

- Pars Advanced and Minimally Invasive Medical Manners Research Center, Pars Hospital, Iran University of Medical Sciences, Tehran, Iran
Correspondence Address:
Naser Asgari
Pars Advanced and Minimally Invasive Medical Manners Research Center, Pars Hospital, Iran University of Medical Sciences, Tehran, Iran
DOI:10.4103/sni.sni_308_18
Copyright: © 2018 Surgical Neurology International This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.How to cite this article: Abolfazl Rahimizadeh, Naser Asgari, Housain Soufiani, Shaghayegh Rahimizadeh. Ossification of the cervical ligamentum flavum and case report with myelopathy. 24-Dec-2018;9:263
How to cite this URL: Abolfazl Rahimizadeh, Naser Asgari, Housain Soufiani, Shaghayegh Rahimizadeh. Ossification of the cervical ligamentum flavum and case report with myelopathy. 24-Dec-2018;9:263. Available from: http://surgicalneurologyint.com/surgicalint-articles/9144/
Date of Submission
09-Sep-2018
Date of Acceptance
21-Nov-2018
Date of Web Publication
24-Dec-2018
Abstract
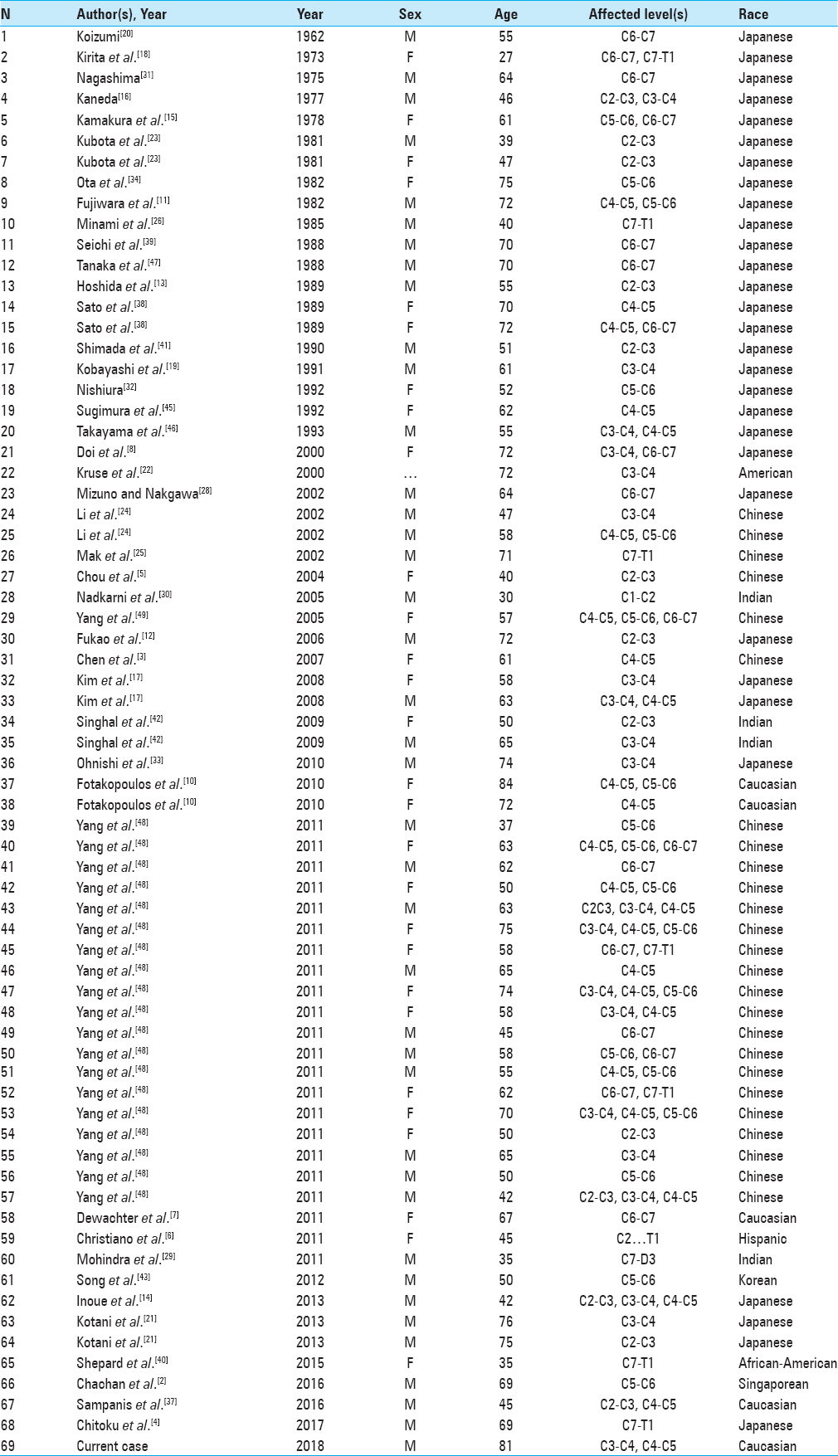
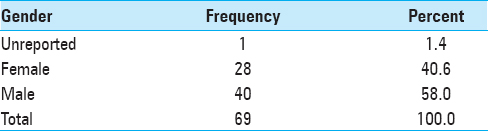
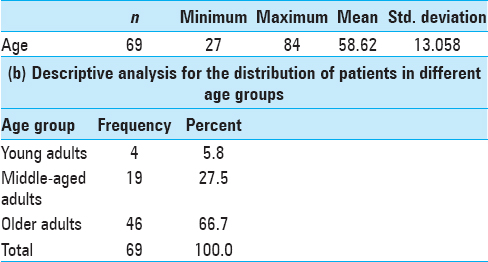
Background:Ossification of the ligamentum flavum (OLF) occurs mostly in adult males, typically in the thoracolumbar spine where it may contribute to neurological deficits. Here we reviewed 68 cases of cervical OLF resulting in progressive quadriparesis.
Methods:The literature on cervical OLF was reviewed between 1962 and 2018 along with the case of an 81-year-old male with progressive quadriparesis attributed to cervical OLF.
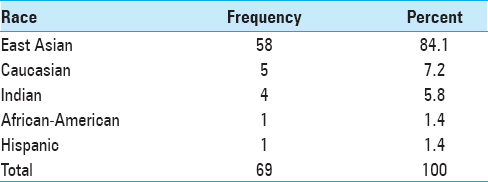
Results:Most patients with cervical OLF are Asian, with Caucasians constituting the second most frequently impacted population.
Conclusions:Cervical OLF is typically reported in the Asian, followed by the Caucasian population, and is most often found in the thoracolumbar spine. Here we presented an 81-year-old male with cervical OLF contributing to quadriparesis.
Keywords: Cervical myelopathy, cervical spine, ossification of ligamentum flavum, ossification of posterior longitudinal ligament, ossification of yellow ligament, review article
INTRODUCTION
Ossification of the ligamentum flavum (OLF) typically occurs in adults involving the thoracolumbar spine. It is less frequently encountered in the cervical region (<1%).[
CASE REPORT
An 81-year-old bed-ridden male presented a spastic quadriparesis. The T1-weighted sagittal magnetic resonance image (MRI) showed a large heterogeneous mass resulting in dorsolateral cord compression at C4-C5, and a smaller lesion at the C5-C6 levels, consistent with OLF [
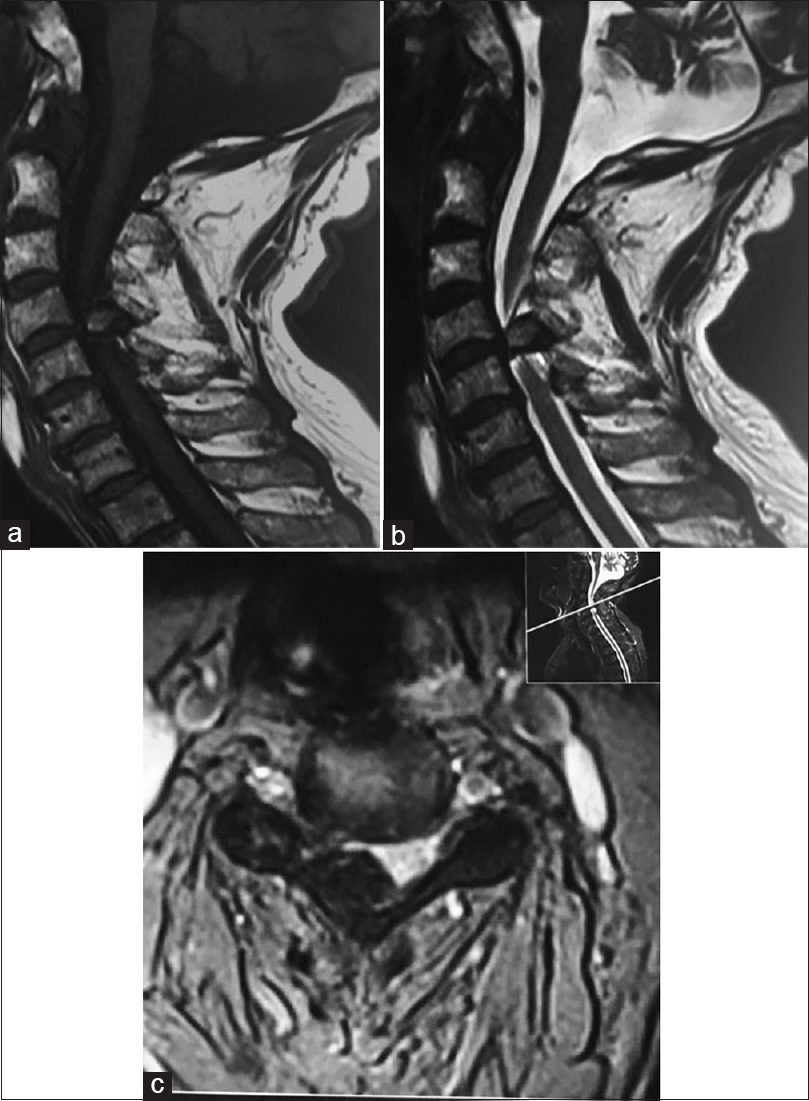
Figure 1
Cervical MRI: (a) T1-weighted sagittal image showing a heterointense epidural mass at the posterior aspect of the spinal cord at the C4-C5 level, a smaller one is visualized below this level. (b) T2-weighted sagittal image demonstrating a hypointense mass with an isointensity at the center of the mass. (c) It also reveals a significant reduction in the cervical canal diameter
The patient underwent a C4-C6 laminectomy for resection of large dorsolateral OLF masses (C45, C56) [

DISCUSSION
About 80% of the ligamentum flavum is composed of elastic fibers, and 20% with collagen.[
Incidence
There are 69 previously reported cases of cervical OLF
Clinical picture
Patients with cervical OLF often present late in the clinical course with cord compression/spondylosis resulting in chronic myeloradiculopathy and an evolving quadriparesis.[
Imaging
Lateral cervical plain radiographs may demonstrate OLF located between the bases of two spinal processes.[
Treatment
A decompressive laminectomy with excision of OLF may be warranted in symptomatic patients. The OLF dissection from the dura should be accomplished under the operating microscope to lyse adhesions. Li et al. described decompressive en-block laminectomy for removal of OLF.[
Outcome
Typically following a cervical laminectomy with resection of OLF, patients should significantly recover from their preoperative myeloradicular syndrome.
Summary
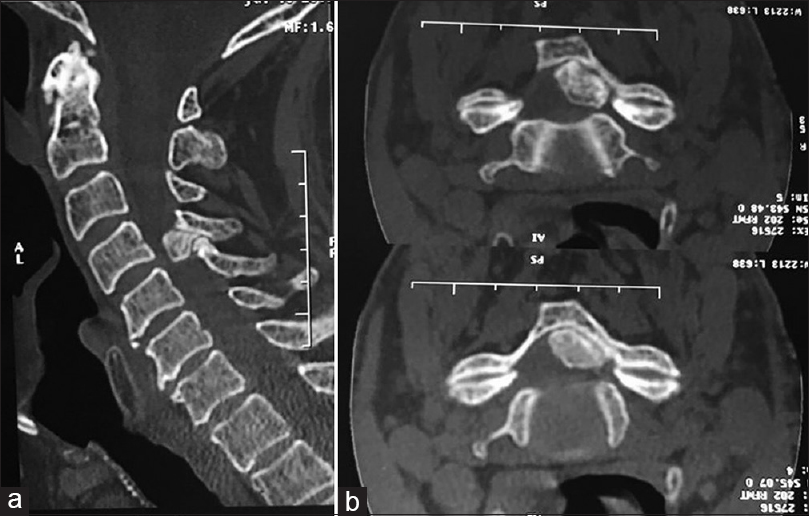
Cervical OLF rarely causes cervical myeloradiculopathy. Following both MR and CT studies to adequately document the location/extent of disease, laminectomy alone often suffices to decompress the cord.
Declaration of patient consent
Written informed consent was obtained from the patient for publication and corresponding images.
Contribution
The steps of this article from design to writing were made by Abolfazl Rahimizadeh, Naser Asgari, Housain Soufiani, and Shaghayegh Rahimizadeh, retrospectively.
Ethical approval
Approved.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Chachan S, Kasat NS, Keng PTL. Cervical myelopathy secondary to combined ossification of ligamentum flavum and posterior longitudinal ligament—A case report. Int J Spine Surg. 2018. 12: 121-5
2. Chachan S, Kasat NS, Thng PK. Cervical myelopathy secondary to combined ossification of ligamentum flavum and posterior longitudinal ligament. J Spinal Surg. 2016. 3: 157-9
3. Chen P-Y, Lin C-Y, Tzaan W-C, Chen H-C. Brown-Sequard syndrome caused by ossification of the ligamentum flavum. J Clin Neurosci. 2007. 14: 887-90
4. Chitoku S, Nishiura I, Fukuda M, Amano S. Ossification of the yellow ligament combined with ossification of the posterior longitudinal ligament at the cervicothoracic junction. World Neurosurg. 2017. 103: 952.e19-952.e22
5. Chou Y-C, Lee C-C, Yen P-S, Lin J-F, Su C-F, Lin S-Z. Cough induced by ossification of the ligamentum flavum in the high cervical spine: Case report. J Neurosurg Spine. 2004. 100: 364-6
6. Christiano LD, Assina R, Goldstein IM. Ossification of the ligamentum flavum: A unique report of a Hispanic woman. Neurosurg Focus. 2011. 30: E15-
7. Dewachter L, Govaere F, Crevits I, De Man R. Images in clinical radiology. JBR–BTR. 2011. 94: 219-
8. Doi S, Kageyama Y, Nagahusa T, Okada M. Ossification of the ligamentum flavum of the cervical spine. Case report. Seikei Geka. 2000. 51: 1659-62
9. Epstein NE. Laminectomy with posterior wiring and fusion for cervical ossification of the posterior longitudinal ligament, spondylosis, ossification of the yellow ligament, stenosis, and instability: A study of 5 patients. J Spinal Disord. 1999. 12: 461-6
10. Fotakopoulos G, Alexiou G, Mihos E, V oulgaris S. Ossification of the ligamentum flavum in cervical and thoracic spine. Report of three cases. Acta Neurol Belg. 2010. 110 N2: 186-9
11. Fujiwara M, Bitoh S, Hasegawa H, Nakata M, Hata H. A case of nodular calcification of the ligamentum flavum with ossification of the posterior longitudinal ligament in the cervical spine. No Shinkei Geka. 1982. 10: 769-74
12. Fukao S, Hanakita J, Kitahama Y, Minami M, Tamiya A. Ossification of the ligamentum flavum of the upper cervical spine a case report. Spinal Surg. 2006. 20: 49-54
13. Hoshida T. Three cases of ossified and calcified nodules in the cervical ligamentum flavum. Osaka Keisatsu Byoin Igaku Zasshi. 1989. 13: 71-9
14. Inoue H, Seichi A, Kimura A, Endo T, Hoshino Y. Multiple-level ossification of the ligamentum flavum in the cervical spine combined with calcification of the cervical ligamentum flavum and posterior atlanto-axial membrane. Eur Spine J. 2013. 22: 416-20
15. Kamakura K, Furukawa T, Takasu T, Mannen T, Toyokura Y. Cervical myelopathy due to ossification of ligamenta flava: Report of a case (author's transl). Rinsho Shinkeigaku. 1978. 18: 96-102
16. Kaneda K. Study of an operative case with a myelopathy due to the ossification of the thoracic spinal canal. Rinsho Seikeigeka. 1977. 12: 387-94
17. Kim K, Isu T, Nomura R, Kobayashi S, Teramoto A. Cervical ligamentum flavum ossification. Neurol Med Chir (Tokyo). 2008. 48: 183-7
18. Kirita Y, Miyazaki K, Lin D, Nosaka K, Shima M, Yamamura H. Surgical treatment for the ossification of the ligamentum flavum. Chubu Nippon Seikeigeka Saigaigeka Gakkai Zasshi. 1973. 16: 814-7
19. Kobayashi S, Okada K, Onoda K, Horikoshi S. Ossification of the cervical ligamentum flavum. Surg Neurol. 1991. 35: 234-8
20. Koizumi M. Three cases of spinal cord paralysis proved by ligamenta flava ossification. Rinsho-Geka (Clin Surg). 1962. 17: 1181-8
21. Kotani Y, Takahata M, Abumi K, Ito M, Sudo H, Minami A. Cervical myelopathy resulting from combined ossification of the ligamentum flavum and posterior longitudinal ligament: Report of two cases and literature review. Spine J. 2013. 13: e1-6
22. Kruse JJ, Awasthi D, Harris M, Waguespack A. Case report. Ossification of the ligamentum flavum as a cause of myelopathy in North America: Report of three cases. Clin Spine Surg. 2000. 13: 22-5
23. Kubota M, Baba I, Sumida T. Myelopathy due to ossification of the ligamentum flavum of the cervical spine a report of two cases. Spine. 1981. 6: 553-9
24. Li K-K, Chung O-M, Chang Y-P, So Y-C. Myelopathy caused by ossification of ligamentum flavum. Spine. 2002. 27: E308-12
25. Mak K-h, Mak K-l, Gwi-Mak E. Ossification of the ligamentum flavum in the cervicothoracic junction: Case report on ossification found on both sides of the lamina. Spine. 2002. 27: E11-4
26. Minami Y, Maeyama I, Kawakami T, Sakinaga Y. A case of cervical myelopathy due to ossification of the ligamentum flavum. Orthop Traumatol. 1985. 34: 335-7
27. Miyazawa N, Akiyama I, Di Lorenzo N, Mouchaty H. Ossification of the ligamentum flavum of the cervical spine/comment. J Neurosurg Sci. 2007. 51: 139-44
28. Mizuno J, Nakagawa H. Unilateral ossification of the ligamentum flavum in the cervical spine with atypical radiological appearance. J Clin Neurosci. 2002. p. 9462-4
29. Mohindra S, Gupta R, Chhabra R, Gupta SK. Compressive myelopathy due to ossified yellow ligament among South Asians: Analysis of surgical outcome. Acta Neurochir (Wien). 2011. 153: 581-7
30. Nadkarni TD, Menon RK, Desai KI, Goel A. Ossified ligamentum flavum of the atlantoaxial region. J Clin Neurosci. 2005. 12: 486-9
31. Nagashima C, Takahama M, Nakayama Y, Asano T. Giant occipital hemangioendothelioma with thrombocytopenia, anemia, and hypofibrinogenemia: Case report. J Neurosurg. 1975. 43: 74-9
32. Nishiura I. Cervical radiculopathy due to ossification of yellow ligament: A case report. Sekitsui Sekizui J. 1992. 5: 383-5
33. Ohnishi Y-I, Iwatsuki K, Yoshimura K, Ishihara M, Yoshimine T. Incarcerated herniation of the cervical spinal cord after laminectomy for an ossification of the yellow ligament. Eur Spine J. 2010. 19: 140-3
34. Ota S. A case of cervical myelopathy due to ossification of the ligamentum-flavum. Chubu Nippon Seikeigeka Saigaigeka Gakkai Zasshi. 1982. 25: 966-8
35. Rahimizadeh A. Isolated proximal thoracic ossified ligamentum flavum causing paraparesis in a caucasian: A case report and review of literature. World Spinal Column J. 2012. 3: 38-43
36. Rahimizadeh A, Soufiani H, Amirzadeh M, Rahimizadeh S. Ossification of the ligamentum flavum of the lumbar spine in caucasians: Case series. J Spine Neurosurg. 2017. 6: 5-
37. Sampanis N, Gavriilaki E, Paschou E, Kalaitzoglou A, Vasileiou S. Ossification of the cervical ligamentum flavum and osseous brown tumor: Late manifestations of primary hyperparathyroidism misdiagnosed in a case of parathyroid carcinoma. Clin Cases Miner Bone Metab. 2016. 13: 54-6
38. Sato K, Hayashi M, Kubota T, Kawano H, Handa Y, Kabuto M. Symptomatic calcification and ossification of the cervical ligamentum flavum: Clinical, radiological and pathological features. Br J Neurosur. 1989. 3: 597-602
39. Seichi A, Katoh H, Tanaka H, Tuzuki N. Radiculomyelopathy due to ossification of the ligamentum flavum of the cervical spine; a case report. Seikeigeka. 1988. 39: 929-32
40. Shepard NA, Shenoy K, Cho W, Sharan AD. Extensive ossification of the ligamentum flavum treated with triple stage decompression: A case report. Spine J. 2015. 15: e9-14
41. Shimada Y. Ossification of the ligamentum flavum of the cervical spine. Case report. Seikeigeka To Saigaigeka. 1990. 33: 399-403
42. Singhal U, Jain M, Jaiswal AK, Behari S. Unilateral ossified ligamentum flavum in the high cervical spine causing myelopathy. Indian J Orthop. 2009. 43: 305-8
43. Song JY, Park JH, Roh SW. Ossified ligamentum flavum causing cervical myelopathy. Korean J Spine. 2012. 9: 24-7
44. Sonntag VK. Ossification of the ligamentum flavum (OLF): An increasing cause of cervical myelopathy. World Neurosurg. 2011. 3: 445-6
45. Sugimura H, Kakitsubata Y, Suzuki Y, Kakitsubata S, Tamura S, Uwada O. MRI of ossification of ligamentum flavum. J Comput Assist Tomogr. 1992. 16: 73-6
46. Takayama S, Kuribayashi K, Miyamoto Y, Nakasu Y, Handa J. Ossification and calcification of the cervical ligamentum flavum--case reports. No to shinkei. 1993. 45: 859-63
47. Tanaka H, Tsuzuki N, Seichi A, Hotta Y, Iizuka T. Anatomical study of ossification and calcification of the yellow ligament of spine with reference to the distribution of the yellow ligament. Rinsho Seikei Geka. 1988. 23: 411-7
48. Yang J, Ni B, Xie N, Guo Q, Wang L. Surgical treatments of myelopathy caused by cervical ligamentum flavum ossification. World Neurosurg. 2011. 75: 546-50
49. Yang JC, Lin CP, Chan JY, Liu YK, Huang JS. Surgical treatment of multilevel cervical radiculomyelopathy caused by the concomitant ossification of the ligamentum flavum and the posterior longitudinal ligament. Surg Pract. 2005. 9: 111-4

