

Occipitofrontal switch for correction of anterior plagiocephaly planned through virtual mock surgery
- Department of Burns and Plastic Surgery, All India Institute of Medical Science, Rishikesh, Uttarakhand, India.
- Department of Neurosurgery, All India Institute of Medical Science, Rishikesh, Uttarakhand, India.
Correspondence Address:
Debarati Chattopadhyay
Department of Neurosurgery, All India Institute of Medical Science, Rishikesh, Uttarakhand, India.
DOI:10.25259/SNI_757_2020
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Debarati Chattopadhyay1, Madhubari Vathulya1, Praveen Jayaprakash1, Akshay Kapoor1, Vaishali Verma1, Rajnish Arora2. Occipitofrontal switch for correction of anterior plagiocephaly planned through virtual mock surgery. 08-Apr-2021;12:148
How to cite this URL: Debarati Chattopadhyay1, Madhubari Vathulya1, Praveen Jayaprakash1, Akshay Kapoor1, Vaishali Verma1, Rajnish Arora2. Occipitofrontal switch for correction of anterior plagiocephaly planned through virtual mock surgery. 08-Apr-2021;12:148. Available from: https://surgicalneurologyint.com/surgicalint-articles/10695/
Date of Submission
23-Oct-2020
Date of Acceptance
11-Mar-2021
Date of Web Publication
08-Apr-2021
Abstract
Background: Unilateral coronal synostosis causing anterior plagiocephaly can result in restricted brain development and severe facial deformities. Various surgical procedures have been described for the correction of this deformity. Cranial vault remodeling, however, is associated with several complications. Occipitofrontal switching is a novel technique which utilizes a part of the contralateral occipital bone to reconstruct the frontal area. This is the first such case reported from India and first report where virtual mock surgery has been utilized for precision and improving outcome in this elegant procedure.
Case Description: A 5-year-old girl presented with left anterior plagiocephaly. 3D image of her skull was reconstructed using Geomagic Freeform software (3D Systems, Rock Hill, SC). Measurements were accurately drawn and the procedure was practised virtually before performing the occipitofrontal switch on the patient. There were minimal blood loss and postoperative morbidity. One year follow-up of the patient showed optimal correction of the defect in the forehead region, symmetrical shape of the frontal and occipital region and symmetrical brows.
Conclusion: The technique of occipitofrontal switch for correction of anterior plagiocephaly is an elegant procedure with good functional and aesthetic outcome.
Keywords: 3D model, Occipitofrontal switch, Plagiocephaly
INTRODUCTION
Craniosynostosis occurs due to premature fusion of one or more sutures of the cranial vault.[
This is the first such case reported from India and first report where virtual mock surgery has been utilized for precision and improving outcome with this elegant procedure.
CASE PRESENTATION
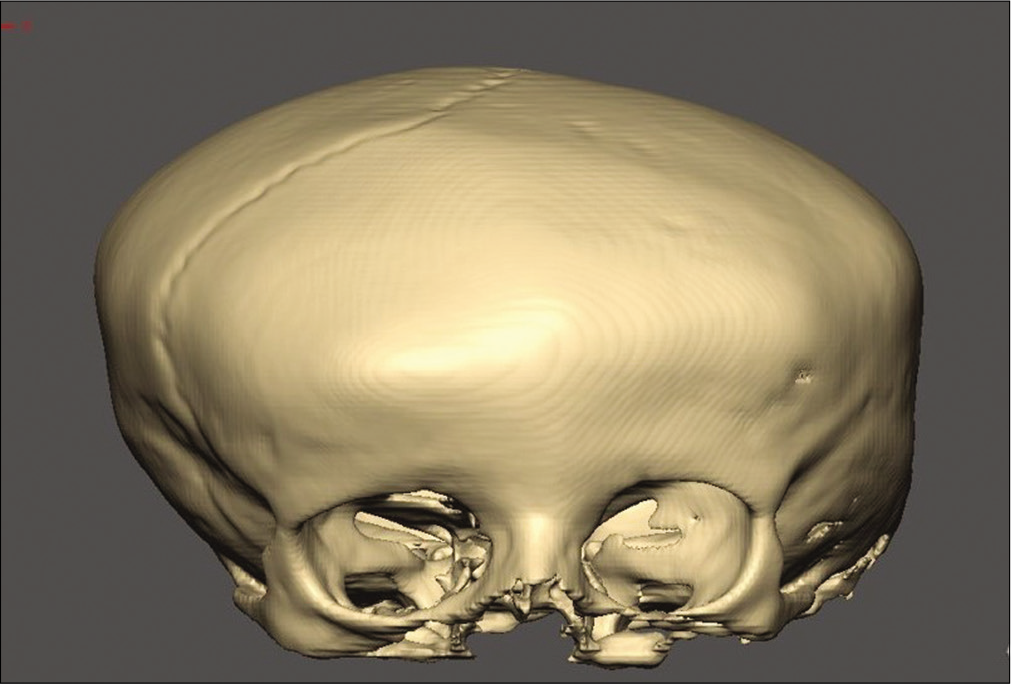
A 5-years-old female child presented to our outpatient department with facial asymmetry. On examination, she had flattening of the forehead and elevation of the eyebrow on the left side [

Preoperative planning
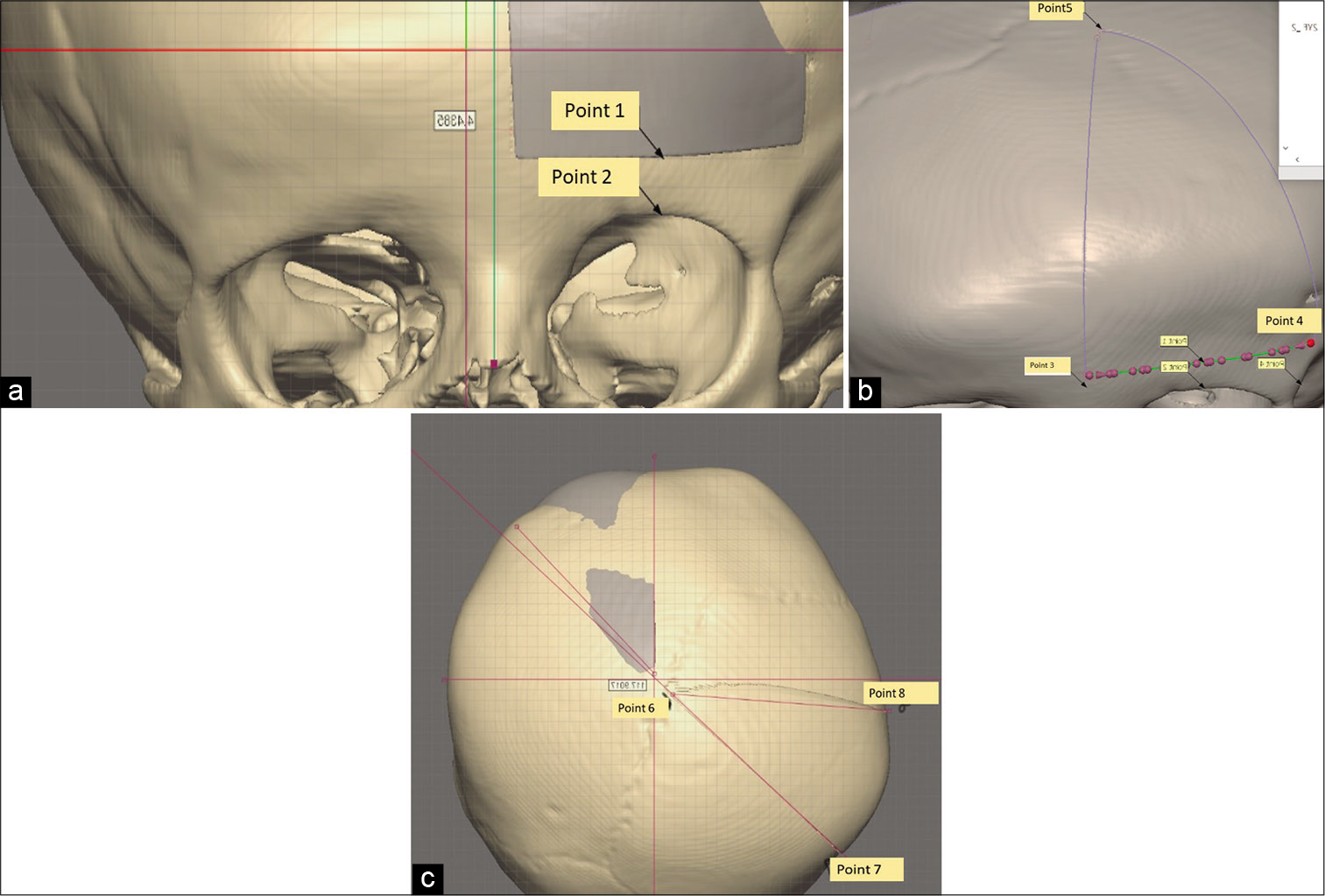
Based on the 3D computer tomography picture a virtual 3D model of the skull was made using the software INVIVO 5 and the model was imported to a virtual clay modeling design software in a haptic based environment, Freeform Geomagic. (3D Systems, Rock Hill, SC) [
Virtual planning and mock surgery was done by the following steps
First, the left fronto-orbital bar was measured preserving the supraorbital and supratrochlear nerve [
Surgery
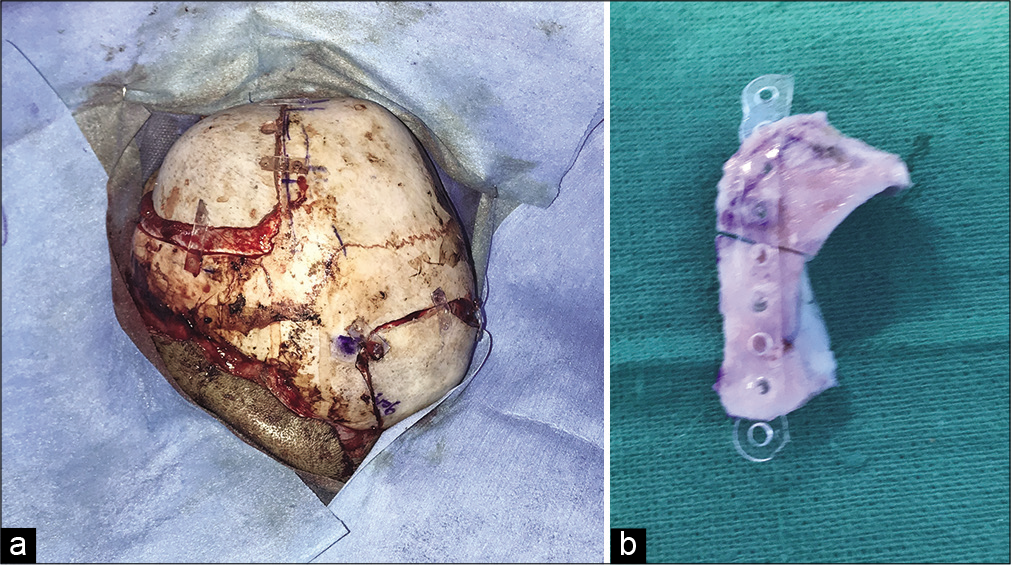
After obtaining clearance from the anaesthesia team and written informed consent from the parents, patient was taken for occipitofrontal switch under general anaesthesia. Patient was placed in the supine position. Bicoronal incision was made which provided adequate exposure to the defective left frontal bone and the planned donor area on the right side occiput. Scalp flaps were raised. The markings obtained from the virtual 3D model were applied to the skull in the defective frontal area and the donor occiput region. Occipital triangle was harvested first followed by the frontal triangle. Curved bone obtained from the hemioccipital triangle was placed over the defective frontal region and secured with biodegradable plates and screws. The flat bone obtained from the defective frontal region was placed over the occipital region and similarly secured [
RESULTS
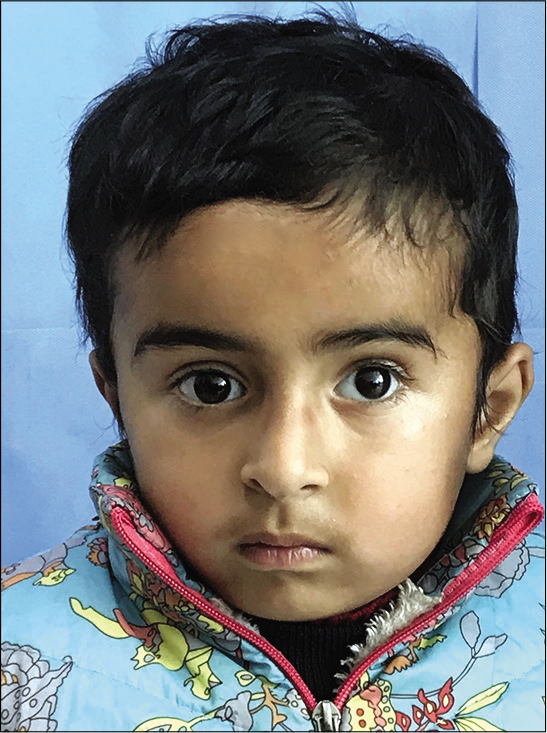
The virtual 3D model helped in accurately predicting the curvature of the diseased site and thus helped in the markings at the defective frontal and the occipital region. This reduced the margin of error. The occipital bone fragment obtained was a perfect fit for the defect in the frontal area. This also helped in reducing the operative time. Since bioabsorbable plates were used for the fixing the bony triangles there would be no growth disturbance. The patient’s parents were pleased with the outcome and cosmetic appearance. 1 year follow-up of the patient showed optimal correction of the defect in the forehead region, symmetrical shape of the frontal and occipital region and symmetrical brows [
DISCUSSION
The term plagiocephaly was coined by Virchow in 1851 based on the Greek term Plagio(slanted/oblique) to define individuals with unipartite flattening of orbit and frontal bone associated with scoliosis of face and skull. In anterior plagiocephaly, there is premature unilateral fusion of the coronal suture. The anterior cranial fossa is underdeveloped in these patients along with altered development of facial and cranial bones. This clinically manifests as flattening of orbit and frontal bone in the affected side. Skull and facial bone anomalies include homolateral advancement of the petrous bone toward the affected side, contralateral deviation of nasal pyramid and vomer, and compensatory growth of temporal bone and forehead of the opposite side.[
The goal of craniosynostosis surgery is to achieve a mesocephalic skull shape with adequate space for brain expansion.[
In unilateral plagiocephaly, the unique technique of occipitofrontal switch allows the abnormal hemifrontal bone to be replaced by contralateral hemioccipital bone.[
This unique technique has been described in only one published article.[
CT scan done 6 months postoperatively showed stable osteosynthesis. There were no complications in the postoperative period. At 1 year follow-up, the patient’s parents were very much satisfied with the cosmetic outcome. The forehead, brow, and occiput were symmetrical. Long term follow-up of the patient is to be done to look for further aesthetic changes and graft resorption.
CONCLUSION
The technique of occipitofrontal switch for correction of anterior plagiocephaly is an elegant procedure with good functional and aesthetic outcome.
Statement of ethics
Written informed consent was obtained from the patient’s parents (father and mother) for publication of this case report and any accompanying images.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
None.
References
1. Cohen SR, Frank RC, Meltzer HS, Levy ML, James ZE, Gordon CR.editors. Craniosynostosis. Handbook of Craniomaxillofacial Surgery. Singapore: World Scientific Publishing Company; 2014. p. 343-68
2. Delashaw BJ, Persing JA, Broaddus CW, Jane JA. Cranial vault growth in craniosynostosis. J Neurosurg. 1989. 70: 159-65
3. Di Rocco C, Paternoster G, Caldarelli M, Massimi L, Tamburrini G. Anterior plagiocephaly: Epidemiology, clinical findings, diagnosis, and classification. A review. Childs Nerv Syst. 2012. 28: 1413-22
4. Esparza J, Hinojosa J, García-Recuero I, Romance A, Pascual B, Martínez de Aragón A. Surgical treatment of isolated and syndromic craniosynostosis. Results and complications in 283 consecutive cases. Neurocirugia (Astur). 2008. 19: 509-29
5. Hassanpour SE, Abbasnezhad M, Otaghvar HA, Tizmaghz A. Surgical correction of unicoronal craniosynostosis with frontal bone symmetrization and staggered osteotomies. Plast Surg Int. 2018. 2018: 3793592
6. Kim PC, Kim YD, Park DH. Occipitofrontal switching for simultaneous correction of synostotic frontal and occipital plagiocephaly: A novel surgical technique. Craniomaxillofac Trauma Reconstr. 2010. 3: 161-6
7. Lane LC. Pioneer craniectomy for relief of mental imbecility due to premature sutural closure and microcephalus. JAMA. 1892. 18: 49-50
8. Muñoz-Casado MJ, Romance AI, García-Recuero JI. Bioabsorbable osteofixation devices in craniosynostosis. Clinical experience in 216 cases. Neurocirugia (Astur). 2009. 20: 255-61
9. Persing JA, Edgerton MT, Park TS, Jane JA.editors. Barrel stave osteotomy for correction of turribrachycephaly craniosynostosis deformity. Craniofacial Surgery. Berlin, Heidelberg: Springer; 1987. p. 145-50
10. Posnick JC. Upper facial asymmetries resulting from unilateral coronal synostosis. Diagnosis and surgical reconstruction. Atlas Oral Maxillofac Surg Clin North Am. 1996. 4: 53-66
11. Silav G, Avci G, Akan M, Taylan G, Elmaci I, Akoz T. The surgical treatment of plagiocephaly. Turk Neurosurg. 2011. 21: 304-14
12. Tessier P. Total facial osteotomy. Crouzon’s syndrome Apert’s syndrome: Oxycephaly, scaphocephaly, turricephaly. Ann Chir Plast. 1967. 12: 273-12
13. Warren SM, Proctor MR, Bartlett SP, Blount JP, Buchman SR, Burnett W. Parameters of care for craniosynostosis: Craniofacial and neurologic surgery perspectives. Plastic Reconstr Surg. 2012. 129: 731-7

