

- Department of Neurosurgery, Max Super Speciality Hospital, Saket, New Delhi, India
Correspondence Address:
Kapil Jain
Department of Neurosurgery, Max Super Speciality Hospital, Saket, New Delhi, India
DOI:10.4103/sni.sni_478_17
Copyright: © 2018 Surgical Neurology International This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.How to cite this article: Saraj K. Singh, Kapil Jain, Vijendra K. Jain, Arun Saroha. Mirror image of bilateral DACA aneurysm with its successful surgical management. 10-Apr-2018;9:80
How to cite this URL: Saraj K. Singh, Kapil Jain, Vijendra K. Jain, Arun Saroha. Mirror image of bilateral DACA aneurysm with its successful surgical management. 10-Apr-2018;9:80. Available from: http://surgicalneurologyint.com/surgicalint-articles/mirror-image-of-bilateral-daca-aneurysm-with-its-successful-surgical-management/
Date of Submission
17-Dec-2017
Date of Acceptance
07-Mar-2018
Date of Web Publication
10-Apr-2018
Abstract
Background:Among various locations of intracranial aneurysms reported in the literature, two different aneurysms situated symmetrically opposite on bilateral distal anterior cerebral arteries (DACA) are very rare.
Case Description:Here, we report a rare case of mirror image distal anterior cerebral aneurysm in a middle-aged male patient. The patient presented with severe headache and loss of consciousness. Angiography was done which suggested mirror imaging of two aneurysms located over both DACA. It was treated through microsurgical approach with a successful outcome.
Conclusion:Careful analysis of intracranial vasculature should be done using angiography, particularly in different views and stages to rule out multiple aneurysms at different locations in the same artery or at different arteries. Mirror images of bilateral DACA aneurysms are very rare. Fundamental surgical strategy of securing the parent artery and clipping the neck after meticulous dissection should be followed.
Keywords: Clipping, corpus callosum, DACA aneurysm, DSA, frontal craniotomy
INTRODUCTION
Among various locations of intracranial aneurysms reported in the literature, two different aneurysms situated on both distal anterior cerebral arteries (DACA) are very rare.[
CASE REPORT
A 45-year-old male patient reported to the casualty with a history of sudden-onset severe headache with loss of consciousness for 1 day. On examination, the patient was E1M5V1, vitals were stable, pupil was normal sized and reacting to light, and there were no focal deficits. Patient came with noncontrast computed tomography (NCCT) of the head [Figure
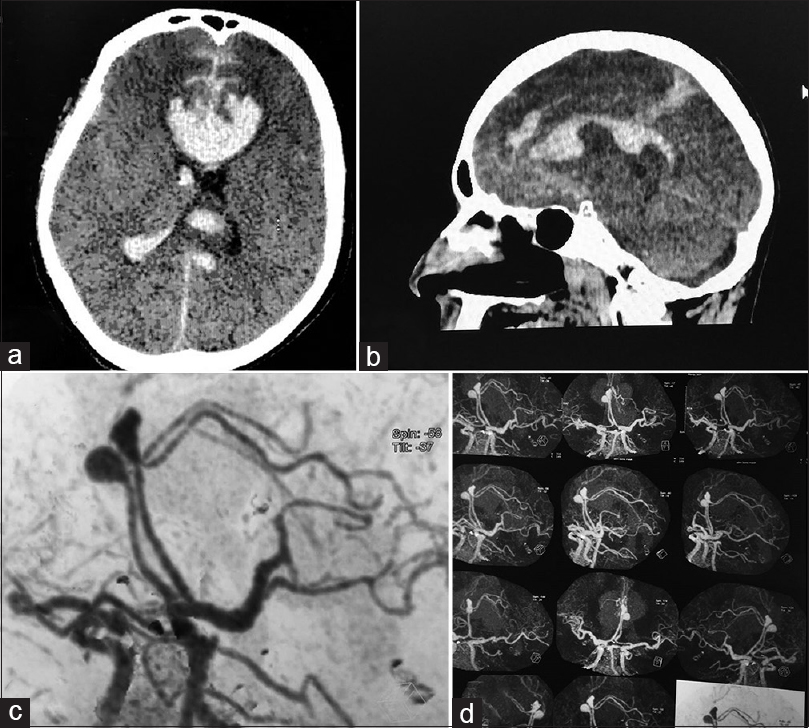
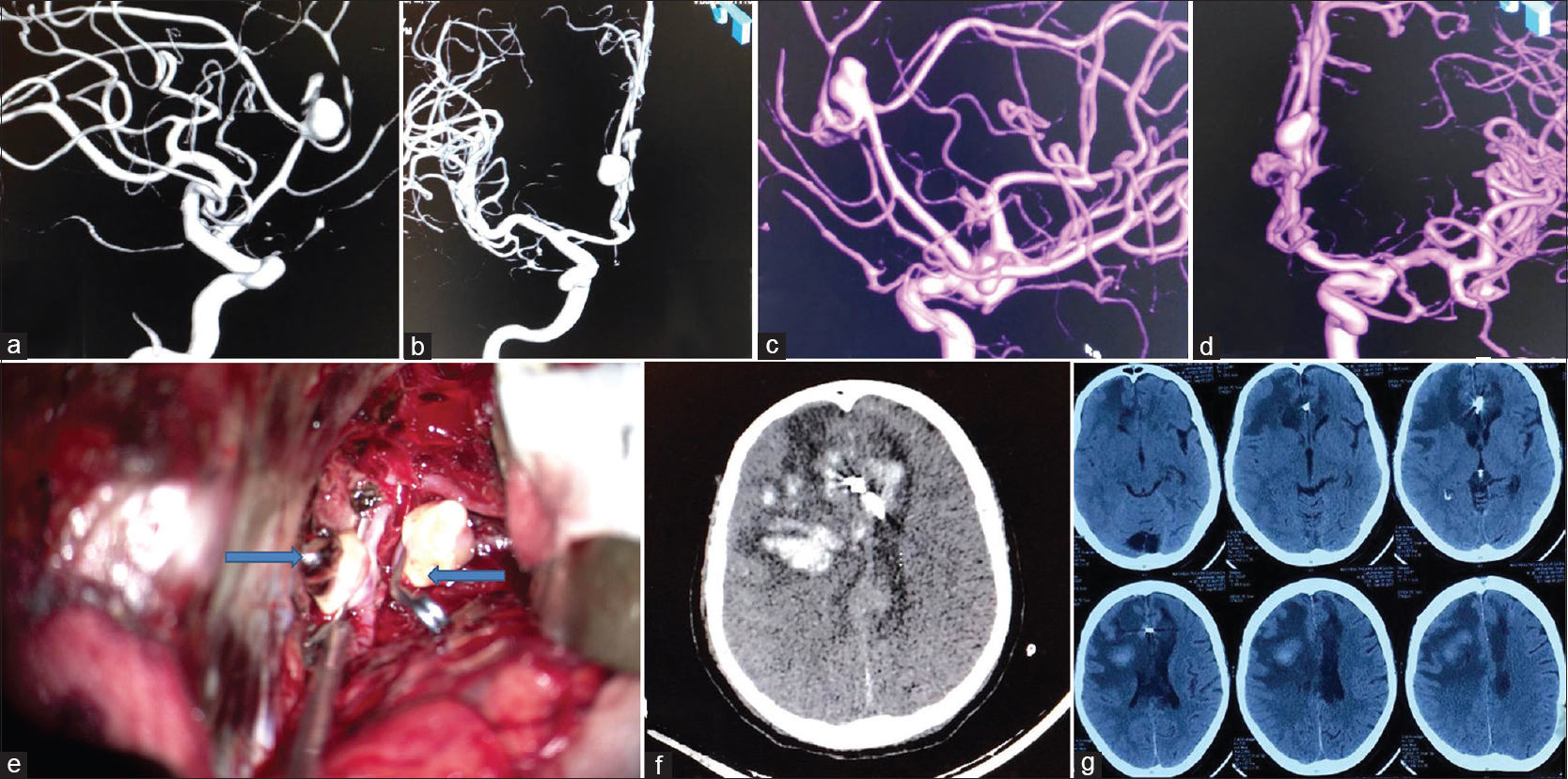
Figure 2
(a and b) DSA of the head showing right DACA aneurysm at the junction of right pericallosal and callosomarginal artery directing anterosuperiorly. (c and d) DSA of the head showing left ICA with left DACA aneurysm. (e) Intraoperative photograph showing clipped DACA aneurysms of both sides. (f) NCCT of the head on the 4th postoperative day showing right posterior frontal infarct. (g) NCCT head after 1 month showing resolving right posterior frontal infarct
The patient was operated; right frontal craniotomy was done. Interhemispheric approach was utilized. Ventricle was opened and intraventricular hematoma (IVH) was evacuated. Pericallosal and callosomarginal arteries of the left side was identified and traced proximally. Left DACA aneurysm arising from the junction of pericallosal and callosomarginal artery directing anterosuperiorly was visualized. Intraoperatively, aneurysmal ruptured site was projecting superiorly with overlying hematoma and adhesions. Moreover, majority of the hematomas were present over the left DACA aneurysm embedded in brain parenchyma. Neck dissected from the surrounding structures and both the arteries visualized with proximal ACA. Clip of size 5 mm was applied on the left side. Right-sided DACA aneurysm was identified and clipped in a similar manner [
Intraoperatively, the procedure was uneventful. There was no aneurysm rupture. There was no episode of blood pressure fluctuation. Minimal brain retraction was done. Postoperatively, the patient was electively ventilated and hypertensive therapy was given. On the 4th postoperative day, patient hemiparesis worsens. CT of the head was done, which was suggestive of right posterior frontal venous infarct and bleed [
DISCUSSION
DACA aneurysms have a very low incidence, and represent 4.4% of all cases of intracranial aneurysms.[
CT angiography, MRA, and DSA are more useful for the diagnosis of bilateral DACA aneurysms. Due to shorter acquisition time and low dose of contrast requirement compared to angiogram, CT angiogram is very useful in early planning of these types of aneurysms. CT angiogram also shows specific relation of aneurysm to bone window helping in rapid planning of craniotomy and clipping of aneurysms. MRA is also very sensitive and specific for distal aneurysm, especially measuring more than 3 mm. There is no radiation risk in MRA. Three-dimensional reconstructions are also available in this imaging.[
Clipping the aneurysm is the most definite management at the bilateral DACA region. Aneurysms at this location usually present with hematoma.[
Our case was not suitable for endovascular coiling because there was diffuse vasospasm in distal arteries. As there were two separate aneurysms located at two different arteries (also distal location), both the internal carotid arteries needs to be cannulated separately for coiling. This maneuver was going to increase the chances of dissecting injuries to both internal carotid arteries. Due to the small caliber of the parent artery, it is challenging for many endovascular microcatheters to navigate.[
CONCLUSION
Careful analysis of intracranial vasculature should be done in angiography, particularly in different views and stages to rule out multiple aneurysms at different locations in the same artery or at different arteries. Mirror images of bilateral DACA aneurysms are very rare. Fundamental surgical strategy of securing the parent artery and clipping the neck after meticulous dissection should be followed. There are high chances of rupture of other aneurysm while handling the first one as dense adhesions are present between them. Surgical maneuver should be modified in such aneurysms by careful analysis of angiography and targeting each aneurysm separately.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Albert FK, Forsting M, Benesch C, Kunze S. Pericallosal artery aneurysm originating from a “supreme anterior communicating artery”. Zentralbl Neurochir. 1999. 60: 15-9
2. Chappell ET, Moure FC, Good MC. Comparison of computed tomographic angiography with digital subtraction angiography in the diagnosis of cerebral aneurysms: A meta-analysis. Neurosurgery. 2003. 52: 624-31
3. Handa J, Suzuki F. Supreme anterior communicating artery. Neuroradiology. 1986. 28: 174-
4. Hernesniemi J, Tapaninaho A, Vapalahti M, Niskanen M, Kari A, Luukkonen M. Saccular aneurysms of the distal anterior cerebral artery and its branches. Neurosurgery. 1992. 31: 998-9
5. Kawashima M, Matsushima T, Sasaki T. Surgical strategy for distal anterior cerebral artery aneurysms: Microsurgical anatomy. J Neurosurg. 2003. 99: 517-25
6. Leheka M, Lehto H, Niemela M, Juvela S, Dashti R, Koivisto T. Distal anterior cerebral artery aneurysms: Treatment and outcome analysis of 501 patients. Neurosurgery. 2008. 60: 590-601
7. Lin N, Lanzino G, Lopes DK, Arthur AS, Ogilvy CS, Ecker RD. Treatment of Distal Anterior Circulation Aneurysms with the Pipeline Embolization Device: A US Multicenter Experience. Neurosurgery. 2016. 79: 14-22
8. Mizunari T, Muray Y, Kobayashi S, Sakai N, Teramoto A. Long-lasting narrowing of the parent artery after bilateral clipping of mirror-image aneurysms of distal anterior cerebral arteries: A case report. J Nippon Med Sch. 2011. 78: 178-83
9. Mori T, Fujimoto M, Shimada K, Shin H, Sakakibara T, Yamaki T. Kissing aneurysms of distal anterior cerebral arteries demonstrated by magnetic resonance angiography. Surg Neurol. 1995. 43: 497-9
10. Navarro R, Chao K, Steinberg GK. Microsurgical management of distal anterior cerebral artery aneurysms: From basic to complex, a video review of four cases. Acta Neurochir. 2013. 155: 2115-9
11. Sindou M, Pelissou-Guyotat I, Mertens P, Keravel Y, Athayde AA. Pericallosal aneurysms. Surg Neurol. 1988. 30: 434-40
12. Wanifuchi H, Shimizu T, Higa T, Nakaya K. Kissing mirror image anterior communicating artery aneurysms. Neurol Med Chir (Tokyo). 2001. 41: 29-32
13. Wisoff JH, Flamm ES. Aneurysms of the distal anterior cerebral artery and associated vascular anomalies. Neurosurgery. 1987. 20: 735-41
14. Yaşargil MG, Carter LP. Saccular aneurysms of the distal anterior cerebral artery. J Neurosurg. 1974. 40: 218-23
15. Yasargil MG, Yasargil MG.editors. Distal anterior cerebral artery aneurysms (pericallosal artery aneurysms). Microneurosurgery. Stuttgart: Georg Thieme Verlag; 1984. Vol II: 224-31
16. Yoshimoto T, Uchida K, Suzuki J. Surgical treatment of distal anterior cerebral artery aneurysms. J Neurosurg. 1979. 50: 40-4

