

- Neurosurgical Department, UHC Ibn Rochd, Hassan II University, Casablanca, Morocco
Correspondence Address:
Said Hilmani
Neurosurgical Department, UHC Ibn Rochd, Hassan II University, Casablanca, Morocco
DOI:10.4103/2152-7806.195580
Copyright: © 2016 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Said Hilmani, Yassine Houass, Abdessamad El Azhari. Paraventricular meningioma revealed by mental disorder. 12-Dec-2016;7:
How to cite this URL: Said Hilmani, Yassine Houass, Abdessamad El Azhari. Paraventricular meningioma revealed by mental disorder. 12-Dec-2016;7:. Available from: http://surgicalneurologyint.com/surgicalint_articles/paraventricular-meningioma-revealed-by-mental-disorder/
Date of Submission
18-Jun-2016
Date of Acceptance
15-Sep-2016
Date of Web Publication
12-Dec-2016
Abstract
Background:Ventricular meningioma constitutes 2% of intracranial meningioma, representing a challenging disease for neurosurgeons. Although cognitive impairment is one of the major symptoms of ventricular tumors, few studies have reported the details of cognitive impairment before and after their surgical removal. The expected effects on cognitive function should also be considered when choosing a surgical approach.
Case Descriptions:We report the case of a large lateral ventricle meningioma revealed by cognitive dysfunction and moderate intellectual disability. The patient underwent subtotal resection of the tumor which had partial improvement in cognitive disorders. It is important to precisely assess neuropsychological function in patients with large brain tumors, and judicious preoperative plan, adequate knowledge of anatomy, and use of correct microsurgical techniques are fundamental in achieving complete resection of paraventricular meningioma with low morbidity.
Conclusion:Pre and postoperative precise neuropsychological examinations may identify the potential cognitive impairment and beneficial effects of surgery in patients with large lateral ventricle meningiomas.
Keywords: Meningioma, mental disorder, ventricle
INTRODUCTION
Ventricular meningioma constitutes 2% of intracranial meningioma,[
Here, we report the case of a large lateral ventricle meningioma associated with cognitive dysfunction and intellectual disability. The patient underwent subtotal resection of the tumor with an improvement in cognitive disorders.
CASE REPORT
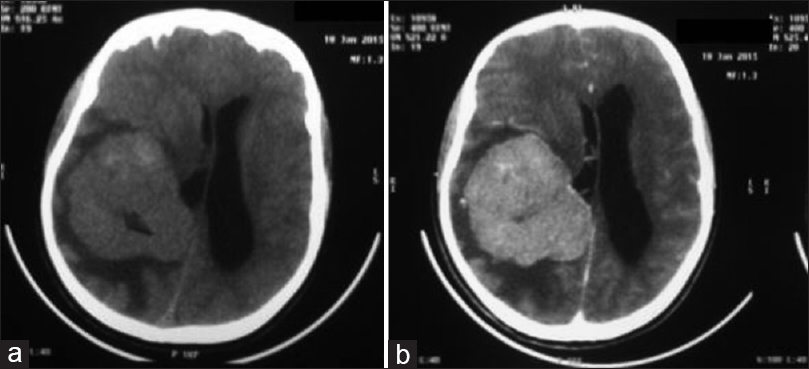
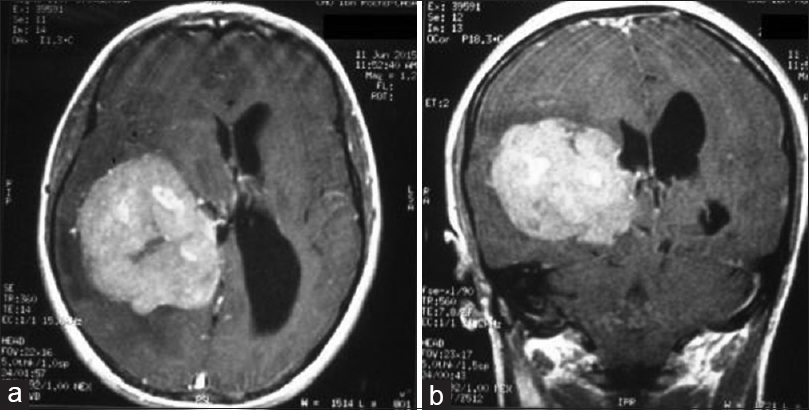
A 26-year-old women had moderate intellectual disability with cognitive disorders. She presented with increase intracranial hypertension and seizure, but without motor or sensitive disturbance. The fundus showed papillary edema. Computed tomography (CT) scan demonstrated an isodense tumor located in the right paraventricular at the occipitotemporal region [
DISCUSSION
Meningiomas arising in the ventricular system without dural attachment are extremely rare, with an incidence of 0.5–3% (average 2%) among all intracranial meningiomas.[
Cognitive impairment is well known as a major symptom of entlateral vricular tumors and may potentially be complicated after their surgical removal.[
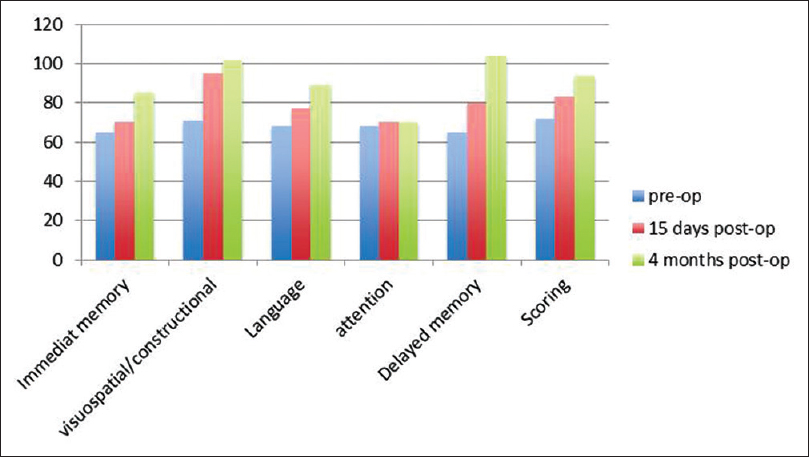
RBANS score was selected to identify and evaluate cognitive disorders before and after the surgery. The RBANS consists of 12 subtests and yields index scores for 5 traits, namely, attention (digit span, coding), language (picture naming, semantic fluency), visuospatial/constructional abilities (figure copy, line orientation), immediate memory (list learning, story memory), and delayed memory (list recall, list recognition, story recall, figure recall). Scores can be normalized for age, sex, ethnicity, and level of education, with a score of 100 and a standard deviation of 15 for the index group.[
The optimal surgical approach for a paraventricular meningioma is still controversial. In general, there are three main surgical approaches to remove lateral ventricle tumors, namely the superior parietal, transcallosal, and middle temporal gyrus approaches.[
In our opinion, the objective is not to obtain maximum tumor resection but extirpation with less surgical morbidity and minimal or no damage to surrounding brain tissue. The aim must be a good exposure of the lesion as well as an early visualization of the arterial pedicle. Occlusion of these vessels results in tumor hemostasis. Piecemeal removal is crucial for achieving resection of the tumor with minimum damage and for careful intraoperative hemostasis to ovoid intraventricular hemorrhage.
CONCLUSION
In conclusion, pre and postoperative precise neuropsychological examinations may identify the potential cognitive impairment and beneficial effects of surgery in patients with large lateral ventricle meningiomas. The cure of meningioma of this tumor can be achieved with appropriately selecting surgical route according to the anatomical features of the region, characteristics of the individual presentation such as size, location, growing patterns, and clinical preoperative deficits.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Alver I, Abuzayed B, Kafadar AM, Muhammedrezai S, Sanus GZ, Akar Z. Primary fourth ventricular meningioma: Case report and review of the literature. Turk Neurosurg. 2011. 21: 249-53
2. Barrow DL, Dawson R. Surgical management of arteriovenous malformations in the region of the ventricular trigone. Neurosurgery. 1994. 35: 1046-54
3. Bertalanffy A, Roessler K, Koperek O, Gelpi E, Prayer D, Neuner M. Intraventricular meningiomas: A report of 16 cases. Neurosurg Rev. 2006. 29: 30-5
4. Bhatoe HS, Singh P, Dutta V. Intraventricular meningiomas: A clinicopathological study and review of the literature. Neurosug Focus. 2006. 20: 1-6
5. Criscuolo GR, Symon L. Intraventricular meningioma. A review of 10 cases of the National Hospital, Queen Square (1974-1985) with reference to the literature. Acta Neurochir. 1986. 83: 83-91
6. D’Angelo VA, Galarza M, Catapano D, Monte V, Bisceglia M, Carosi I. Lateral ventricle tumors: Surgical strategies according to tumor origin and development-a series of 72 cases. Neurosurgery. 2005. 56: 36-45
7. Erman T, Göçer AI, Erdogan S, Boyar B, Hactyakupoglu S, Zorludemir S. Intraventricular meningiomas. A review of the literature and report of 8 cases. Neurosurg Q. 2004. 14: 154-60
8. Faquini I, Fonseca RB, Vale de Melo SL, Negri H, Vieira E, Saboia T. Trigone ventricular meningiomas: Is it possible to achieve good results even in the absence of high tech tools?. Surg Neurol Int. 2015. 6: 180-
9. Fornari M, Savoiardo G, Morello G, Solero CL. Meningiomas of the lateral ventricles. Neuroradiological and surgical considerations in 18 cases. J Neurosurg. 1981. 54: 64-74
10. Gokalp HZ, Yuceer N, Arasil E, Deda H, Attar A, Erdogăan A. Tumours of the lateral ventricle. A retrospective review of 112 cases operated upon 1970-1997. Neurosurg Rev. 1998. 21: 126-37
11. Guidetti B, Delfini R, Gagliardi FM, Vagnozzi R. Meningiomas of the lateral ventricles. Clinical, neuroradiologic, and surgical considerations in 19 cases. Surg Neurol. 1985. 24: 364-70
12. Kashiwazaki D, Takaiwa A, Nagai S, Akioka N, Kurosaki K, Noguchi K. Reversal of Cognitive Dysfunction by Total Removal of a Large Lateral Ventricle Meningioma: A Case Report with Neuropsychological Assessments. Case Rep Neurol. 2014. 22: 44-9
13. Kawashima M, Li X, Rhoton AL, Ulm AJ, Oka H, Fujii K. Surgical approaches to the atrium of the lateral ventricle: Microsurgical anatomy. Surg Neurol. 2006. 65: 436-45
14. Kim EY, Kim ST, Kim HJ, Jeon P, Kim KH, Byun HS. Intraventricular meningiomas: Radiological findings and clinical features in 12 patients. Clin Imaging. 2009. 33: 175-80
15. Levin HS, Speirs PA, Heilman K, Valenstein E.editors. Acalculia. Clinical Neuropsychology. New York: Oxford University Press; 1985. p. 97-113
16. Liu M, Liu Y, Zhu S, Li X. Intraventricular meningiomas: A report of 25 cases. Neurosurg Rev. 2006. 29: 36-40
17. Lyngdoh BT, Giri PJ, Behari S, Banerji D, Chhabra DK, Jain VK. Intraventric- ular meningiomas: A surgical challenge. J Clin Neurosc. 2007. 14: 442-8
18. Mahaney KB, Abdulrauf SI. Anatomic relationship of the optic radiations to the atrium of the lateral ventricle: Description of a novel entry point to the trigone. Neurosurgery. 2008. 63: 195-202
19. McDermott MW. Intraventricular meningiomas. Neurosurg Clin N Am. 2003. 14: 559-69
20. Milligan BD, Meyer FB. Morbidity of transcallosal and transcortical approaches to lesions in and around the lateral and third ventricles: A single-institution experience. Neurosurgery. 2010. 67: 1483-96
21. Nakamura M, Roser F, Bundschuh O, Vorkapic P, Samii M. Intraventricular meningiomas: A review of 16 cases with reference to the literature. Surg Neurol. 2003. 59: 491-504
22. Nishizaki T, Ikeda N, Nakano S, Okamura T, Abiko S. Occipital inter-hemispheric approach for lateral ventricular trigone meningioma. Acta Neurochir. 2009. 151: 1717-21
23. Peltier J, Travers N, Destrieux C, Velut S. Optic radiations: A microsurgical anatomical study. J Neurosurg. 2006. 105: 294-300
24. Randolph C, Tierney MC, Mohr E, Chase TN. The Repeatable Battery for the Assessment of Neuropsychological Status (RBANS): Preliminary clinical validity. J Clin Exp Neuropsychol. 1998. 20: 310-9
25. Takaiwa A, Hayashi N, Kuwayama N, Akioka N, Kubo M, Endo S. Changes in cognitive function during the 1-year period following endarterectomy and stenting of patients with high-grade carotid artery stenosis. Acta Neurochir. 2009. 151: 1593-600
26. Villani R, Papagno C, Tomei G, Grimoldi N, Spagnoli D, Bello L. Transcallosal approach to tumors of the third ventricle: Surgical results and neuropsy- chological evaluation. J Neurosurg Sci. 1997. 41: 41-50
27. Zając-Mnich M, Kostkiewicz A, Guz W, Dziurzyńska-Białek E, Solińska A, Stopa J. Clinical and morphological aspects of gray matter heterotopia type developmental malformations. Pol J Radiol. 2014. 79: 502-7
28. Zanini MA, Faleiros AT, Almeida CR, Clara CA, Gabarra RC. Trigone ventricular meningiomas: Surgical approaches. Arq Neuro-Psiquiatr. 2011. 69: 670-5

