

- Department of Neurosurgery, Icahn School of Medicine at Mount Sinai, New York, NY, United States.
- Department of Medical Education, New York University School of Medicine, New York, NY, United States.
- Department of Medical Education, Icahn School of Medicine at Mount Sinai, New York, NY, United States.
Correspondence Address:
Remi A. Kessler
Department of Neurosurgery, Icahn School of Medicine at Mount Sinai, New York, NY, United States.
DOI:10.25259/SNI_403_2019
Copyright: © 2019 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Remi A. Kessler, Jeremy Steinberger, Sabrina Chen, Rebecca Baron, John M. Caridi. Lung adenocarcinoma presumed to be Pott’s disease in a 28-year-old patient: A case report and review of literature. 18-Oct-2019;10:208
How to cite this URL: Remi A. Kessler, Jeremy Steinberger, Sabrina Chen, Rebecca Baron, John M. Caridi. Lung adenocarcinoma presumed to be Pott’s disease in a 28-year-old patient: A case report and review of literature. 18-Oct-2019;10:208. Available from: http://surgicalneurologyint.com/surgicalint-articles/9716/
Date of Submission
04-Sep-2019
Date of Acceptance
25-Sep-2019
Date of Web Publication
18-Oct-2019
Abstract
Background: Tuberculous spondylitis (Pott’s disease), a common extrapulmonary manifestation of tuberculosis (TB), typically presents with back pain, tenderness, paraparesis/paraplegia, and various constitutional symptoms. Due to radiological similarities between Pott’s disease and lung cancer, some lung cancer patients may initially be erroneously diagnosed and treated for TB, allowing for extensive progression of their cancer.
Case Description: A 28-year-old male presented with a chronic dry cough, weight loss, and 2 months of increased back pain accompanied by bilateral lower extremity weakness. Magnetic resonance imaging revealed an epidural collection causing compression of the spinal cord at the T5-T6 level. The initial diagnosis was Mycobacterium tuberculosis/Pott’s disease. A thoracic T4-T8 decompression fusion was performed; however, pathologic examination of the tissue revealed adenocarcinoma. Postoperatively, after the patient experienced several episodes of acute respiratory distress and a tension pneumothorax, lung imaging confirmed multiple tumor infiltrates along with lung cancer extending into the thoracic vertebrae. Pelvic studies also confirmed the presence of pelvic metastases. The patient passed away 3 weeks following surgery.
Conclusion: In this case report, a 28-year-old male was treated for thoracic Pott’s disease that proved to be metastatic lung adenocarcinoma. To avoid such misdiagnoses in the future, physicians should better differentiate spinal TB from other malignancies that may affect the spine. This study underscores the importance of obtaining at least a chest X-ray in any patient with suspected Pott’s disease, irrespective of age, to help rule out lung cancer or other pathologies.
Keywords: Lung adenocarcinoma, Mycobacterium tuberculosis, Pott’s disease, Spine, Thoracic, Vertebra
INTRODUCTION
Tuberculous spondylitis, or tuberculosis (TB) of the spine (Pott’s disease), is a common extrapulmonary manifestation of TB.[
Pott’s disease is included among the differential diagnoses for patients presenting with spondylitis, intraspinal or paravertebral abscess, and/or progressive back pain with pulmonary nodules.[
Here, we present a 28-year-old male originally diagnosed with Pott’s disease who underwent a T5-T6 decompression with T4-T8 fusion; at surgery, the lesion proved to be an adenocarcinoma of the lung. Further imaging of the thoracic region revealed a moderate left lung effusion accompanied by a lung mass and metastatic lung cancer extending into the T5-T6 vertebrae. Abdominal studies later additionally confirmed metastases to the pelvis. This study underscores the importance of obtaining at least a chest X-ray in a patient with suspected Pott’s disease, irrespective of age, to help rule out lung cancer or other tumor or nonneoplastic pathologies.
CASE DESCRIPTION
History and physical examination
A 28-year-old male presented with a chronic dry cough and weight loss of 1-year duration, and 2 months of worsening mid-thoracic back pain accompanied by bilateral lower extremity weakness. Notably, there were no known TB exposure, recent travel, smoking, or history of intravenous drug use. On the initial physical examination, he had bilateral rales and left lower extremity weakness (4/5).
Imaging
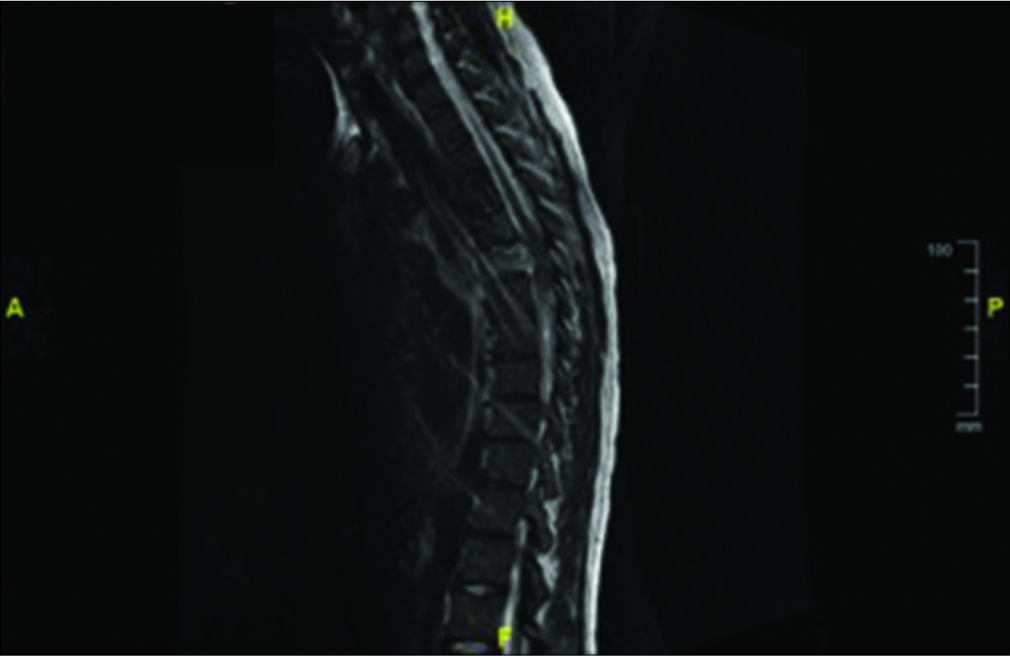
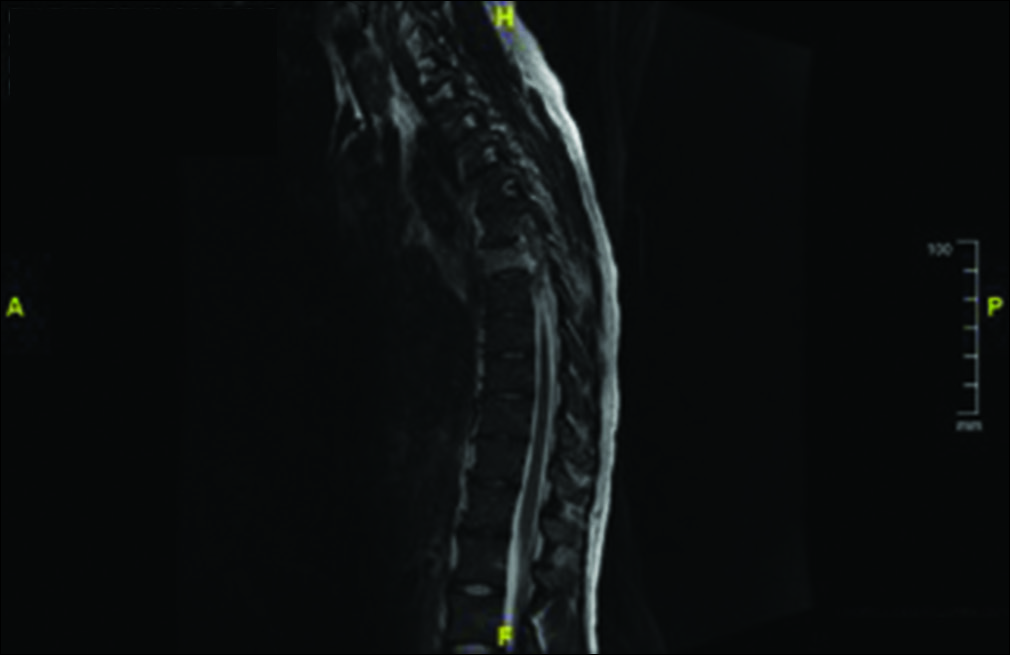
Magnetic resonance imaging revealed an epidural collection causing compression of the spinal cord from T5 to T6; this was accompanied by a moderate-sized, left-sided pleural effusion, a left lingular/lower lobe consolidation, and multiple cavitary lesions in the right lung [


Surgical treatment
Surgery included a T5-T6 decompression (e.g., costotransversectomy); the largely ventral mass (e.g., anterior to the cord) was removed. This was followed by open reduction and a posterior T4-T8 fusion.
Pathology
A 1.2 cm × 0.9 cm × 0.6 cm bone tissue fragment from the T6 lamina and 3.0 cm × 2.0 cm × 1.0 cm aggregate from the T6 epidural tissue demonstrated metastatic adenocarcinoma, likely primary from the lung.
Postsurgical course
The patient’s postoperative course was complicated by an inability to be weaned off the ventilator; the high oxygen requirements were attributed to the left lung disease. A chest radiograph performed the day of surgery demonstrated an enlarging left pleural effusion and a left pneumothorax. There were also patchy right perihilar airspace opacities/scattered nodules, considered infectious/inflammatory [

DISCUSSION
The diagnosis of TB, and especially extrapulmonary TB, requires a complete evaluation.[
Radiological similarities with Pott’s disease versus lung cancer
Due to radiological similarities, it is possible that lung cancer patients may initially be erroneously diagnosed and treated for TB rather than lung cancer. This may lead to delays in the diagnosis and appropriate treatment of their lung cancer. Such delays should be avoided to limit extension and/or progression of their cancer; performing X-ray, computed tomography (CT) scan/fiberoptic bronchoscopy may help avoid the failure to differentiate lung opacities due to TB versus lung cancer.[
Lung cancer
In patients under 25 years of age, NSCLC is extremely rare (i.e., 0.3/100,000).[
Treatment options
In this case, had the authors been aware of the underlying diagnosis of lung cancer with multiple metastases, they would not have proceeded with the spinal decompression/ fusion surgery (e.g., instead utilization of CT-guided biopsy and appropriate treatment of lung cancer). Spinal surgeons should be cognizant that spinal metastases secondary to lung adenocarcinoma may mimic Pott’s disease and should obtain preoperative chest X-rays to rule out other pathologies including lung cancer; in this case, it would have avoided unnecessary spinal surgery.
CONCLUSION
Spinal surgeons should be aware of the shared radiological features for Pott’s disease/spinal TB versus other metastatic malignancies (e.g., lung cancer). In this case, a 28-year- old who was misdiagnosed with Pott’s disease at the T5- T6 level would not have undergone unnecessary spine surgery (e.g., T4-T8 decompression/fusion) but rather would have been appropriately treated for lung cancer (e.g., stereotactic CT-guided biopsy and chemotherapy/ radiation therapy).
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Ansari S, Amanullah MF, Ahmad K, Rauniyar RK. Pott’s spine: Diagnostic imaging modalities and technology advancements. N Am J Med Sci. 2013. 5: 404-11
2. Kaila R, Malhi AM, Mahmood B, Saifuddin A. The incidence of multiple level noncontiguous vertebral tuberculosis detected using whole spine MRI. J Spinal Disord Tech. 2007. 20: 78-81
3. Khan O, Tong WP, Karlin NJ. Metastatic lung adenocarcinoma in a 20-year-old patient. Curr Oncol. 2010. 17: 56-8
4. Pertuiset E, Beaudreuil J, Lioté F, Horusitzky A, Kemiche F, Richette P. Spinal tuberculosis in adults. A study of 103 cases in a developed country, 1980-1994. Medicine (Baltimore). 1999. 78: 309-20
5. Ringshausen FC, Tannapfel A, Nicolas V, Weber A, Duchna HW, Schultze-Werninghaus G. A fatal case of spinal tuberculosis mistaken for metastatic lung cancer: Recalling ancient Pott’s disease. Ann Clin Microbiol Antimicrob. 2009. 8: 32-
6. . Available from: http://www.ahrq.gov/clinic/uspstf/uspslung.htm [Last accessed on 2019 Oct 06].
7. .editors. United States, National Institutes of Health, National Cancer Institute, Surveillance Epidemiology and End Results (seer) Cancer Statistics Review, 1975-2006. Bethesda, MD: National Cancer Institute, Cancer Statistics Branch; 2009. p.
8. .editors. Global Tuberculosis Control: Surveillance, Planning, Financing. WH Report. 2008. p.

