

- Spinal Disorders Center, Fujieda Heisei Memorial Hospital, Fujieda, Japan
- Spinal Disorders Center, Division of Neurosurgery, Shizuoka Cancer Center, Nagaizumi, Japan
Correspondence Address:
Ryo Kanematsu, Spinal Disorders Center, Fujieda Heisei Memorial Hospital, Fujieda, Japan.
DOI:10.25259/SNI_603_2024
Copyright: © 2024 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Ryo Kanematsu1, Junya Hanakita1, Toshiyuki Takahashi1, Manabu Minami1, Koichi Mitsuya2. Long-term survival following molecular-targeted therapy for intramedullary non-small-cell lung cancer metastasis. 30-Aug-2024;15:312
How to cite this URL: Ryo Kanematsu1, Junya Hanakita1, Toshiyuki Takahashi1, Manabu Minami1, Koichi Mitsuya2. Long-term survival following molecular-targeted therapy for intramedullary non-small-cell lung cancer metastasis. 30-Aug-2024;15:312. Available from: https://surgicalneurologyint.com/surgicalint-articles/13068/
Date of Submission
21-Jul-2024
Date of Acceptance
06-Aug-2024
Date of Web Publication
30-Aug-2024
Abstract
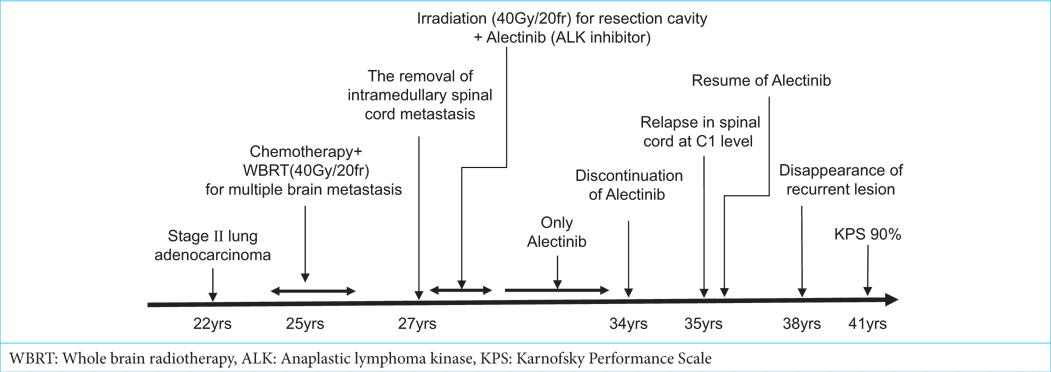
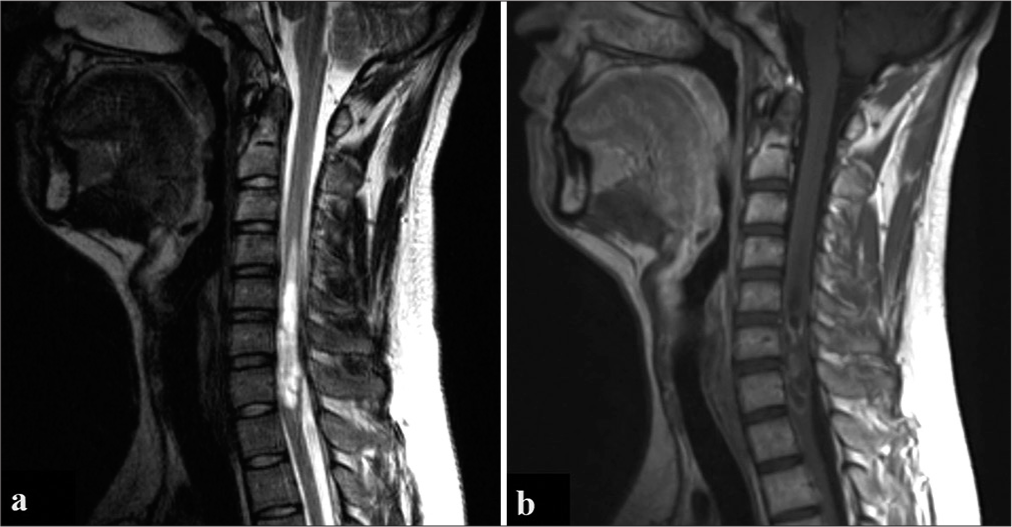
Background: Intramedullary spinal cord metastases (ICSMs) are very rarely curable; these patients typically have very short-term survival rates. Here, a 22-year-old male with non-small-cell lung cancer (NSCLC) later developed ICSM twice; the first C4–C7 tumor responded well to surgery, radiation, and alectinib molecular-targeted therapy. The secondary ICSM C1 lesion seen years later (i.e., likely due to alectinib having been stopped) resolved once alectinib was again administered.
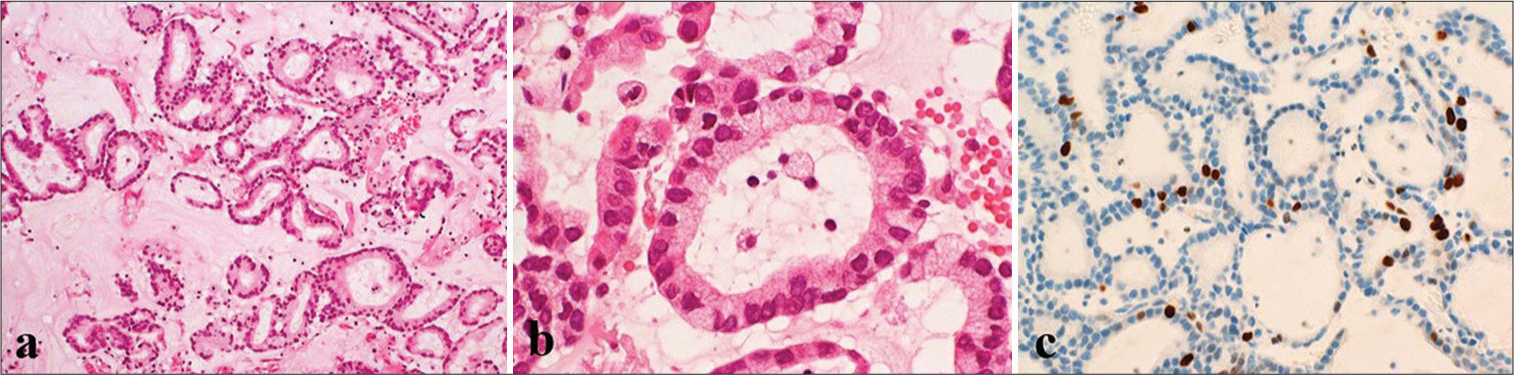
Case Description: A 22-year-old male with a limited smoking history presented with advanced non-small-cell lung cancer (NSCLC) treated with pulmonary surgery followed by radiotherapy and chemotherapy. Four years later, he developed cervical myelopathy attributed to a C4–C7 stage IV NSCLC ICSM (i.e., notably associated with an anaplastic lymphoma kinase [ALK] rearrangement). After cervical surgery and irradiation (40 Gy/20 fr) of the resection cavity, he was also given alectinib; the patient remained disease-free for the next 7 years, remaining on alectinib. However, 1 year after alectinib was discontinued, he experienced a newly occurrent C1 ICSM lesion; the alectinib was restarted, and his tumor regressed over the next 3 years. At present, 14 years after the original ICSM surgery, the patient remains disease free but continued alectinib (Karnofsky Performance Scale: 90%).
Conclusion: Although the prognosis for ICSM is generally poor, molecular-targeted therapies, such as alectinib, as administered in this case, may provide long-term survival for patients with ALK-positive NSCLC tumors.
Keywords: Intramedullary spinal cord metastasis, Molecular-targeted therapy, Non-small-cell lung cancer
INTRODUCTION
Intramedullary spinal cord metastasis (ICSM) is rarely curable. In a meta-analysis involving 284 patients, the median overall survival was 7.3 months.[
CASE DESCRIPTION
A 22-year-old male with a limited smoking history presented with Stage II lung NSCLC adenocarcinoma (i.e., harboring an ALK rearrangement) [

DISCUSSION
Molecular-targeted therapy for metastases in the central nervous system
We have summarized the characteristics of patients with ICSM from NSCLC who have achieved long-term survival [

CONCLUSION
Although the prognosis for ICSM/NSCLC tumors is generally poor, molecular-targeted therapy with alectinib in a patient with a tumor showing ALK-positive gene rearrangement has, thus far, survived 14 years following the original NSCLC surgery.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Biya J, Caramella C, Lindsay CR, Planchard D, Besse B. A long-term spinal intramedullary response to ceritinib in ALK rearranged non-small-cell lung cancer. J Thorac Oncol. 2015. 10: e44-5
2. Gainor JF, Ou SH, Logan J, Borges LF, Shaw AT. The central nervous system as a sanctuary site in ALK-positive non-small-cell lung cancer. J Thorac Oncol. 2013. 8: 1570-3
3. Hata Y, Takai Y, Takahashi H, Takagi K, Isobe K, Hasegawa C. Complete response of 7 years’ duration after chemoradiotherapy followed by gefitinib in a patient with intramedullary spinal cord metastasis from lung adenocarcinoma. J Thorac Dis. 2013. 5: E65-7
4. Johung KL, Yeh N, Desai NB, Williams TM, Lautenschlaeger T, Arvold ND. Extended survival and prognostic factors for patients with ALK-rearranged non-small-cell lung cancer and brain metastasis. J Clin Oncol. 2016. 34: 123-9
5. Kalayci M, Cağavi F, Gül S, Yenidünya S, Açikgöz B. Intramedullary spinal cord metastases: Diagnosis and treatment-An illustrated review. Acta Neurochir (Wien). 2004. 146: 1347-54 discussion 1354
6. Kodama K, Kimura Y, Momozane T, Sigetsu K, Takeda M, Kishima H. Long-term treatment with ALK inhibitors for postoperative recurrence of ALK-rearranged lung cancer. Int Cancer Conf J. 2022. 11: 238-41
7. Li Y, Zhang T, Zhang J, Li W, Yuan P, Xing P. Response to crizotinib in advanced ALK-rearranged non-small cell lung cancers with different ALK-fusion variants. Lung Cancer. 2018. 118: 128-33
8. Nishino M, Soejima K, Mitsudomi T. Brain metastases in oncogene-driven non-small cell lung cancer. Transl Lung Cancer Res. 2019. 8: S298-307
9. Sperduto PW, Kased N, Roberge D, Xu Z, Shanley R, Luo X. Summary report on the graded prognostic assessment: An accurate and facile diagnosis-specific tool to estimate survival for patients with brain metastases. J Clin Oncol. 2012. 30: 419-25

