

- Department of Vascular Neurosurgery, National Institute of Neurology and Neurosurgery ‘Manuel Velasco Suárez’, Mexico City, Mexico.
Correspondence Address:
Edgar Nathal, Department of Vascular Neurosurgery, National Institute of Neurology and Neurosurgery ‘Manuel Velasco Suárez’, Mexico City, Mexico.
DOI:10.25259/SNI_374_2023
Copyright: © 2023 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Javier Degollado-García, Héctor A. Rodríguez-Rubio, Alfredo Bonilla-Suastegui, Alejandro Serrano-Rubio, Carlos F. Nicolas-Cruz, Edgar Nathal. Limitation of fenestrated clips during clipping of middle cerebral artery aneurysm: Technical note. 16-Jun-2023;14:204
How to cite this URL: Javier Degollado-García, Héctor A. Rodríguez-Rubio, Alfredo Bonilla-Suastegui, Alejandro Serrano-Rubio, Carlos F. Nicolas-Cruz, Edgar Nathal. Limitation of fenestrated clips during clipping of middle cerebral artery aneurysm: Technical note. 16-Jun-2023;14:204. Available from: https://surgicalneurologyint.com/surgicalint-articles/12368/
Date of Submission
29-Apr-2023
Date of Acceptance
27-May-2023
Date of Web Publication
16-Jun-2023
Abstract
Background: The middle cerebral artery (MCA) is a common site of cerebral aneurysms and 82.6% occur at the bifurcation. When surgery is selected as a therapeutic option, it intends to clip the neck completely because if some remnant occurs, there exists the possibility of regrowth and bleeding in the short- or long-term.
Methods: We analyzed one drawback of the fenestrated clips of Yasargil and Sugita types to occlude the neck totally at a specific point formed by the union of the fenestra with the blades, creating a triangular space where the aneurysm can protrude, giving place to a remnant that can lead to a future recurrence and rebleeding. We show two cases of ruptured MCA aneurysms in which a cross-clipping technique occluded a broad base and dysmorphic aneurysm using straight fenestrated clips.
Results: In both cases (one using a Yasargil clip and the other with a Sugita clip), a small remnant was visualized when fluorescein videoangiography (FL-VAG) was used. In both cases, the small remnant was clipped with a 3 mm straight miniclip.
Conclusion: We should be aware of this drawback when clipping aneurysms using fenestrated clips to ensure a complete obliteration of the aneurysm’s neck.
Keywords: Aneurysm remnant, Cerebral aneurysm, Clipping surgery, Closure line technique, Middle cerebral artery
INTRODUCTION
Anterior circulation aneurysms represent approximately 85% of all cerebral aneurysms and the middle cerebral artery (MCA) is one of the most common sites of occurrence. About 82.6% of MCA aneurysms occur at the bifurcation.[
Yasargil aneurysm clips
The first generation was made in 1968. Subsequently, the clips have been improved to provide safety, efficacy, stability, and closure force.[
In 2013, the Yasargil fenestrated mini-clips were introduced to the market, leading to a more precise vascular reconstruction in complex cases, reducing the triangle-shaped gap of the large clips and the formation of residual “dog ear” aneurysms at this point.[
Sugita aneurysm clips
Sugita titanium aneurysm clips are made of a titanium alloy termed 6-aluminium-4-vanadiun-titanium (90% titanium, 6% aluminum, and 4% vanadium). A double-coiled flat spring mechanism maintains a stable spring pressure and wide opening of the blades.[
One of the principal differences between Sugita and Yasargil titanium clips is related to their designs. The Sugita clip has a single stabilizing wire to prevent scissoring and maintain the clamping surfaces opposition. The stabilizing wire has no pinching effect of closing. On the other hand, in the Yasargil clips, the blades are welded onto the spring in a “box lock” structure to prevent scissoring.[
MATERIALS AND METHODS
Closure line
The closure line is above the aneurysm that emerges at the time of clipping.[
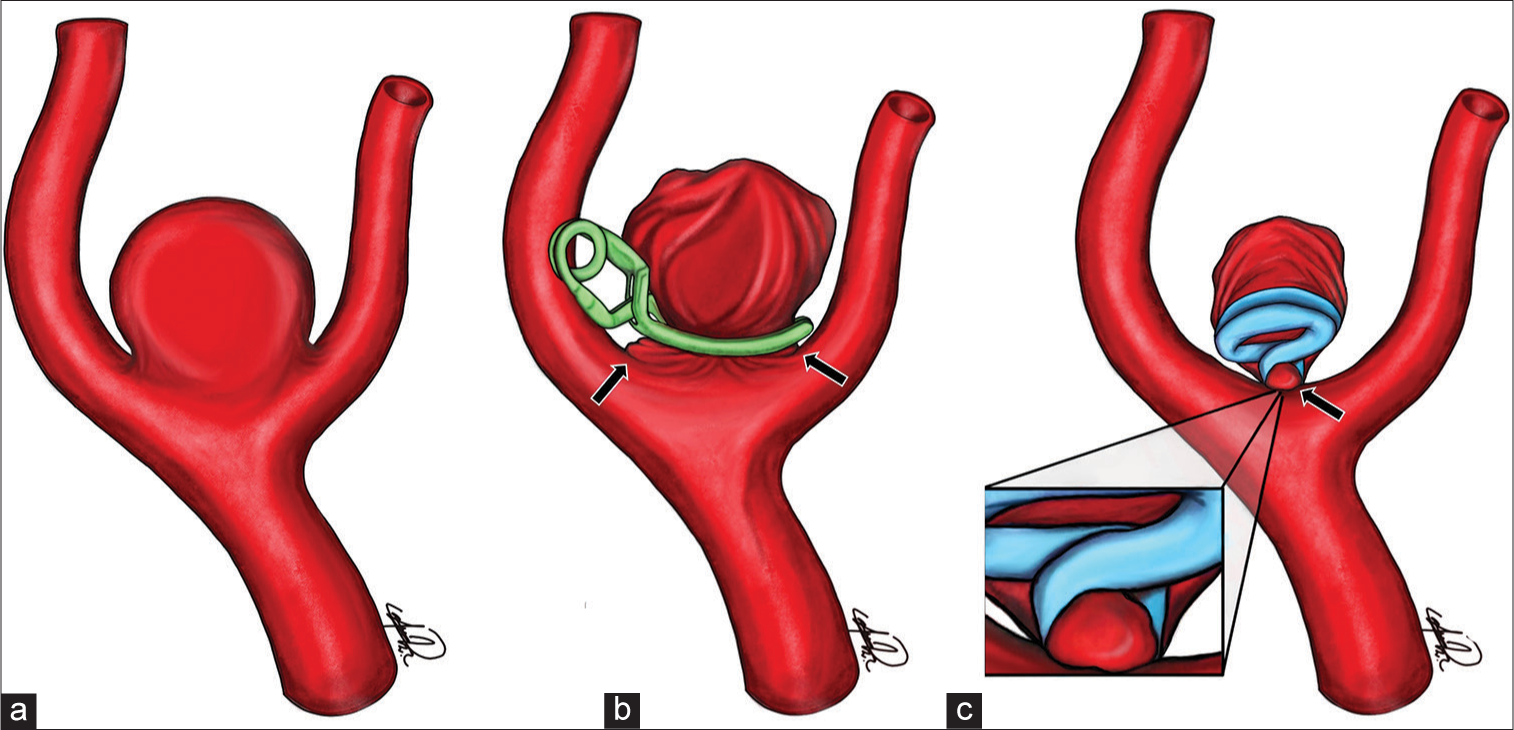
Figure 1:
Illustrations showing parallel and perpendicular clipping in a wide neck middle cerebral artery (MCA) aneurysm. Aneurysm of the MCA bifurcation (a). Parallel clipping to the efferent arteries shows a wide-based residual neck (arrows) (b). Perpendicular clipping to the efferent arteries showing a “dog-ear” shaped residual neck (arrow) (c).
RESULTS
Case 1: Yasargil clip
This 56-year-old male with a history of arterial hypertension was admitted to the hospital because of a sudden onset of a severe headache. CT revealed a right temporal subarachnoid hemorrhage (SAH) [
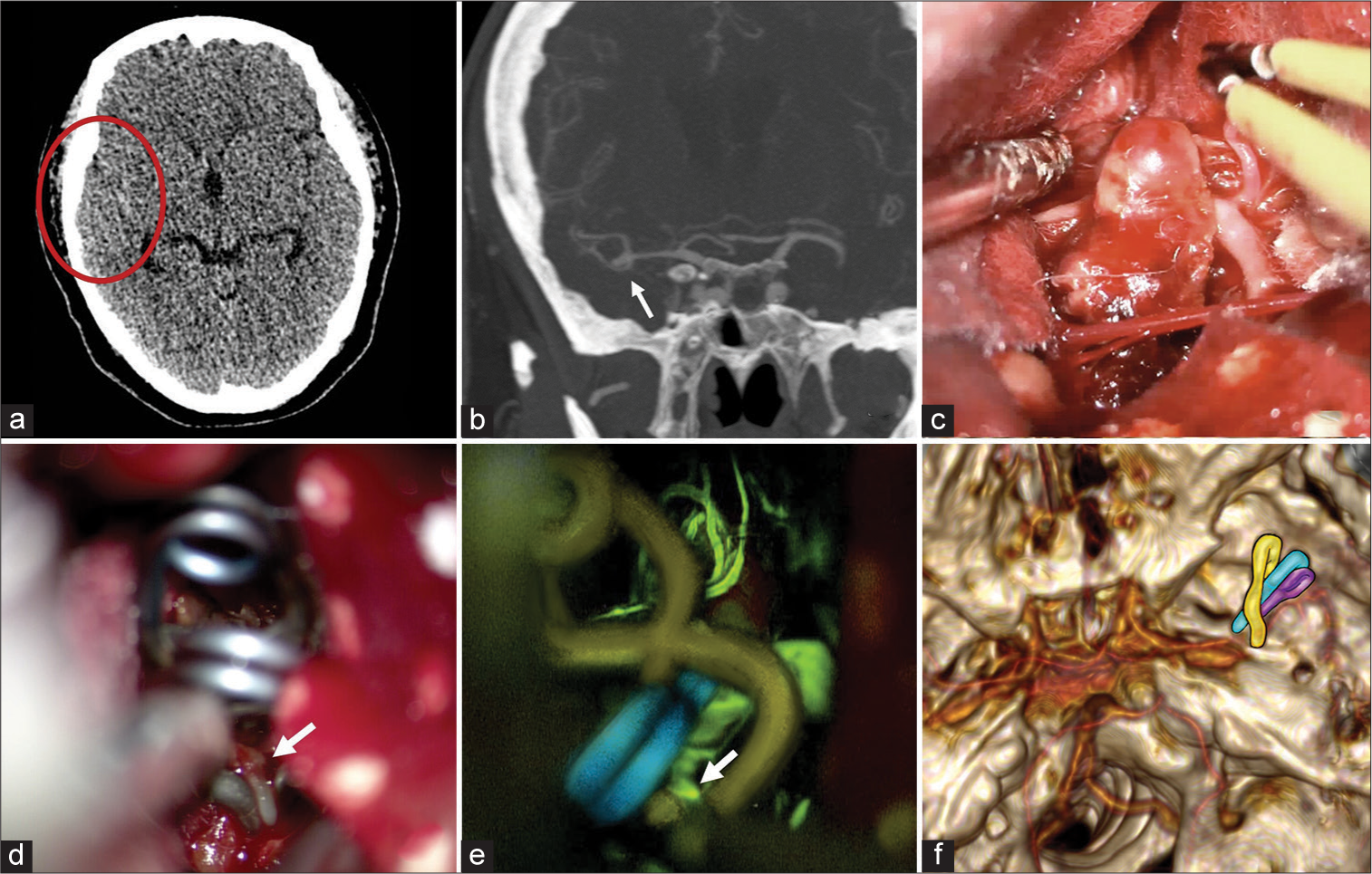
Figure 2:
Computed tomography (CT) scan showing a subarachnoid hemorrhage Fisher 1 in the right middle cerebral artery (MCA) territory (red circle) (a). CT angiography reveals a saccular aneurysm of 11 mm at the bifurcation of the right MCA (arrow) (b). Intraoperative image demonstrating the aneurysm at the MCA’s bifurcation (c). Initial clipping of the aneurysm using a cross-clipping technique with a 7 mm straight clip and a 5 mm straight fenestrated clip, showing a small neck remnant (arrow) (d). Closure confirmation using intraoperative FL-VAG demonstrating a small filling of the aneurysm through the orifice located at the junction of the blades and the fenestra portion of the clip (arrow) (e). A 3 mm straight mini-clip was placed in this small remnant to occlude the aneurysm completely. Postoperative CT angiography displays the three clips’ final arrangement (yellow, blue, and purple structures) (f).
The patient was operated on through a right-side minipterional approach, as Nathal and Gomez-Amador described.[
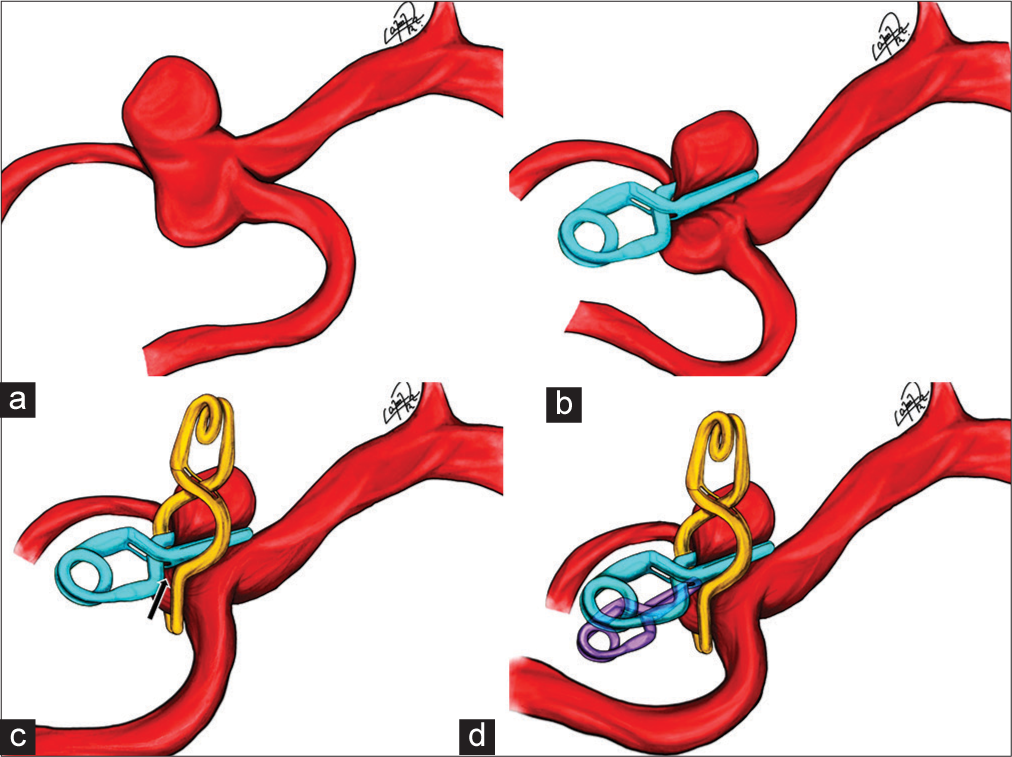
Figure 3:
Illustration showing the clipping of the middle cerebral artery (MCA) bifurcation aneurysm. Bi-lobulated dysmorphic MCA bifurcation aneurysm (a). Initial clipping of the neck using a 7 mm straight clip parallel to M1 segment (b). A second fenestrated clip was set across the primary clip, noticing a small remnant in the fenestra area (arrow) with the fluorescein videoangiography (c). A third straight miniclip was placed to close the remnant left by the fenestrated clip (d).
Case 2: Sugita clip
A 47-year-old female with SAH, Fisher IV, Hunt-Hess II, was admitted to the hospital. Computed tomography showed a right temporal SAH [
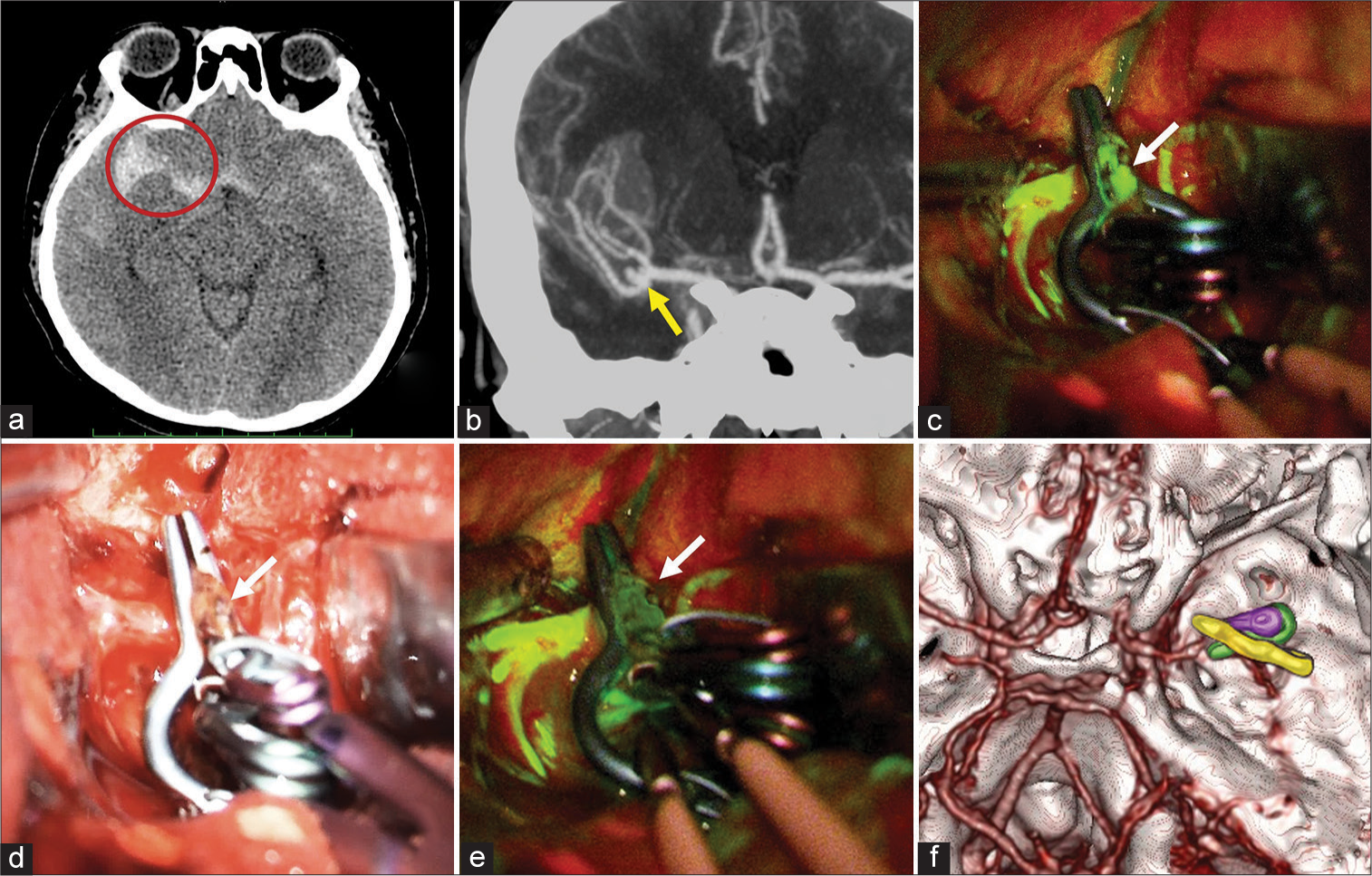
Figure 4:
Computed tomography (CT) scan showing subarachnoid hemorrhage Fisher grade IV in the right middle cerebral artery (MCA) territory (red circle) (a). CT angiography shows a saccular aneurysm of 6 mm at the bifurcation of the right MCA (arrow)(b). Intraoperative view shows the initial clipping of the aneurysm with a 7 mm straight clip in the ventral part of the aneurysm and a 5 mm straight fenestrated clip to the dorsal part, showing a small neck remnant (arrow) that still fills with FL-VAG (c). Total closure with a 3 mm mini clip placed in the filling area through the blades and the fenestration (arrow) (d). Confirmation of the closure using intraoperative FL-VAG (arrow) (e). Postoperative CT angiography shows the three clips’ final arrangement (yellow, green, and purple structures) (f).
DISCUSSION
Closure line concept
Multiple clipping techniques have been reported, such as the tandem technique to eliminate dog-ear remnants.[
Surgical approach
Dissecting the dome entirely before applying the pilot clip is not advisable, but a sharp dissection of the arteries around and adjacent to the base is crucial. The M1-M2 segments and adjacent and perforating branches near the bifurcation should be unhurriedly, clearly, and painstakingly visualized before the final clipping of a bifurcation-type aneurysm neck; the duration of each temporary occlusion should be kept as short as possible (maximum intervals of 5 min). The proximal clip can be close to the bifurcation, but the distal ones should be at a distance so as not to interfere with the visualization and permanent clipping of the neck. A proper selection of clips with different shapes and lengths and applicators, suiting the imaging anatomy of the neck, should be ready for use. If reshaping is not considered, the blade of a single occluding clip should be 1.5 times longer than the width of the base. Temporary clipping of M1 and M2 segments reduces intraluminal pressure; it softens the dome with minimal reduction of the arterial lumen, and a thin portion of the healthy arterial wall is taken inside the clip for safe neck closure. Double tandem clips may be applied if the first clip slides, exposing some part of the neck.[
Although aneurysm recurrence after a technically perfect neck clipping is rare, it can be seen in all large series with careful long-term follow-up. Various clip systems are currently available, but the most popular nowadays are Yasargil and Sugita-type clips; the two blades of an aneurysm clip are responsible for the proper and permanent occlusion of the aneurysm neck while preserving sufficient blood flow through the parent vessel.[
Fenestrated clips drawback
One limitation of Yasargil and Sugita fenestrated clips is the geometric design that produces a small space located at the junction of the blades and spring portions [
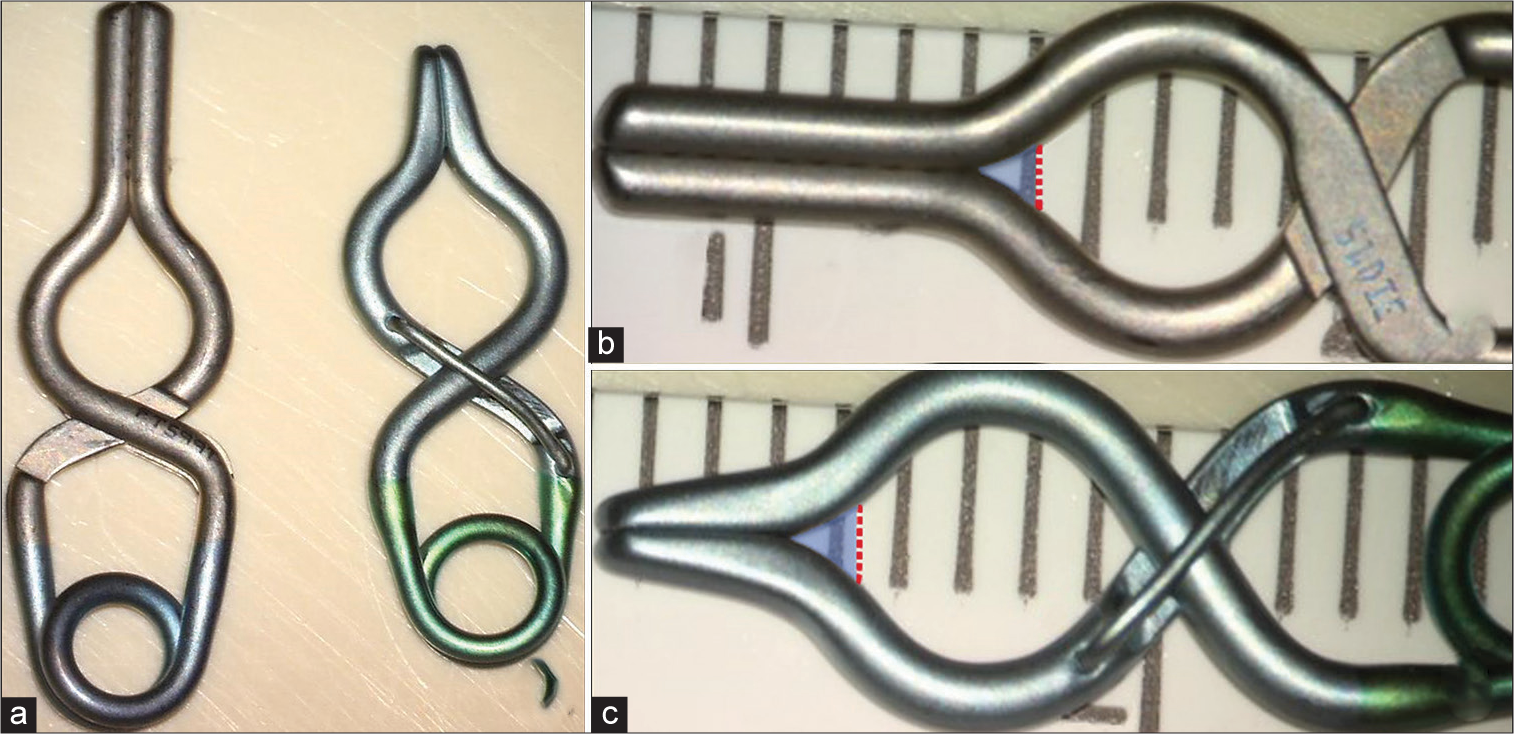
Figure 5:
Comparison of a fenestrated Yasargil (left) and Sugita clip (right) (a). Yasargil and Sugita fenestrated clip showing the triangular-shaped gap in the blue shade (b and c). Notice that the space in both clips is around 1 mm, a little bit larger in the Sugita clips. This area should be revised after clipping to confirm the absence of some remnant.
Neurosurgeons usually pay particular attention to the tip of the clip blades during the clipping procedure, ensuring that all parts of the aneurysm neck are inside the clip. Because of this, there is a general tendency to push the clip too far, resulting in a substantial risk of aneurysm refilling and recurrence at this potentially untreated point during the early postoperative or long-term follow-up.[
Practical solutions to avoid such adverse events might be to use clips with slightly longer blades to prevent placing the clip close to this weak point (triangular-shaped gap) or to apply an additional clip to close the untreated part.
CONCLUSION
When clipping a dysmorphic aneurysm with a wide neck, we should consider the weak points of the fenestrated clips. In this sense, using an intraoperative image, modality such as FL-VAG will help to demonstrate small remnants. These residual necks should be obliterated to avoid the possibility of recurrence in the future. Our proposal for these cases is to place a straight mini clip of 3 mm, closing directly the remnant “dog ear” that sometimes is underestimated, achieving a complete obliteration of the aneurysm.
The closure line concept is a good way of reconstructing the neck anatomically and hemodynamically because, in addition to a complete neck occlusion, it rebuilds the bifurcation from a “T” to a “Y” shape improving the flow dynamics. Due to the complexity and variation of the necks of aneurysms, the selection of clips during surgery is of utmost importance. We should take into account that every clip has some particularities. In this report, we want to bring into focus the triangular area of Yasargil and Sugita fenestrated clip as a possible source of “dog ears” causing a potential aneurysm recurrence.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of patient consent
Patients’ consent not required as patients’ identities were not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Başkaya MK, Uluç K. Application of a new fenestrated clip (Yaşargil T-bar clip) for the treatment of fusiform M1 aneurysm: Case illustration and technical report. Neurosurgery. 2012. 70: 339-42
2. Celik O, Niemelä M, Romani R, Hernesniemi J. Inappropriate application of Yaşargil aneurysm clips: A new observation and technical remark. Neurosurgery. 2010. 66: 84-7 discussion 87
3. David CA, Vishteh AG, Spetzler RF, Lemole M, Lawton MT, Partovi S. Late angiographic follow-up review of surgically treated aneurysms. J Neurosurg. 1999. 91: 396-401
4. Gasparotti R, Liserre R. Intracranial aneurysms. Eur Radiol. 2005. 15: 441-7
5. Horiuchi T, Hongo K, Shibuya M. Scissoring of cerebral aneurysm clips: Mechanical endurance of clip twisting. Neurosurg Rev. 2012. 35: 219-24 discussion 224-5
6. Ishikawa T, Nakayama N, Moroi J, Kobayashi N, Kawai H, Muto T. Concept of ideal closure line for clipping of middle cerebral artery aneurysms--technical note. Neurol Med Chir (Tokyo). 2009. 49: 273-7 discussion 277-8
7. Kobayashi S, Moroi J, Hikichi K, Yoshioka S, Saito H, Tanabe J. Treatment of recurrent intracranial aneurysms after neck clipping: Novel classification scheme and management strategies. Oper Neurosurg (Hagerstown). 2017. 13: 670-8
8. Krammer MJ, Lumenta CB. The new aneurysm clip system for particularly complex aneurysm surgery: Technical note. Neurosurgery. 2010. 66: 336-8
9. Nagy L, Ishii K, Karatas A, Shen H, Vajda J, Niemelä M. Water dissection technique of Toth for opening neurosurgical cleavage planes. Surg Neurol. 2006. 65: 38-41 discussion 41
10. Nathal E, Gomez-Amador JL. Anatomic and surgical basis of the sphenoid ridge keyhole approach for cerebral aneurysms. Neurosurgery. 2005. 56: 178-85 discussion 178-85
11. Ogilvy CS, Crowell RM, Heros RC. Surgical management of middle cerebral artery aneurysms: Experience with transsylvian and superior temporal gyrus approaches. Surg Neurol. 1995. 43: 15-22 discussion 22-4
12. Ota N, Tanikawa R, Noda K, Tsuboi T, Kamiyama H, Tokuda S. The efficiency of the new Yaşargil titanium fenestrated mini-clips for ideal clipping of a cerebral aneurysm. Surg Neurol Int. 2015. 6: S553-9
13. Otawara Y, Ogasawara K, Kashimura H, Kubo Y, Ogawa A, Watanabe K. Mechanical characteristics and surface elemental composition of a Yaşargil titanium aneurysm clip after long-term implantation. J Neurosurg. 2010. 112: 1260-2
14. Papadopoulos MC, Apok V, Mitchell FT, Turner DP, Gooding A, Norris J. Endurance of aneurysm clips: Mechanical endurance of Yaşargil and Spetzler titanium aneurysm clips. Neurosurgery. 2004. 54: 966-70 discussion 970-2
15. Rinne J, Hernesniemi J, Niskanen M, Vapalahti M. Analysis of 561 patients with 690 middle cerebral artery aneurysms: Anatomic and clinical features as correlated to management outcome. Neurosurgery. 1996. 38: 2-11
16. Sugita K, Hirota T, Iguchi I, Mizutani T. Comparative study of the pressure of various aneurysm clips. J Neurosurg. 1976. 44: 723-7
17. Suzuki J, Yoshimoto T, Kayama T. Surgical treatment of middle cerebral artery aneurysms. J Neurosurg. 1984. 61: 17-23
18. Takayasu M, Nagatani T, Noda A, Shibuya M, Yoshida J. Clinical safety and performance of Sugita titanium aneurysm clips. Acta Neurochir (Wien). 2000. 142: 159-62 discussion 162-3
19. Takeda R, Kurita H. “Mass reduction” clipping technique for large and complex intracranial middle cerebral artery aneurysm. World Neurosurg. 2019. 125: 150-5
20. Yaşargil MG, editors. Microneurosurgery. Stuttgart: Georg Thieme Verlag; 1984. 2: 124-64
21. Yaşargil Aneurysm Clip System Brochure. Available from: https://www.aesculapusa.com/content/dam/aesculap-us/us/website/aesculap-inc/healthcareprofessionals/or-soultions/pdfs/DOC697-YASARAGIL%20Aneurysm%20Clip%20System%20Brochure-Rev%20H.pdf [Last accessed on 2015 Feb 02].

