

- Department of Neurosurgery, Brain Research Institute, Niigata University, Niigata, Japan.
Correspondence Address:
Tomoaki Suzuki, Department of Neurosurgery, Brain Research Institute, Niigata University, Niigata, Japan.
DOI:10.25259/SNI_930_2023
Copyright: © 2024 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Tomoaki Suzuki, Hitoshi Hasegawa, Kouichirou Okamoto, Kohei Shibuya, Hidemoto Fujiwara, Makoto Oishi. Non-sinus type of transverse sinus dural arteriovenous fistulas on the arachnoid granulation of the dural sinus wall. 09-Feb-2024;15:43
How to cite this URL: Tomoaki Suzuki, Hitoshi Hasegawa, Kouichirou Okamoto, Kohei Shibuya, Hidemoto Fujiwara, Makoto Oishi. Non-sinus type of transverse sinus dural arteriovenous fistulas on the arachnoid granulation of the dural sinus wall. 09-Feb-2024;15:43. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=12732
Date of Submission
20-Nov-2023
Date of Acceptance
09-Jan-2024
Date of Web Publication
09-Feb-2024
Abstract
Background: The etiology of a non-sinus-type dural arteriovenous fistulas (DAVFs) with shunt points located on the sinus wall, previously described as on-the-wall-type DAVFs, is unknown.
Case Description: Two cases of non-sinus-type transverse sinus DAVF with a shunt point limited to the dural sinus wall, causing cortical venous reflux, were successfully treated with endovascular transarterial Onyx embolization. The Onyx cast showed multiple feeders from the occipital and middle meningeal arteries aggregated in the arachnoid granulation (AG), which dilated the draining vein.
Conclusion: Non-sinus-type DAVFs with shunt points located on the AG may be one of the presentations of an on-the-wall-type DAVF.
Keywords: Arachnoid granulation, Dural arteriovenous fistula, On-the-wall-type, Onyx transarterial embolization, Transverse sinus
INTRODUCTION
A dural arteriovenous fistula (DAVF) is a rare intracranial vascular malformation, accounting for 10–15% of all cases. During the development of DAVFs, meningeal arteries develop fistulous connections with the dural sinus or cortical veins through the enlargement of pre-existing physiological shunts or the development of de novo fistulas through neoangiogenesis.[
CASE DESCRIPTION
Case 1
A 64-year-old man with motor weakness in the right hand was admitted to our hospital. Magnetic resonance imaging revealed no lesions responsible for his symptoms; however, time-of-flight magnetic resonance angiography demonstrated venous reflux into the vein of Labbe (VOL), suggesting a TS-DAVF [
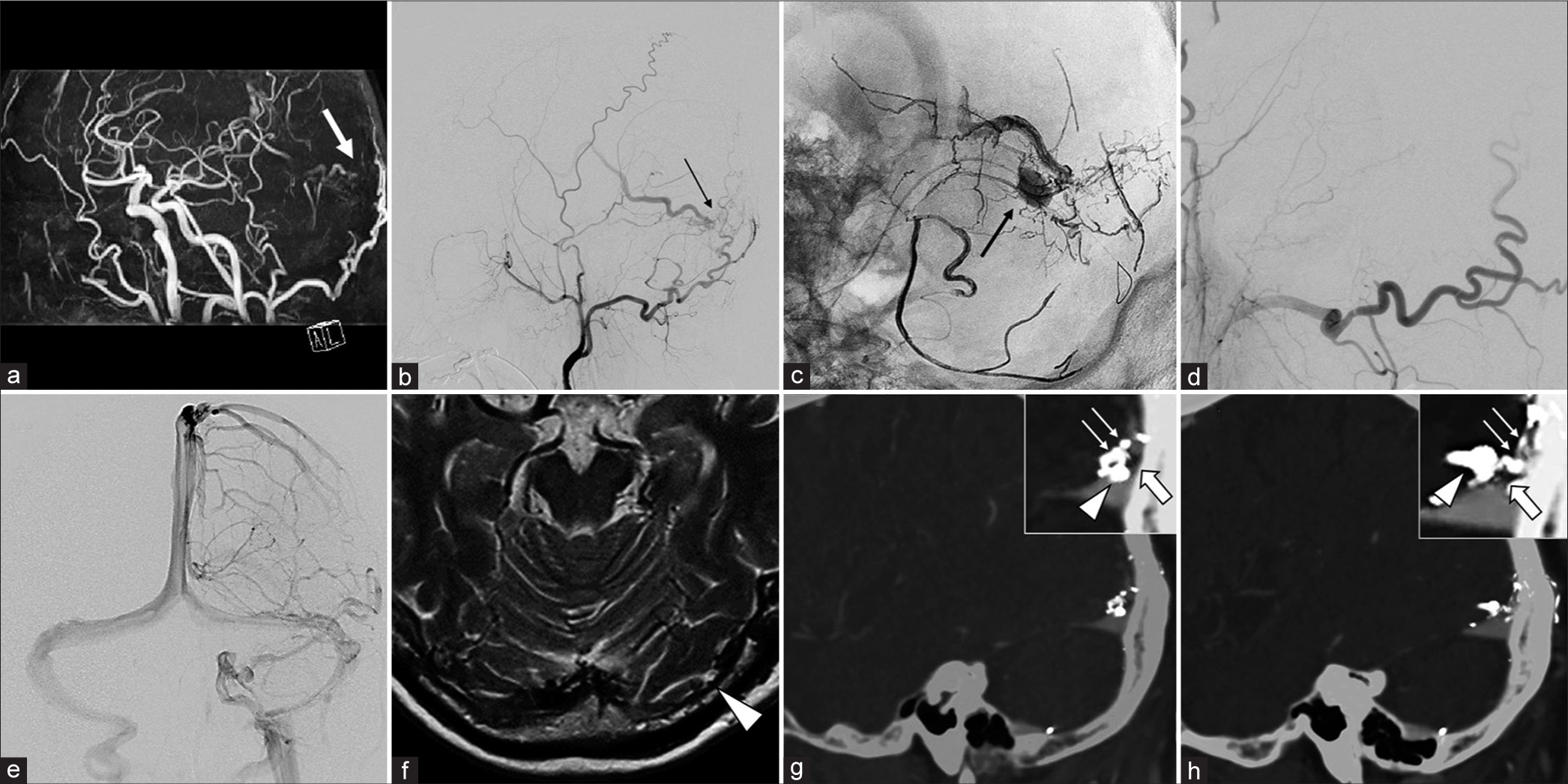
Figure 1:
(a) A time-of-flight magnetic resonance angiography image demonstrates a left transverse-sigmoid dural arteriovenous fistula (DAVF) with cortical venous reflux (white arrow). (b) Left external carotid artery angiography (lateral view) demonstrates multiple feeding arteries of a DAVF from the mastoid branches of the occipital artery (OA) and petrosquamous branches of the middle meningeal artery directly draining into the vein of Labbe (VOL) (black arrow). The shunting point was suspected to be limited to the transverse sinus (TS) wall with no venous drainage into the dural sinus. (c) Transarterial Onyx embolization was performed through the mastoid branch of the OA with a DeFrictor microcatheter (Medico’s Hirata, Osaka, Japan) and achieved successful penetration into the VOL. A SHOURYU HR (Kaneka Medics, Kanagawa, Japan) 7 × 7-mm balloon catheter was placed on standby in the TS for Onyx penetration into the sinus; however, the shunting point was completely isolated from the TS (black arrow). (d) Final view after Onyx embolization; complete occlusion of the arteriovenous shunt. (e) The venous phase of internal carotid artery angiography demonstrates that the left TS was intact. (f) Heavy T2-weighted magnetic resonance imaging before Onyx embolization demonstrates the existence of arachnoid granulation (AG) in the shunting point of the left TS (white arrowhead). (g and h) The sagittal view of postoperative digital subtraction angiography and computed tomography fusion image shows that the Onyx cast demonstrated that multiple feeders (white arrows) aggregated into the AG (white arrow) and a dilated draining vein launched from the shunt point (white arrowhead).
Video 1
Case 2
A 54-year-old man was incidentally suspected of having a TS-DAVF with cerebral cortical venous reflux on contrast-enhanced CT for examination of thyroid disease [
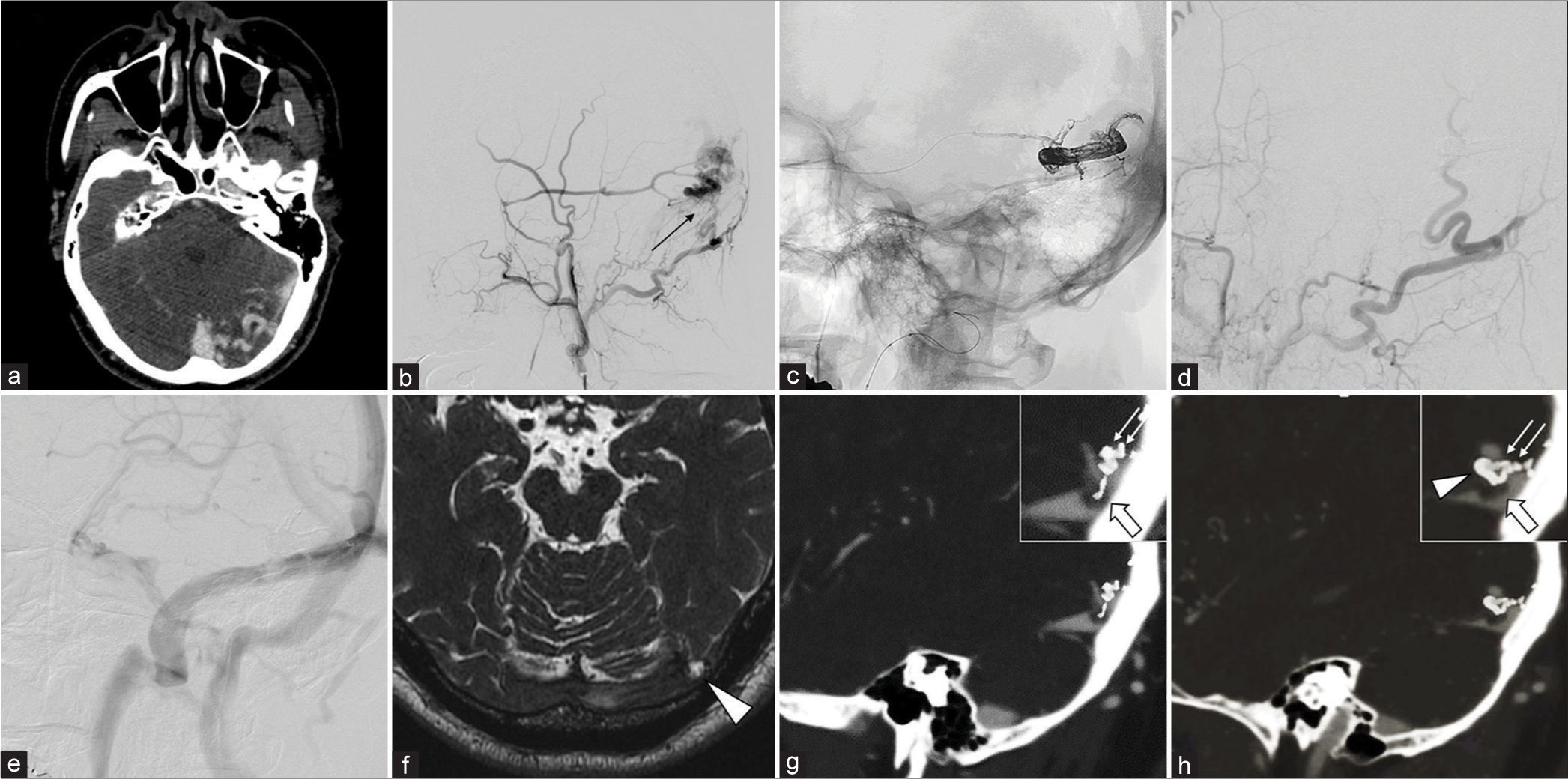
Figure 2:
(a) Contrast-enhanced computed tomography (CT) demonstrates cortical venous reflux, indicating a left transverse-sigmoid dural arteriovenous fistula (DAVF). (b) Left external carotid artery angiography (lateral view) demonstrates multiple feeding arteries of a DAVF from the petrosquamous branches of the middle meningeal artery (MMA) and transosseous branches of the occipital artery (OA) directly draining into the cortical vein. The shunting point was suspected to be limited to the transverse sinus (TS) wall with no venous drainage into the dural sinus (black arrow). (c) Transarterial Onyx embolization was performed through the petrosquamous branch of the MMA with a DeFrictor microcatheter (Medico’s Hirata, Osaka, Japan) and achieved successful penetration into the cortical vein. A Scepter C (Terumo, Tokyo, Japan) 4×10-mm balloon catheter was placed and inflated on the proximal side of the OA, with flow reduction during Onyx injection. (d) Final view after Onyx embolization; complete occlusion of the arteriovenous shunt. (e) The venous phase of internal carotid artery angiography demonstrates that left the TS was intact with no Onyx penetration. (f) Heavy T2-weighted magnetic resonance imaging before Onyx embolization demonstrates the existence of arachnoid granulation (AG) in the shunting point of the left TS (white arrowhead). (g and h) The sagittal view of postoperative digital subtraction angiography and CT fusion image shows that the Onyx cast demonstrated that multiple feeders (white arrows) aggregated into the AG (white arrow) and a dilated draining vein launched from the shunt point (white arrowhead).
Video 2
DISCUSSION
Two cases of non-sinus-type TS-DAVF with the shunt point limited to the dural sinus wall causing cortical venous reflux were successfully treated with endovascular transarterial Onyx embolization. Interestingly, post-Onyx-embolization images showed that the Onyx cast could clearly trace the feeding arteries to the draining veins, including the shunt point on the AG outside the TS [
Transarterial Onyx embolization has recently become widely recognized in the treatment of DAVFs.[
CONCLUSION
A non-sinus-type DAVF with shunt points located on the AG may be one of the presentations of an on-the-wall-type DAVF.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Videos available on
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Barnwell SL, Halbach VV, Dowd CF. A variant of arteriovenous fistulas within the wall of dural sinuses. Results of combined surgical and endovascular therapy. J Neurosurg. 1991. 74: 199-204
2. Bavinzski G, Schoeggl A, Gruber A, Killer M. Variant arteriovenous fistula of the superior sagittal sinus-case report. Neurol Med Chir (Tokyo). 1999. 39: 362-6
3. Gailloud P, Muster M, Khaw N, Martin JB, Murphy KJ, Fasel JH. Anatomic relationship between arachnoid granulations in the transverse sinus and the termination of the vein of Labbé: An angiographic study. Neuroradiology. 2001. 43: 139-43
4. Ito H, Kuwayama N, Masataka K, Okamoto S, Yamamoto H, Endo S. A case of a unique Dural arteriovenous fistula on the wall of the sinus. Surg Cereb Stroke. 2011. 39: 432-6 [In Japanese]
5. Karegowda LH, Rajagopal K, Krishnamurthy SK, Lakshmana S. Giant arachnoid granulation with a thrombosed dural arteriovenous fistula. BMJ Case Rep. 2018. 2018: bcr2018224851
6. Reynolds MR, Lanzino G, Zipfel GJ. Intracranial dural arteriovenous fistulae. Stroke. 2017. 48: 1424-31
7. Torok CM, Nogueira RG, Yoo AJ, Leslie-Mazwi TM, Hirsch JA, Stapleton CJ. Transarterial venous sinus occlusion of dural arteriovenous fistulas using ONYX. Interv Neuroradiol. 2016. 22: 711-6
8. Uchida K, Hokaku H, Aoyagi C, Takuma Y, Furudate R, Hirota N. Dural arteriovenous fistula on the wall of the superior sagittal sinus treated with transarterial embolization with onyx: A case report. J Neuroendovasc Ther. 2019. 13: 336-41
9. Yağmurlu K, Sokolowski J, Soldozy S, Norat P, Çırak M, Tvrdik P. A subset of arachnoid granulations in humans drain to the venous circulation via intradural lymphatic vascular channels. J Neurosurg. 2022. 136: 917-26

