

- Department of Neurosurgery and Surgery, Aga Khan University, Karachi, Pakistan
- Medical College, Aga Khan University, Karachi, Pakistan
- Department of Histopathology, Aga Khan University, Karachi, Pakistan
- Department of Surgery, Section of Neurosurgery, Aga Khan University, Karachi, Pakistan
Correspondence Address:
Abdul Malik Amir Humza Sohail
Department of Surgery, Section of Neurosurgery, Aga Khan University, Karachi, Pakistan
DOI:10.4103/2152-7806.166771
Copyright: © 2015 Kalimullah J. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.How to cite this article: Kalimullah J, Humza Sohail AM A, Shahjehan RD, Siddique S, Bari ME. Neurofibromatosis type 2 patient presenting with medulloblastoma. Surg Neurol Int 07-Oct-2015;6:
How to cite this URL: Kalimullah J, Humza Sohail AM A, Shahjehan RD, Siddique S, Bari ME. Neurofibromatosis type 2 patient presenting with medulloblastoma. Surg Neurol Int 07-Oct-2015;6:. Available from: http://surgicalneurologyint.com/surgicalint_articles/neurofibromatosis-type-2-patient-presenting-with/
Abstract
Background:Neurofibromatosis type 2 (NF2) is an autosomal dominant syndrome with a frequency of 1 in 25,000 live births and a penetrance of almost 100% by the sixth decade of life. The main tumors occurring in NF2 patients are bilateral vestibular schwannomas, other peripheral, cranial and spinal nerve schwannomas, intracranial and intraspinal meningiomas, ependymomas, and gliomas.
Case Description:We report the case of a 6-year-old boy who presented with a 1-month history of nausea and recurrent vomiting. Physical examination was positive for ataxic gait and left-sided facial nerve palsy. Family history was positive for NF2 in the patient's father and paternal uncle. Magnetic resonance imaging brain revealed a solid enhancing lesion arising from the right cerebellar cortex, which was effacing the fourth ventricles and causing hydrocephalus. Craniotomy and excision of the lesion were performed. Histopathology report confirmed the diagnosis to be desmoplastic medulloblastoma. Based on the patient's subsequent history and family history, he was diagnosed to be a case of NF2.
Conclusion:This is the first case of medulloblastoma occurring in a patient with NF2 and raises the possibility of an association between medulloblastoma and NF2.
Keywords: Association, brain neoplasm, medulloblastoma, neurofibromatosis type 2
BACKGROUND
Neurofibromatosis type 2 (NF2) is an autosomal dominant syndrome with a frequency of 1 in 25,000 live births and a penetrance of almost 100% by the sixth decade of life.[
Clinical presentation of most patients with NF2 includes hearing loss which is usually unilateral, with or without tinnitus.[
Herein, we report a case NF2 presenting with recurrent vomiting and headache that was diagnosed with medulloblastoma. This, to the best of our knowledge, is the first case of medulloblastoma occurring in an NF2 patient.
CASE REPORT
A 6-year-old boy of average height and weight presented to the ER in 2003 with complaints of repeated vomiting and headache for 1-month. He was a student of a local public school, his past medical history being unremarkable; his immunization status was complete, and there were no known allergies. In family history, the patient's father and uncle (father's brother) were known to have NF2. On physical examination, he was vitally stable. Positive findings included left-sided facial nerve palsy and ataxic gait.
After a series of initial investigations, magnetic resonance imaging (MRI) brain was done. The report described a solid mass arising from the right cerebellar cortex, which was isointense to the gray matter on T1-weighted images and hypo to isointense to the gray matter on T2-weighted images. Postcontrast images showed an intense enhancement, which was almost homogenous. The mass was causing effacement of the fourth ventricles with dilatation of the third and lateral ventricles. The vertical height of the lesion was 4.2 cm; AP dimension was 4 cm, and the transverse diameter was 4.8 cm. There was no evidence of intracranial hemorrhage. Gray and white matter signals of supratentorial brain were within normal limits. No midline structural defect was seen. The differential diagnoses of medulloblastoma or astrocytoma were made.
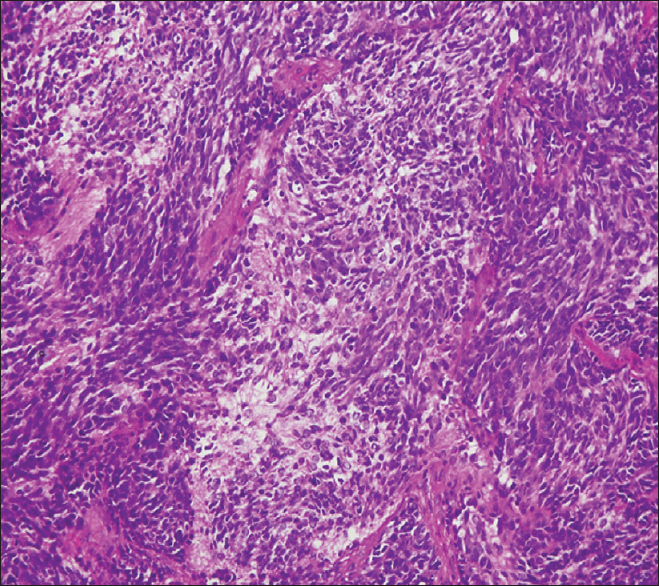
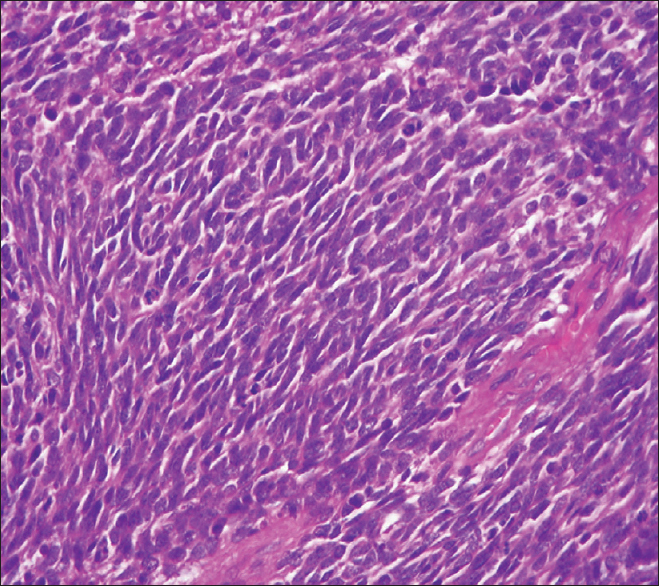
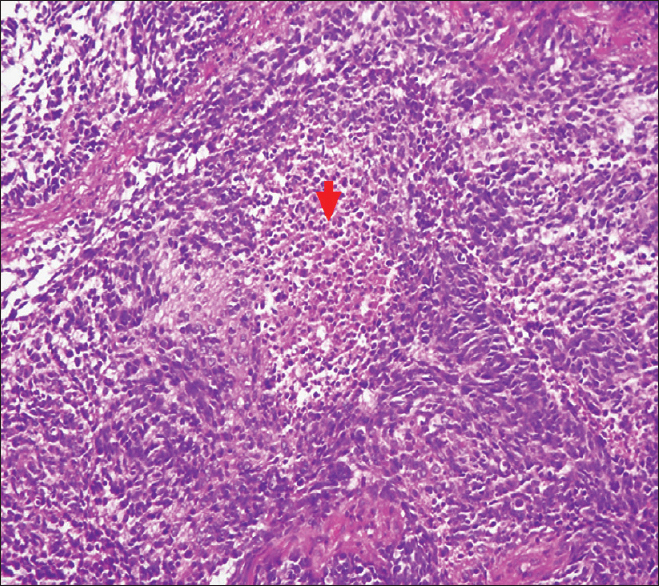
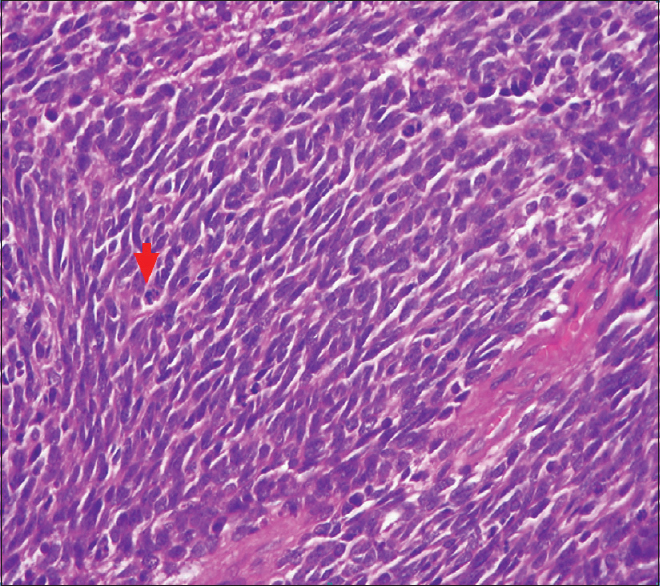
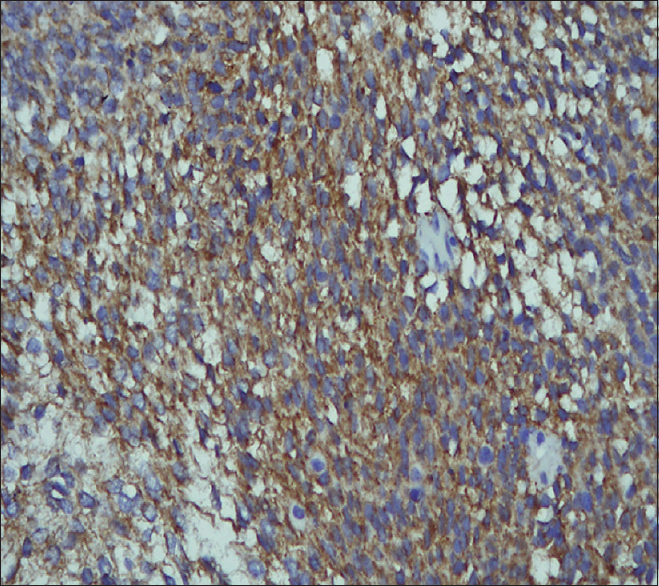
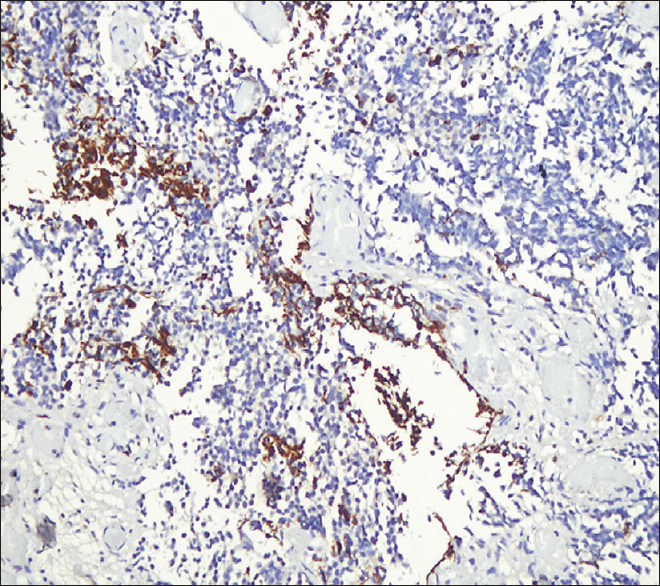
The patient underwent craniotomy and excision of the lesion with the insertion of a ventriculoperitoneal shunt. The histopathology report described a malignant infiltrating tumor present in sheets [
The patient underwent metastatic workup which was negative. After discharge, he was kept under close follow-up. Pediatric oncology team was taken on board and after discussing the case at the tumor board meeting, a multidisciplinary approach was taken and both chemotherapy and radiotherapy were administered.
In 2003, he was found to have a 1.0 cm × 1.5 cm skin colored nodule on this left forearm, which was excised with histopathology of the lesion revealing benign peripheral nerve sheath tumor.
In 2004, during a routine MRI scan the patient was found to have a cerebellar lesion for which he underwent craniotomy and excision of the lesion. Biopsy of the excised specimen revealed postchemotherapy and radiotherapy gliosis. He was then again kept under close follow-up. He complained of vision disturbances in 2006 and after an ophthalmological exam, was diagnosed to have right eye cataract for which he underwent phacoemulsification and insertion of the intraocular lens.
Till 2010, his routine follow-up MRI scans showed no significant pathological changes. However, in 2010, he again started complaining of vision disturbances and ophthalmological examination revealed right-sided posterior capsular opacification and left-sided cataract. He underwent left capsulectomy.
Over the span of next 3 years the patient remained well however, in 2013, he was again brought to Aga Khan University Hospital with complaints of headache, vomiting, and gait disturbances. MRI brain showed right superior frontal, inferior frontal, parasagittal and left posterior parietal meningiomas; excision of the lesions was performed.
Considering his case history and his family history, a diagnosis of NF2 was considered for him. A neurologist was taken on board; the NIH criterion was applied, and the patient was diagnosed to have NF2.
After the surgery in 2013, the patient has not been reported any symptoms. The follow-up MRI scans have not revealed any positive findings.
DISCUSSION
NF is a genetic disorder of the nervous system. It became widely recognized in the 19th century,[
NF is considered to have two distinct types, NF1 and NF2.[
NF2 is often a devastating autosomal dominant disorder which until recently was confused with its more common namesake NF1.[
NF2 inevitably develops schwannomas, typically affecting both the vestibular nerves, resulting in hearing loss and deafness. Most of the patients present with hearing loss which is unilateral at onset and may be accompanied or preceded by tinnitus.[
Medulloblastoma is an aggressive posterior fossa brain tumor. Although medulloblastoma has been reported in patients with NF1, one study found the prevalence of posterior fossa tumors in NF1 to be 0.83%, there is no reported case of medulloblastoma occurring in a patient with NF2.[
To the best of our knowledge, this is the first case of medulloblastoma in a patient with NF2. The literature review conducted for this report could not find any case report or research study relating medulloblastoma and NF2. This raises the possibility of an association between these two disease entities and shows that even NF2 can also have this posterior fossa brain stem tumor.
References
1. Ahn MS, Jackler RK, Lustig LR. The early history of the neurofibromatosis. Evolution of the concept of neurofibromatosis type 2. Arch Otolaryngol Head Neck Surg. 1996. 122: 1240-9
2. Asthagiri AR, Parry DM, Butman JA, Kim HJ, Tsilou ET, Zhuang Z. Neurofibromatosis type 2. Lancet. 2009. 373: 1974-86
3. Brosius S. A history of von Recklinghausen's NF1. J Hist Neurosci. 2010. 19: 333-48
4. Evans DG, Huson SM, Donnai D, Neary W, Blair V, Newton V. A clinical study of type 2 neurofibromatosis. Q J Med. 1992. 84: 603-18
5. Evans DG, Huson SM, Donnai D, Neary W, Blair V, Newton V. A genetic study of type 2 neurofibromatosis in the United Kingdom. II. Guidelines for genetic counselling. J Med Genet. 1992. 29: 847-52
6. Evans DG, Sainio M, Baser ME. Neurofibromatosis type 2. J Med Genet. 2000. 37: 897-904
7. Evans DG. Neurofibromatosis type 2 (NF2): A clinical and molecular review. Orphanet J Rare Dis. 2009. 4: 16-
8. Feucht M, Griffiths B, Niemüller I, Haase W, Richard G, Mautner VF. Neurofibromatosis 2 leads to higher incidence of strabismological and neuro-ophthalmological disorders. Acta Ophthalmol. 2008. 86: 882-6
9. Han F. Type of mutation in the neurofibromatosis type 2 gene (NF2) frequently determines severity of disease. Am J Hum Genet. 1996. 59: 331-42
10. Kanter WR, Eldridge R, Fabricant R, Allen JC, Koerber T. Central neurofibromatosis with bilateral acoustic neuroma: Genetic, clinical and biochemical distinctions from peripheral neurofibromatosis. Neurology. 1980. 30: 851-9
11. Mautner VF, Lindenau M, Baser ME, Hazim W, Tatagiba M, Haase W. The neuroimaging and clinical spectrum of neurofibromatosis 2. Neurosurgery. 1996. 38: 880-5
12. Parry DM, Eldridge R, Kaiser-Kupfer MI, Bouzas EA, Pikus A, Patronas N. Neurofibromatosis 2 (NF2): Clinical characteristics of 63 affected individuals and clinical evidence for heterogeneity. Am J Med Genet. 1994. 52: 450-61
13. Pascual-Castroviejo I, Pascual-Pascual SI, Viaño J, Carceller F, Gutierrez-Molina M, Morales C. Posterior fossa tumors in children with neurofibromatosis type 1 (NF1). Childs Nerv Syst. 2010. 26: 1599-603
14. Ruggieri M. The different forms of neurofibromatosis. Childs Nerv Syst. 1999. 15: 295-308
15. Uppal S, Coatesworth AP. Neurofibromatosis type 2. Int J Clin Pract. 2003. 57: 698-703

