

- Department of Neurosurgery, Kaiser Permanente Medical Center, Los Angeles, California, USA
- Department of Neurosurgery, David Geffen School of Medicine at UCLA, Los Angeles, California, USA
Correspondence Address:
D. Diaz-Aguilar
Department of Neurosurgery, Kaiser Permanente Medical Center, Los Angeles, California, USA
DOI:10.4103/sni.sni_315_17
Copyright: © 2018 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: D. Diaz-Aguilar, T. Niu, S. Terterov, R. Scharnweber, A. Tucker, J. Woodard, H. Brara, C. Merna, H. Shah, S. Wang, S. Rahman. Neurenteric cyst of the conus medullaris. 14-Feb-2018;9:33
How to cite this URL: D. Diaz-Aguilar, T. Niu, S. Terterov, R. Scharnweber, A. Tucker, J. Woodard, H. Brara, C. Merna, H. Shah, S. Wang, S. Rahman. Neurenteric cyst of the conus medullaris. 14-Feb-2018;9:33. Available from: http://surgicalneurologyint.com/surgicalint-articles/neurenteric-cyst-of-the-conus-medullaris/
Date of Submission
27-Aug-2017
Date of Acceptance
19-Sep-2017
Date of Web Publication
14-Feb-2018
Abstract
Background:Neurenteric cysts (NECs) are rare developmental malformations of the central nervous system (CNS) which originate as benign congenital lesions. They originate from developmental foregut precursors, and are presumed to be the result of abnormal partitioning of the embryonic notochord plate. Such NECs predominantly arise in the cervical region in patients around 6 years of age or in their twenties or thirties. Notably, NECs of the conus medullaris are exceedingly rare, especially in patients of advanced age.
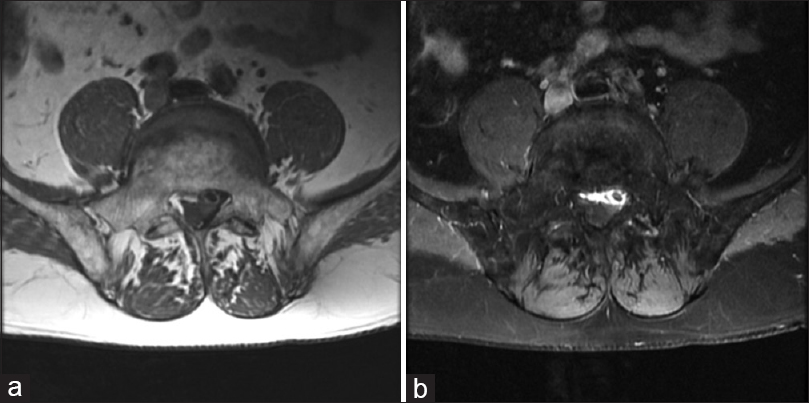
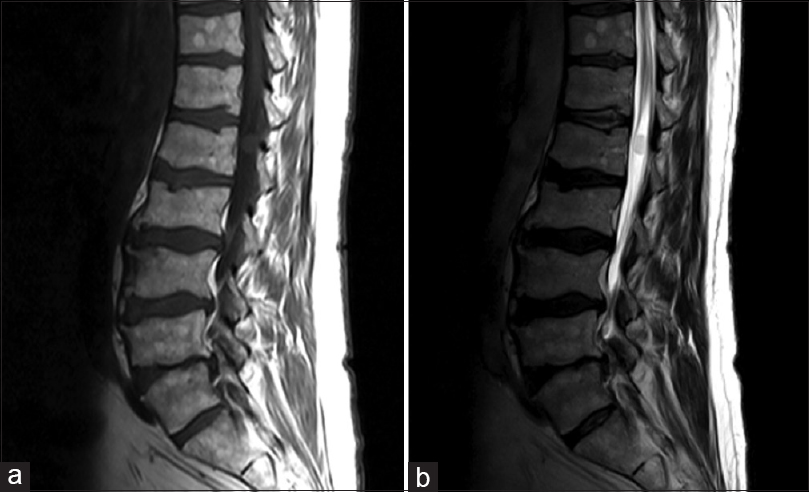
Case Description:A 70-year-old male presented with bilateral upper thigh and leg pain of over 20 years duration. His pain worsened over the past 3 years, and he sought surgical management. Although his neurological exam was normal, the lumbar magnetic resonance imaging revealed an intradural, nonenhancing, thin-walled, cystic lesion at L1/conus medullaris. The lesion was successfully resected without any adverse sequelae.
Conclusions:NECs are rare congenital legions that involve the spine. Here, an L1 intradural extramedullay neuroenteric cyst of the conus medullaris was resected without complications.
Keywords: Conus medullaris, neurenteric cysts, spinal cord tumor
INTRODUCTION
Neurenteric cysts (NECs), known as enterogenous cysts or endodermal cysts, are rare developmental malformations of the central nervous system. As benign congenital lesions of foregut origin, NECs result from abnormal partitioning of the embryonic notochord plate and endoderm.[
Frequency
NECs represent 0.3–1.3% of all spinal cord tumors. They occur more frequently in males (66–73%), and are found most commonly in patients around 6 years of age or in those in their twenties or thirties.[
Localization
NECs predominantly occur in the lower cervical or cervicothoracic regions; 90% are intradural/extramedullary (IDEM), but 10% are either extradural or intramedullary. Here, we describe a very rare lumbar NEC (IDEM) involving the conus medullaris/L1 level in a 70-year-old male.
CASE REPORT
History, physical, and diagnostic work-up
A 70-year-old male presented with bilateral upper thigh pain of 20 years duration that progressed over the last 3 years. Although neurologically intact, the MRI documented an L1/conus medullaris intradural, nonenhancing, thin-walled, cystic lesion resulting in significant cauda equina compression. He underwent an L1–L2 laminectomy with intradural resection of two lesions that were adherent to the conus. Following careful resection/dissection, he remained neurologically intact, and was still asymptomatic 1 year later [Figures
DISCUSSION
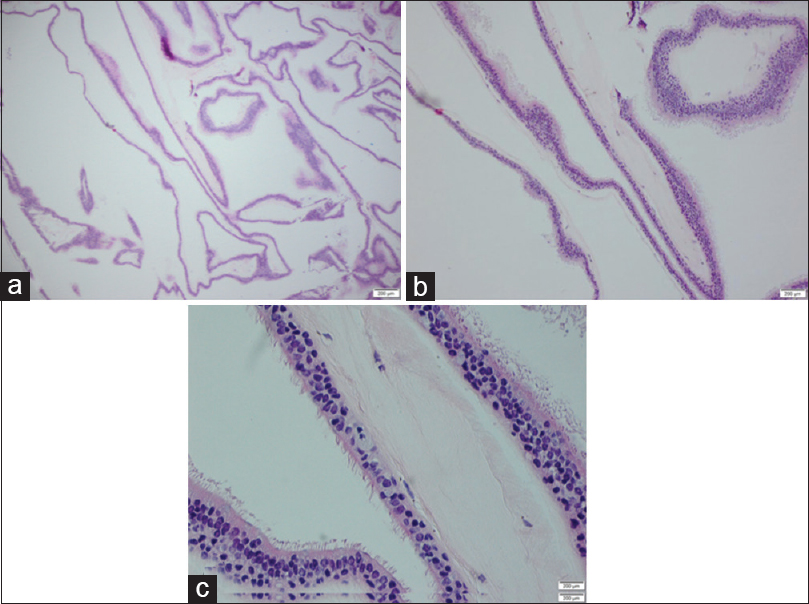
NECs typically occur in the cervical/cervicothoracic spine. Pathologically, they are lined by mucin secreting cuboidal or columnar epithelium of the intestinal or respiratory type. More than half of spinal NECs are associated with vertebral anomalies.[
CONCLUSION
NECs are rare, congenital lesions of endodermal origin that most commonly occur in the cervical or cervicothoracic regions. Only rarely do they involve the conus medullaris where they are typically extradural/intramedullary in location. Here, a 70-year-old male presented with an IDEM NEC at the L1 level compressing the conus medullaris, which was successfully resected without complications.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that name and initial will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Chakraborty S, Priamo F, Loven T, Li J, Insinga S, Schulder M. Supratentorial Neurenteric Cysts: Case Series and Review of Pathology, Imaging, and Clinical Management. World Neurosurg. 2016. 85: 143-52
2. Sadeghi-Hariri B, Khalatbari MR, Hassani H, Taheri B, Abbassioun K. Intramedullary neurenteric cyst of the conus medullaris without associated spinal malformation: A case report and review of the literature. Turk Neurosurg. 2012. 22: 478-82
3. Savage JJ, Casey JN, Mcneill IT, Sherman JH. Neurenteric cysts of the spine. J Craniovertebr Junction Spine. 2010. 1: 58-63
4. Yang T, Wu L, Fang J, Yang C, Deng X, Xu Y. Clinical presentation and surgical outcomes of intramedullary neurenteric cysts. J Neurosurg Spine. 2015. 23: 99-110
5. Yunoki M, Hirashita K, Gohda Y, Yoshino K, Fujimoto S, Mizobuchi K. True Intraspinal Neurenteric Cyst in the Lumbosacral Region-Case Report. Neurol Med Chir (Tokyo). 2007. 47: 237-9

