

- Department of Neurosurgery, Albert Einstein College of Medicine of Yeshiva University and Montefiore Medical Center, Bronx, New York, USA
Correspondence Address:
Arundhati Biswas
Department of Neurosurgery, Albert Einstein College of Medicine of Yeshiva University and Montefiore Medical Center, Bronx, New York, USA
DOI:10.4103/2152-7806.196380
Copyright: © 2016 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: David Altschul, Arundhati Biswas, Jonathan Nakhla, Murray Echt, David Gordon. Novel double catheter technique with detachable microcatheter for the treatment of arteriovenous malformations: A technical note. 21-Dec-2016;7:
How to cite this URL: David Altschul, Arundhati Biswas, Jonathan Nakhla, Murray Echt, David Gordon. Novel double catheter technique with detachable microcatheter for the treatment of arteriovenous malformations: A technical note. 21-Dec-2016;7:. Available from: http://surgicalneurologyint.com/surgicalint_articles/novel-double-catheter-technique-with-detachable-microcatheter-for-the-treatment-of-arteriovenous-malformations-a-technical-note/
Date of Submission
12-Apr-2016
Date of Acceptance
05-Jul-2016
Date of Web Publication
21-Dec-2016
Abstract
Background:Onyx has improved the safety and efficacy of endovascular treatment in the management of cerebral arteriovenous malformations (AVMs). However, during injection inadvertent reflux around the delivery microcatheter into important normal arterial branches remains a major challenge.
Methods:We describe a new double arterial catheterization technique using a detachable tip microcatheter in conjunction with a second microcatheter to form a proximal antireflux Onyx plug. This novel technique allows for increased amounts of Onyx to be steadily injected while avoiding dangerous backflow in the treatment of AVMs.
Results:The patient tolerated the procedure well without changes in hemodynamics. Using the novel double catheter technique, a significant portion of the AVM was embolized and the patient had no complications postoperatively.
Conclusions:The novel double catheter technique with a detachable microcatheter is a safe and effective technique to increase the amount of Onyx embolization material into the AVM nidus.
Keywords: Cerebral arteriovenous malformations, embolization, Endovascular treatment, Onyx
INTRODUCTION
Endovascular treatment is commonly used as an adjuvant therapy in the management of cerebral arteriovenous malformations (AVMs), either for preoperative reduction in vascularity, or pre-radiosurgical volume reduction. The widespread use of Onyx has improved the curative rates of embolization as it allows for more controlled injection over a period of time.[
ILLUSTRATIVE CASE
A 21-year-old man was admitted secondary to intracerebral hemorrhage due to rupture of a known AVM. He had an external ventriculostomy drain placed for hydrocephalus that was weaned without the need for shunting. Cerebral digital subtraction angiography (DSA) showed a right frontal Spetzler–Martin grade V AVM with supply from right middle cerebral artery (MCA) and anterior cerebral artery (ACA) feeders with superficial and deep drainage. Four sessions of Onyx embolization were performed to occlude the medial deeper portion of the AVM with intranidal aneurysm along a distal right ACA feeder. In the fifth session, a double catheterization technique was used to create an antireflux Onyx plug around the detachable part of an Apollo™ micro catheter to allow for greater penetration of the nidus [
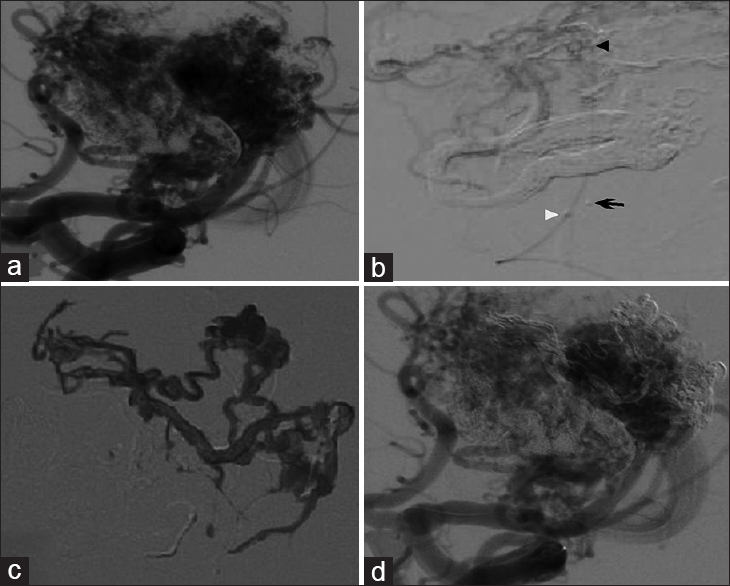
Figure 1
(a) Digital subtraction angiography prior to staged embolization with right internal carotid artery selective injection demonstrating arteriovenous malformation (AVM) (b) Double microcatheter technique with superselective injection ensuring that Onyx will not enter en-passage arteries; black arrowhead points to the detachment zone of the Echelon microcatheter with contrast injection, white arrowhead points to the coil detachment of the Echelon microcatheter, and the arrow points to the detachment tip of the Apollo microcatheter (c) Onyx within nidus of AVM after detachment of Apollo. (d) Control angiogram shows reduction in AVM opacification
Through a 6 Fr Envoy guide catheter, an Echelon-10 microcatheter was advanced over a 0.08 in microwire (Mirage, ev3) to access a distal M4 branch supplying the AVM. An Apollo™ 3 cm detachable tip microcatheter was navigated alongside the first catheter in the same feeder but more distally into the nidus. Super selective microinjection was performed through both catheters to identify the distal aspect of the target vessel supplying the nidus and identifying any en-passage vessels. The Echelon microcatheter tip was positioned between the most distal marker and the detachment zone of Apollo and preloaded with 0.34 cc of dimethyl sulfoxide DMSO. Under continuous roadmap guidance, approximately 0.4 cc of Onyx 34 was embolized into the feeding branch vessel to build an Onyx plug to prevent reflux. Once an adequate plug had been created, the Echelon catheter was removed under fluoroscopic guidance. The Apollo microcatheter was then preloaded with 0.23 cc of DMSO and 1.7 cc of Onyx 18 was embolized into the nidus of the AVM.
After embolization was confirmed by control angiogram, the Apollo tip was successfully detached and was withdrawn under fluoroscopic guidance. Flow was eliminated through a significant portion of the nidus using this technique. The patient remained hemodynamically stable throughout the procedure and no immediate complications were noted.
DISCUSSION
While the nonadhesive nature of Onyx (ev3, Irvine, California), allows for prolonged and repeated injections from the same point, resulting in deeper penetration into the larger part of the nidus. However, there is still a significant risk of reflux into vessels supplying the normal brain and early inadvertent occlusion of the draining vein, which might limit the procedure. The maximal safe reflux distance along the feeding vessel judged on the initial angiogram should usually be no more than 2 cm back or 1 cm distal to a cortical branch of the feeding artery.[
There has been recent development of Onyx-compatible double lumen balloons (HyperForm and HyperGlide [ev3] and Sceptor C and Scepter XC [MicroVention]) as a way to avoid the need for a plug and its associated risks, as well as to minimize reflux around the microcatheter by inflating proximal to the Onyx injection site, thereby minimizing the risk of catheter retention. The main limitation of this technique is the difficulty encountered while navigating the dual lumen balloon into distal arterial feeders, especially the small ones as these vessels can often be accessed only with flow-directed microcatheters.[
To overcome these limitations, we report a new technique using a second microcatheter to form an Onyx plug for creating a seal around the distally placed detachable tip. This wedge flow condition reduced the blood supply through the AVM and contrast washout during selective injections. It prevented Onyx from reflux into important vessels and allowed for more forceful and thorough embolization. After the initial embolization epoch with more viscous Onyx-34, with the plug well formed, we switched to Onyx-18, which is less viscous and penetrated the AVM more easily.[
Chapot et al.[
CONCLUSION
In conclusion, this technique has the dual benefit of potentially lowering fluoroscopy times and of increasing the amount of Onyx that can be injected in AVMs while simultaneously avoiding dangerous backflow. It might increase the curative potential of large AVMs and reduce the number of treatment sessions.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Altschul D, Paramasivam S, Ortega-Gutierrez S, Fifi JT, Berenstein A. Safety and efficacy using a detachable tip microcatheter in the embolization of pediatric arteriovenous malformations. Child's Nerv Syst. 2014. 30: 1099-107
2. Chapot R, Stracke P, Velasco A, Nordmeyer H, Heddier M, Stauder M. The Pressure Cooker Technique for the treatment of brain AVMs. J Neuroradiol. 2014. 41: 87-91
3. Peschillo S, Caporlingua A, Colonnese C, Guidetti G. Brain AVMs: An Endovascular, Surgical, and Radiosurgical Update. Scientific World Journal. 2014. 2014: 834931-
4. Potts M, Zumofen D, Raz E, Nelson P, Riina H. Curing arteriovenous malformations using embolization. Neurosurg Focus. 2014. 37: E19-
5. Sekhar LN, Biswas A, Hallam D, Kim LJ, Douglas J, Ghodke B. Neuroendovascular Management of Tumors and Vascular Malformations of the Head and Neck. Neurosurg Clin N Am. 2009. 20: 453-85

