

- Department of Neurosurgery, University Hospital of Patras, Patras, Achaia, Greece.
- Department of Radiology, University Hospital of Patras, Patras, Achaia, Greece.
- Department of Otolaryngology, University Hospital of Patras, Patras, Achaia, Greece.
Correspondence Address:
Miltiadis Georgiopoulos
Department of Neurosurgery, University Hospital of Patras, Patras, Achaia, Greece.
DOI:10.25259/SNI_808_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Miltiadis Georgiopoulos1, Dimitrios Papadakos1, Pantelis Kraniotis2, Spyridon Lygeros3, Vasilios Margaritis3, Dimitrios Karnabatidis2, Georgios Gatzounis1. Neck angioedema after anterior cervical discectomy and fusion with coexistent epiglottic cyst. 22-Dec-2020;11:459
How to cite this URL: Miltiadis Georgiopoulos1, Dimitrios Papadakos1, Pantelis Kraniotis2, Spyridon Lygeros3, Vasilios Margaritis3, Dimitrios Karnabatidis2, Georgios Gatzounis1. Neck angioedema after anterior cervical discectomy and fusion with coexistent epiglottic cyst. 22-Dec-2020;11:459. Available from: https://surgicalneurologyint.com/surgicalint-articles/10484/
Date of Submission
12-Nov-2020
Date of Acceptance
08-Dec-2020
Date of Web Publication
22-Dec-2020
Abstract
Background: We present a case and reviewed the literature regarding airway obstruction and angioedema after an anterior cervical discectomy and fusion (ACDF).
Case Description: A 60-year-old female with degenerative cervical myelopathy and a previously undiagnosed epiglottic cyst underwent a C5–C6 ACDF; notably, the anesthesiologist found an epiglottic cyst when the patient was first intubated. Two hours postoperatively, the patient acutely developed severe neck swelling with airway obstruction due to angioedema. She was immediately treated with hydrocortisone and required a tracheostomy. The edema decreased markedly in the next 12 h and by the 3rd postoperative day it resolved. Three months later, she had no residual medical sequelae.
Conclusion: Patients with epiglottic cysts who need cervical spine surgery should either first have the cyst treated or should be closely monitored postoperatively.
Keywords: Angioedema, Anterior cervical discectomy and fusion, Cervical, Epiglottic, Spine
INTRODUCTION
Postoperative airway obstruction (PAO, partial or complete) after anterior cervical spine surgery (ACSS) occurs in 1.2–6.1% of patients and in up to 14% of cases following multilevel ACSS.[
Epiglottic cysts (ECs) are usually asymptomatic lesions caused by mucus retention, appearing mostly in 60-year-old patients.[
MATERIALS AND METHODS
History and examination
A 60-year-old female presented with a 1-year history of progressive myelopathy attributed to a C5–C6 MR-documented cervical stenosis with cord compression. The modified Japanese Orthopedic Association (mJOA) score was 14. At surgery, during intubation, the anesthesiologist noticed an EC cyst on the lingual surface of the epiglottis. A C5–C6 ACDF was routinely completed utilizing polymethylmethacrylate-based bone cement (Palamed G, Heraeus Medical Ltd., Wehrheim, Germany) containing gentamicin, as a cage was not available at the time. There were no intraoperative surgical or anesthetic complications.
RESULTS
Postoperative course
One hour postoperatively, the patient received one dose of parecoxib (40 mg, Dynastat, Pfizer Ltd., Kent, UK) and one dose of hydrocortisone (100 mg, Solu-Cortef, Pfizer Hellas, Athens, Greece) intravenously (e.g., to prevent edema, due to surgical manipulations with the newly diagnosed EC). Nonetheless, at 2 h postoperatively, she developed severe swelling of the whole right side of the neck/lower face along with difficulty breathing and swallowing. She immediately received 500 mg of intravenous hydrocortisone, while the otolaryngologists performed a fiber-optic endoscopy that showed acute swelling of the EC and edema of the hypopharynx/larynx.
The emergent computed tomography scan revealed massive edema of the right lateral neck affecting the epiglottis/ hypopharyngeal wall, resulting in severe airway compromise. To a lesser extent, it involved the rest of the larynx and oropharynx. There was no evidence of rupture of the EC [
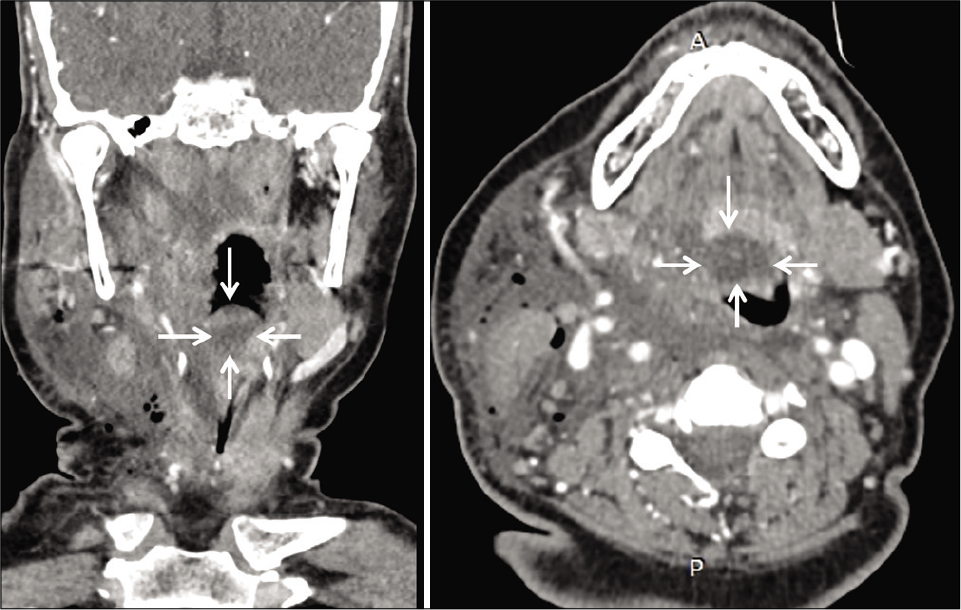
Figure 1:
Coronal multiplanar reformat (left image) and axial (right image) postcontrast computed tomography images of the neck at the level of the epiglottis. There is a cystic lesion (1.8 × 1.6 × 1 cm) centered at the tip of the epiglottis, consistent with an epiglottic cyst (arrows). The right vallecula is completely obliterated, while the left vallecula is less affected. Furthermore, there is extensive edema of the soft tissues of the right lateral neck.
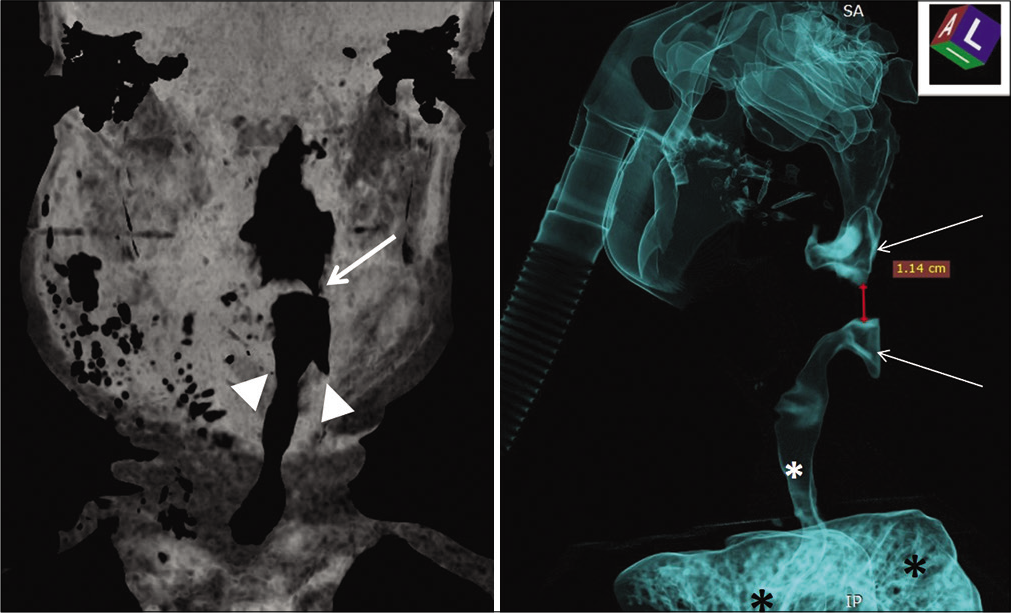
Figure 2:
Computed tomography coronal minimum intensity projection image of the neck (left image) and left lateral oblique volume-rendered image reconstructed with airway algorithm (right image). These images show the compromised airway, which measures 1.14 cm in length (depicted between the red calipers in the right image) and includes just a tiny patent part left (arrow in the left image). Furthermore, in the left image, the piriform sinus is obliterated on the right side compared to the left normal side (arrowheads). In the right image, the patent airway above and below the narrowed part are shown with white arrows, the patent trachea with a white asterisk and the lungs with black asterisks.
The anesthesiologist emergently intubated the patient, and a tracheotomy performed by the otolaryngologists. The edema decreased markedly in the next 12 h, and by the 3rd postoperative day, it resolved. Her neurologic condition improved postoperatively (mJOA score: 16), and there were no surgical/medical sequelae at 3 postoperative months [
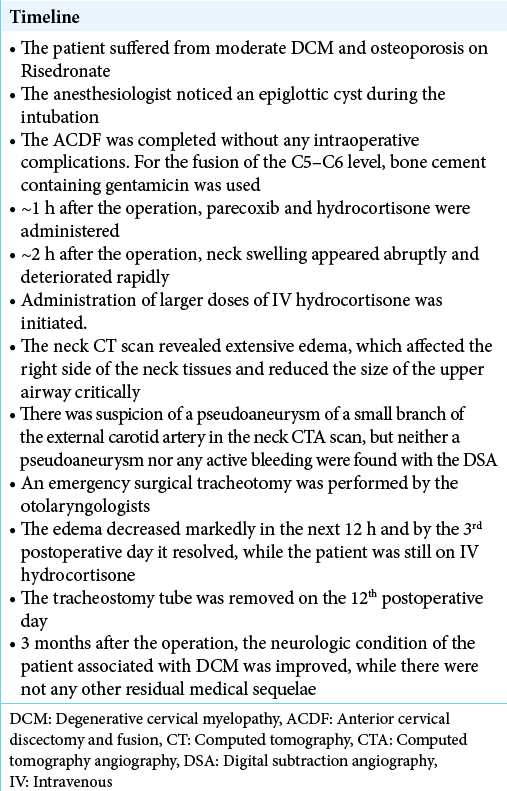
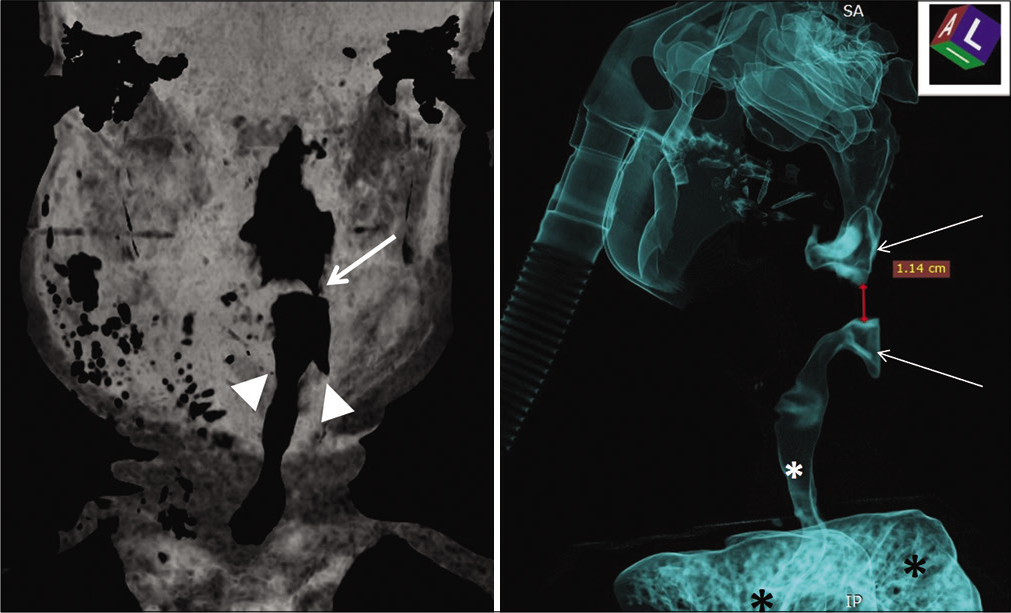
Figure 3:
Left image: axial T2 fast spin echo magnetic resonance imaging image of the neck, which shows a high signal cyst next to the right side of the base of the tongue (white arrow) corresponding to the known epiglottic cyst. Right image: endoscopic view of the epiglottic cyst (red arrow) on the lingual surface of the epiglottis.
DISCUSSION
Literature review
Although we searched the following databases: PubMed, PubMed Central, Scopus, Science Direct, Directory of Open Access Journals, and Google Scholar using multiple key words, for example, cervical, spine, neck, surgery, angioedema, epiglottic, laryngeal, and cyst (in various combinations), we were unable to find case reports/studies comparable to the one presented.
Reintubation rate after ACSS
According to the literature, reintubation after ACSS occurs in 0.1–2.4% of patients overall and in 1.6–5.2% of cases after multilevel surgery.[
Angioedema
Angioedema is one of the earliest causes of postoperative airway compromise after ACSS and typically presents within 6–12 h. However, due to its rarity, it is often misdiagnosed [
EC
ECs are usually undiagnosed because patients may not report any symptoms, but they may be potentially life threatening, requiring emergent tracheostomy.[
CONCLUSION
Patients with EC who need ACSS/ACDF neck surgery should either receive treatment of the cyst before an ACDF (e.g., if incidentally found on intubation, surgery should be cancelled and the cyst dealt with) or be closely monitored postoperatively for signs of increased airway obstruction.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Actonel (Risedronate) Dosing, Indications, Interactions, Adverse Effects and More, Medscape. Available from: https://www.reference.medscape.com/drug/actonelrisedronate-342835 [Last accessed on 2019 Nov 27].
2. Debkowska MP, Butterworth JF, Moore JE, Kang S, Appelbaum EN, Zuelzer WA. Acute post-operative airway complications following anterior cervical spine surgery and the role for cricothyrotomy. J Spine Surg. 2019. 5: 142-54
3. Dynastat 40mg Powder for Solution for Injection. Available from: https://www.medicines.org.uk/emc/product/1606/smpc [Last accessed on 2019 Nov 30].
4. Hannoodi F, Sabbagh H. ACE inhibitor-induced angioedema following cervical spine surgery. Case Rep Cardiol. 2017. 2017: 4268962
5. Kariya N, Nishi S, Minami W, Funao T, Mori M, Nishikawa K. Airway problems related to laryngeal mask airway use associated with an undiagnosed epiglottic cyst. Anaesth Intensive Care. 2004. 32: 268-70
6. Palumbo MA, Aidlen JP, Daniels AH, Bianco A, Caiati JM. Airway compromise due to laryngopharyngeal edema after anterior cervical spine surgery. J Clin Anesth. 2013. 25: 66-72
7. Sagi HC, Beutler W, Carroll E, Connolly PJ. Airway complications associated with surgery on the anterior cervical spine. Spine (Phila Pa 1976). 2002. 27: 949-53
8. Umerani MS, Alzahrani K, Mostafa GA. Hereditary angioedema: A rare presentation after anterior cervical discectomy and fusion. Asian J Neurosurg. 2015. 10: 253-5
9. Wilson LA, Zubizarreta N, Bekeris J, Poeran J, Liu J, Fiasconaro M. Risk factors for reintubation after anterior cervical discectomy and fusion surgery: Evaluation of three observational data sets. Can J Anaesth. 2020. 67: 42-56

