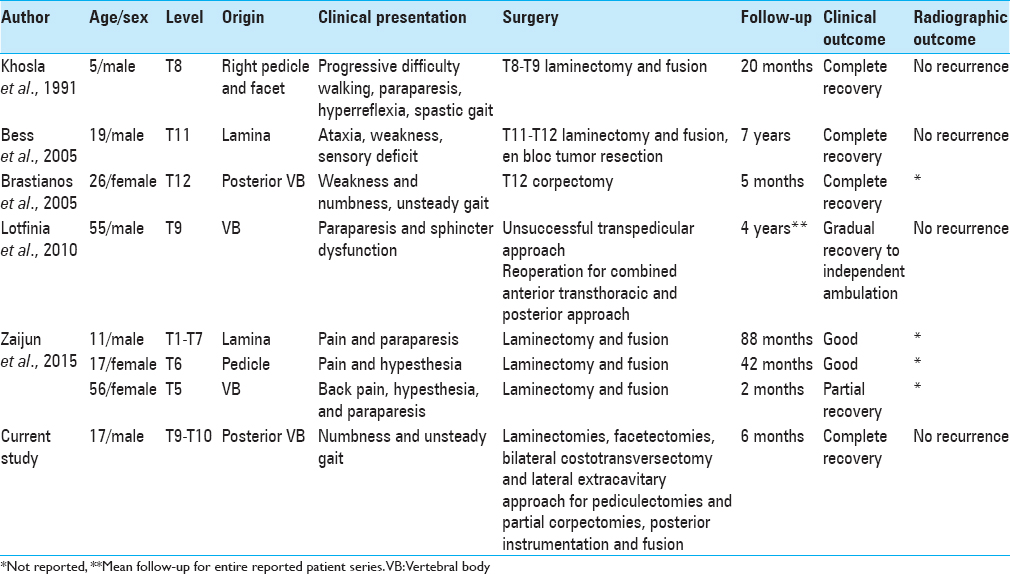
Our patient presented with significant spinal cord compression causing myelopathy from a large osteochondroma originating from the T9 posterior VB. He required bilateral costotransversectomies and a left two-level lateral extracavitary approach for three partial corpectomies to both safely decompress the spinal canal as well as obtain a gross total resection of the tumor. Use of the O-arm intraoperative stereotactic CT navigation system assisted in delineating the osseous portions of the tumor for surgical removal. To our knowledge, this is the first report of a single-stage extensive posterior approach to the ventral thoracic spine for the purpose of osteochondroma resection. We present this case to highlight the feasibility and successful execution of this technique for resection of a solitary thoracic osteochondroma causing cord compression originating from the posterior VB.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Albrecht S, Crutchfield JS, SeGall GK. On spinal osteochondromas. J Neurosurg. 1992. 77: 247-52
2. Brastianos P, Pradilla G, McCarthy E, Gokaslan ZL. Solitary thoracic osteochondroma: Case report and review of the literature. Neurosurgery. 2005. 56: E1379-
3. Gürkanlar D, Aciduman A, Günaydin A, Koçak H, Celik N. Solitary intraspinal lumbar vertebral osteochondroma: A case report. J Clin Neurosci. 2004. 11: 911-3
4. Lotfinia I, Vahedi P, Tubbs RS, Ghavame M, Meshkini A. Neurological manifestations, imaging characteristics, and surgical outcome of intraspinal osteochondroma. J Neurosurg Spine. 2010. 12: 474-89
5. Sharma MC, Arora R, Deol PS, Mahapatra AK, Mehta VS, Sarkar C. Osteochondroma of the spine: An enigmatic tumor of the spinal cord. A series of 10 cases. J Neurosurg Sci. 2002. 46: 66-70

