

- Department of Neurosurgery, Akita Red Cross Hospital, Akita, Japan
- Department of Neurosurgery, Brain Research Institute, University of Niigata, Niigata, Japan
Correspondence Address:
Jun Watanabe
Department of Neurosurgery, Brain Research Institute, University of Niigata, Niigata, Japan
DOI:10.4103/2152-7806.183518
Copyright: © 2016 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Watanabe J, Maruya J, Nishimaki K, Ito Y. Onyx removal after embolization of a superior sagittal sinus dural arteriovenous fistula involving scalp artery. Surg Neurol Int 03-Jun-2016;7:
How to cite this URL: Watanabe J, Maruya J, Nishimaki K, Ito Y. Onyx removal after embolization of a superior sagittal sinus dural arteriovenous fistula involving scalp artery. Surg Neurol Int 03-Jun-2016;7:. Available from: http://surgicalneurologyint.com/surgicalint_articles/onyx-removal-after-embolization-of-a-superior-sagittal-sinus-dural-arteriovenous-fistula-involving-scalp-artery/
Abstract
Background:Most dural arteriovenous fistula (DAVF) in superior sagittal sinus (SSS) requires multimodal treatment. Onyx embolization is useful for DAVF; however, scalp artery embolization has cast extrusion risk.
Case Description:A 59-year-old male presented with involuntary movements of both legs and progressive dementia. Cerebral angiography demonstrated the DAVF in the SSS fed by bilateral superficial temporal, occipital, and middle meningeal arteries. The posterior SSS was thrombosed, and the main drainers were cortical veins. Combined treatment with transarterial embolization using Onyx and transvenous embolization using coils was performed. Although symptoms were improved, a small DAVF remained. Two months later, Onyx cast extrusion through the scalp was observed, requiring removal and debridement because of infection at the extrusion sites. Surgery for the residual DAVF would be difficult because of scalp condition; therefore, an additional endovascular treatment was conducted, completely occluding DAVF.
Conclusion:Onyx embolization is useful for DAVF; however, scalp artery embolization has cast extrusion risk. Therefore, scalp infection should be considered because it may preclude additional surgical procedures.
Keywords: Complication, dural arteriovenous fistula, Onyx, scalp artery, superior sagittal sinus
INTRODUCTION
Currently, transarterial embolization (TAE) with the liquid embolic Onyx is used for the treatment of the superior sagittal sinus (SSS) dural arteriovenous fistulas (DAVFs).[
CASE HISTORY
A 59-year-old male presented with involuntary movements of both legs and progressive dementia. Magnetic resonance imaging and cerebral angiography revealed SSS-DAVF with occlusion of the posterior one-third of SSS. This SSS-DAVF was fed by bilateral occipital arteries (OAs), superficial temporal arteries (STAs), thin middle meningeal arteries (MMAs), and meningeal branches of the vertebral artery. Anterograde drainage was not observed through SSS, whereas drainage routes through dilated medullary and cortical veins (CV) were identified. Iodine-123-N-isopropyl-p-iodoamphetamine single-photon emission computed tomography revealed hypoperfusion of the vertex sides [Figures
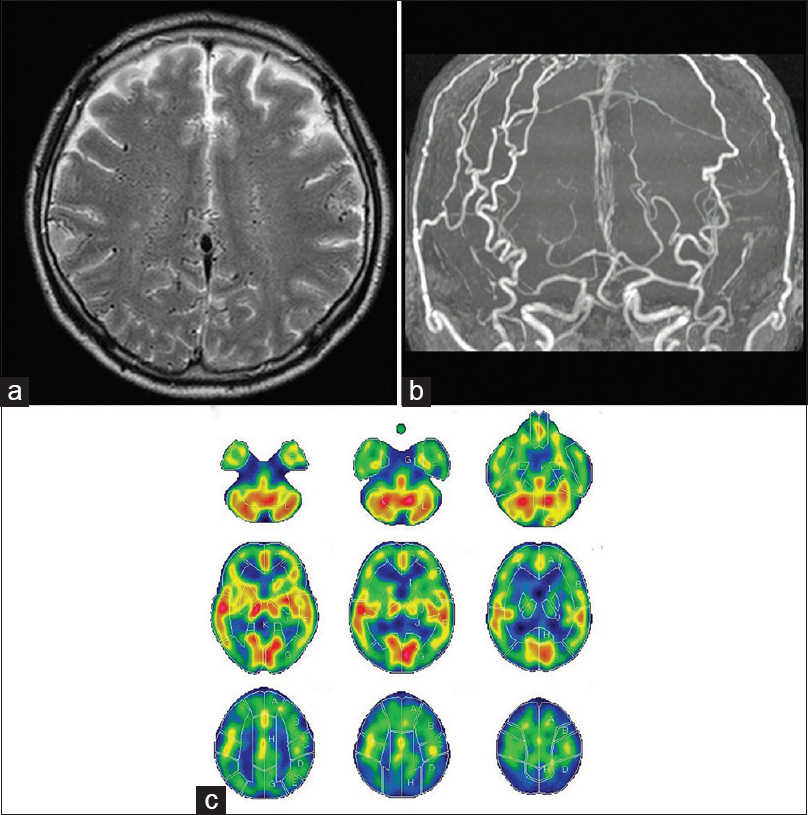
Figure 1
(a) Preoperative T2-weighted magnetic resonance image revealing multiple aberrant medullary veins. (b) Magnetic resonance angiography revealing expanded bilateral occipital arteries and superficial. (c) Iodine-123-N-isopropyl-p-iodoamphetamine single-photon emission computed tomography revealing hypoperfusion of bilateral vertex sides of the frontal, parietal, and occipital lobules
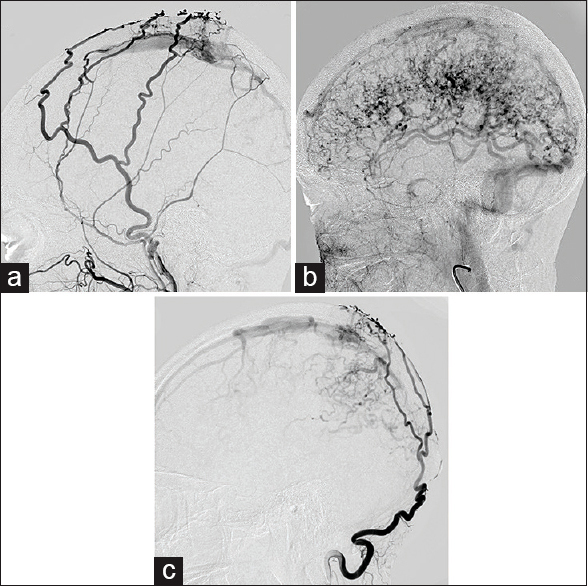
Figure 2
Angiographic images (lateral view). (a) Preoperative right external carotid angiography showing a dural arteriovenous fistula in the superior sagittal sinus fed by the right superficial temporal artery and thin middle meningeal artery. (b) Preoperative right external carotid angiography in the venous phase showing occlusion of the posterior one-third of superior sagittal sinus. The dural arteriovenous fistula is drained via anterograde flow by cortical and medullary veins into the vein of Labbe or deep venous system and subsequently into the vein of Galen. (c) Preoperative right occipital artery angiography showing the dural arteriovenous fistula fed by occipital artery
First embolization
Right femoral artery puncture was performed under general anesthesia. A microcatheter (Marathon; eV3 Neurovascular, Irvine, CA, USA) was navigated to the distal left OA for Onyx-18 injection, causing incomplete DAVF obliteration. Onyx embolization was performed through the left STA, resulting in a partial reduction in blood flow from the left feeding arteries [
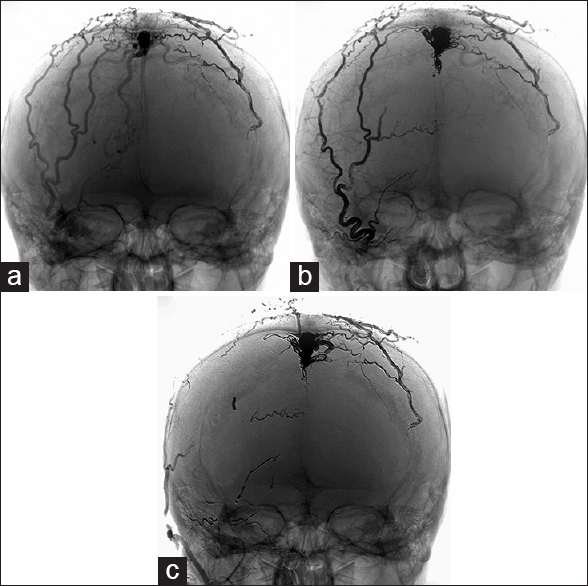
Figure 3
Angiographic images (anteroposterior view). (a) After the first embolization, right occipital artery angiography showing a residual dural arteriovenous fistula after left occipital artery and superficial temporal artery embolization using Onyx. (b) After the second embolization, right carotid artery angiography showing a reduction of the shunt and remaining drainer. Right occipital artery is occluded by Onyx. The proximal segment of the right occipital artery is highly tortuous. Compared to the left occipital artery, the right occipital artery is occluded from the proximal segment. The fistulous portion of superior sagittal sinus is packed using coils of various sizes. (c) After the third embolization, right external carotid angiography showing complete obliteration of the dural arteriovenous fistula. Residual dural arteriovenous fistula is occluded by Onyx. The Onyx cast in the right occipital artery was extruded
Second embolization
We performed Onyx embolization from the right OA. However, Onyx infiltration into the fistula point was unsuccessful; therefore, transvenous embolization (TVE) was conducted. Through the 4F guiding catheter, a microcatheter (Neurodeo 10; Medico Hirata, Tokyo, Japan) was advanced over a microguidewire (Chikai 0.014 inch; Asahi Intecc, Nagoya, Japan) into the posterior third of the thrombosed SSS. The fistulous portion of SSS was tightly packed from the anterior to posterior end with coils of various sizes. However, little cortical venous drainage to the left parietal lobe was present [
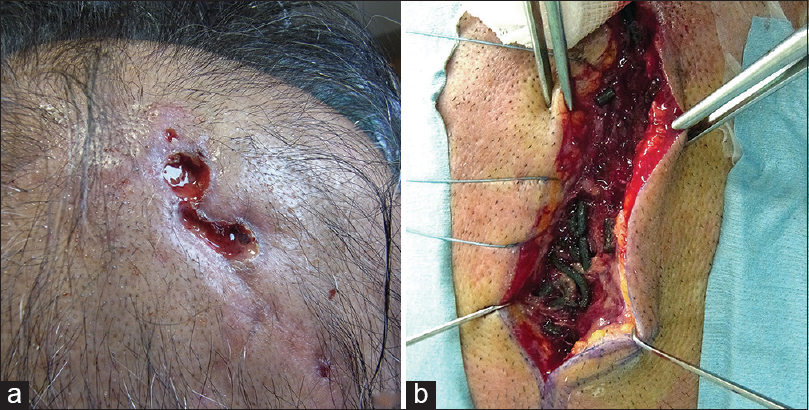
Two months after the last Onyx embolization, the patient complained of scalp pain along the right OA. Redness and swelling of his scalp were clearly observed exactly above OA, and Onyx casts were partially exposed within lesions [
Third embolization
Follow-up angiography revealed left MMA growth. Onyx embolization through the left MMA was performed, and complete occlusion of the fistula was achieved [
DISCUSSION
SSS-DAVFs account for approximately 8% of all DAVFs,[
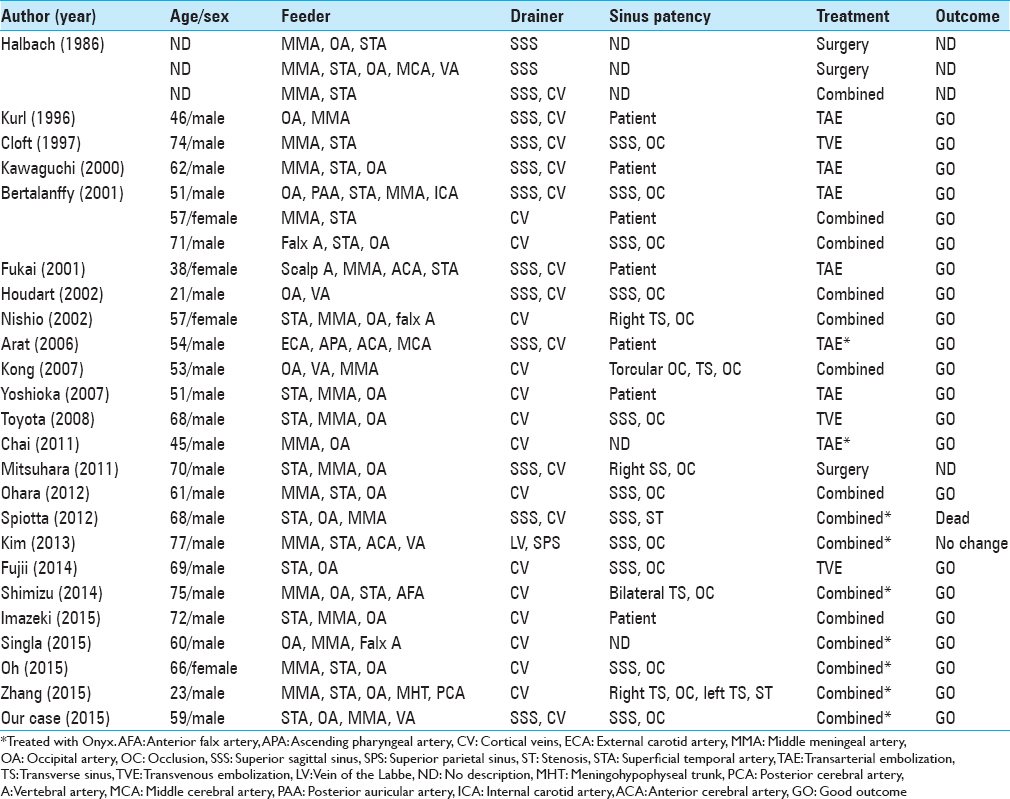
TAE alone was performed in seven cases (7/27, 25.9%). TAE with Onyx for DAVF has been increasingly used since Onyx was first available in the year 2000.[
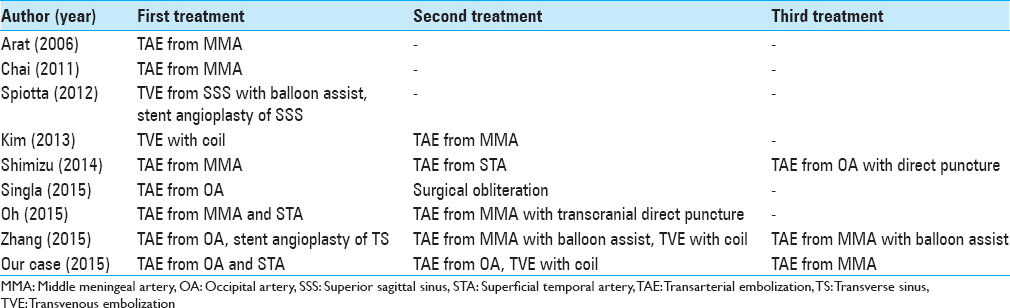
Combined treatment was the single most common choice, performed in 14 cases (51.9%). Total DAVF obliteration involving SSS is difficult because of their midline location and presence of multiple bilateral feeding arteries, sinus occlusion/stenosis, and scalp artery supply and critical cortical drainage pathway involvement. Therefore, simple TAE or TVE is usually not sufficient, similar to surgery alone because of the danger of intraoperative bleeding or the requirement of a large craniotomy to expose all drainage routes. Therefore, a combined treatment is indicated in most cases.[
In our case, TAE with Onyx was selected first. Because the bilateral MMAs were very thin to insert a microcatheter, we performed TAE from the left STA and OA. However, this only reduced blood flow through the fistula. The cause was high tortuosity of OA and STA. When injected from the proximal OA, Onyx only occluded OA itself and did not reach the fistula. Although an improvement of symptoms was noted after additional TVE, complete embolization was not achieved. We considered that surgical treatment would be useful as further treatment because the residual DAVF was quite localized. However, surgery would have been difficult because of scalp infection/necrosis. Consequently, endovascular therapy was considered a better treatment.
Onyx (eV3 Neurovascular, Irvine, California, USA), an ethylene vinyl alcohol copolymer dissolved in dimethyl sulfoxide (DMSO), is increasingly used as an embolic agent in intracranial vascular malformation management. Transarterial Onyx embolization is now an established DAVF treatment. Murayama et al. found that Onyx could cause inflammatory changes in the subacute and chronic phases after embolization.[
Based on a previous report,[
We described a case of Onyx cast extrusion through scalp arteries and ensuing infection following embolization of OA using Onyx. Most DAVFs in SSS involving scalp arteries require multimodality treatment. Special care should be taken when embolizing scalp arteries using Onyx as these may be prone to inflammatory damage, resulting in Onyx cast extrusion and infection.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Arat A, Inci S. Treatment of a superior sagittal sinus dural arteriovenous fistula with Onyx: Technical case report. Neurosurgery. 2006. 59: ONSE169-70
2. Bertalanffy A, Dietrich W, Kitz K, Bavinzski G. Treatment of dural arteriovenous fistulae (dAVF's) at the superior sagittal sinus (SSS) using embolisation combined with micro- or radiosurgery. Minim Invasive Neurosurg. 2001. 44: 205-10
3. Chai EQ, Wang J. Transarterial Onyx embolization of sagittal sinus dural arteriovenous fistulae. Neurol India. 2011. 59: 262-5
4. Chaloupka JC, Huddle DC, Alderman J, Fink S, Hammond R, Vinters HV. A reexamination of the angiotoxicity of superselective injection of DMSO in the swine rete embolization model. AJNR Am J Neuroradiol. 1999. 20: 401-10
5. Cloft HJ, Kallmes DF, Jensen JE, Dion JE. Percutaneous transvenous coil embolization of a type 4 sagittal sinus dural arteriovenous fistula: Case report. Neurosurgery. 1997. 41: 1191-3
6. Cognard C, Gobin YP, Pierot L, Bailly AL, Houdart E, Casasco A. Cerebral dural arteriovenous fistulas: Clinical and angiographic correlation with a revised classification of venous drainage. Radiology. 1995. 194: 671-80
7. Fujii H, Nagano Y, Hosomi N, Matsumoto M. Dural arteriovenous fistula presenting with progressive dementia and Parkinsonism. BMJ Case Rep 2014. 2014. p.
8. Fukai J, Terada T, Kuwata T, Hyotani G, Raimura M, Nakagawa M. Transarterial intravenous coil embolization of dural arteriovenous fistula involving the superior sagittal sinus. Surg Neurol. 2001. 55: 353-8
9. Halbach VV, Higashida RT, Hieshima GB, Rosenblum M, Cahan L. Treatment of dural arteriovenous malformations involving the superior sagittal sinus. AJNR Am J Neuroradiol. 1988. 9: 337-43
10. Houdart E, Saint-Maurice JP, Chapot R, Ditchfield A, Blanquet A, Lot G. Transcranial approach for venous embolization of dural arteriovenous fistulas. J Neurosurg. 2002. 97: 280-6
11. Hurst RW, Marcotte P, Raps EC, Flamm ES. Dural arteriovenous fistulas involving the superior sagittal sinus: Acute presentation with intracranial hemorrhage. Surg Neurol. 1998. 49: 42-6
12. Imazeki R, Amari K, Sekiguchi T, Mochizuki T, Shimizu S, Yamamoto M. Rapidly progressive dementia caused by a superior sagittal sinus dural arteriovenous fistula: A case report. Tokai J Exp Clin Med. 2015. 40: 22-6
13. Kakarla UK, Deshmukh VR, Zabramski JM, Albuquerque FC, McDougall CG, Spetzler RF. Surgical treatment of high-risk intracranial dural arteriovenous fistulae: Clinical outcomes and avoidance of complications. Neurosurgery. 2007. 61: 447-57
14. Kawaguchi T, Kawano T, Kaneko Y, Koizumi T, Tsutsumi M, Ooigawa H. Transarterial embolization with HEMA-MMA of variant convexity-superior sagittal sinus dural arteriovenous fistula - Case report. Neurol Med Chir (Tokyo). 2000. 40: 366-8
15. Kim ST, Jeong HW, Seo J. Onyx embolization of dural arteriovenous fistula, using Scepter C balloon catheter: A case report. Neurointervention. 2013. 8: 110-4
16. Kong DS, Kwon KH, Kim JS, Hong SC, Jeon P. Combined surgical approach with intraoperative endovascular embolization for inaccessible dural arteriovenous fistulas. Surg Neurol. 2007. 68: 72-7
17. Kurl S, Saari T, Vanninen R, Hernesniemi J. Dural arteriovenous fistulas of superior sagittal sinus: Case report and review of literature. Surg Neurol. 1996. 45: 250-5
18. Liu JK, Dogan A, Ellegala DB, Carlson J, Nesbit GM, Barnwell SL. The role of surgery for high-grade intracranial dural arteriovenous fistulas: Importance of obliteration of venous outflow. J Neurosurg. 2009. 110: 913-20
19. Ma C, Lu Q, Shi W, Su Z, Zhao Y, Li C. Diagnosis and treatment of a dural arteriovenous fistula presenting with progressive parkinsonism and dementia: A case report and literature review. Exp Ther Med. 2015. 9: 523-6
20. Mitsuhara T, Ikawa F, Ohbayashi N, Shirozu H, Abiko M, Ichinose N. A case of multiple dural arteriovenous fistulas treated by multiple modalities. No Shinkei Geka. 2011. 39: 575-80
21. Murayama Y, Viñuela F, Ulhoa A, Akiba Y, Duckwiler GR, Gobin YP. Nonadhesive liquid embolic agent for cerebral arteriovenous malformations: Preliminary histopathological studies in swine rete mirabile. Neurosurgery. 1998. 43: 1164-75
22. Nishio A, Ohata K, Tsuchida K, Tsuyuguchi N, Hara M, Komiyama M. Dural arteriovenous fistula involving the superior sagittal sinus following sinus thrombosis – Case report. Neurol Med Chir (Tokyo). 2002. 42: 217-20
23. Oh JS, Yoon SM, Shim JJ, Bae HG. Transcranial direct middle meningeal artery puncture for the onyx embolization of dural arteriovenous fistula involving the superior sagittal sinus. J Korean Neurosurg Soc. 2015. 57: 54-7
24. Ohara N, Toyota S, Kobayashi M, Wakayama A. Superior sagittal sinus dural arteriovenous fistulas treated by stent placement for an occluded sinus and transarterial embolization. A case report. Interv Neuroradiol. 2012. 18: 333-40
25. Pierot L, Visot A, Boulin A, Dupuy M. Combined neurosurgical and neuroradiological treatment of a complex superior sagittal sinus dural fistula: Technical note. Neurosurgery. 1998. 42: 194-7
26. Shimizu T, Iseki S, Oishi H, Hishii M. Lessons learned from a case of superior sagittal sinus dural arteriovenous fistula:strategy of endovascular treatment. No Shinkei Geka. 2014. 42: 1151-7
27. Singla A, Fargen KM, Hoh B. Onyx extrusion through the scalp after embolization of dural arteriovenous fistula. BMJ Case Rep 2015. 2015. p.
28. Spiotta AM, Sivapatham T, Hussain MS, Hui FK, Moskowitz SI, Gupta R. Combined surgical and endovascular approach to a complex dural arteriovenous fistula involving the superior sagittal sinus and torcula. J Stroke Cerebrovasc Dis. 2012. 21: 283-8
29. Toyota S, Fujimoto Y, Wakayama A, Yoshimine T. Complete cure of superior sagittal sinus dural arteriovenous fistulas by transvenous embolization through the thrombosed sinus in a single therapeutic session. A case report. Interv Neuroradiol. 2008. 14: 319-24
30. Yoshioka T, Kitagawa N, Yokoyama H, Nagata I. Selective transvenous coil embolization of dural arteriovenous fistula. A report of three cases. Interv Neuroradiol. 2007. 13: 123-30
31. Zhang Y, Li Q, Huang QH. Embolization of a superior sagittal sinus dural arteriovenous fistula under intrasinus balloon protection: A case report. Interv Neuroradiol. 2015. 21: 94-100

