

- Department of Neurosurgery, Azienda Ospedaliero Universitaria “Renato Dulbecco” di Catanzaro, Catanzaro, Italy
- Department of Neurosurgery, Azienda Ospedaliero Universitaria di Sassari, Sassari, Italy
- Medical Oncology Unit, University Hospital of Parma, Parma, Italy.
Correspondence Address:
Domenico Policicchio, Department of Neurosurgery, Azienda Ospedaliero Universitaria “Renato Dulbecco” di Catanzaro, Catanzaro, Italy.
DOI:10.25259/SNI_982_2023
Copyright: © 2024 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Domenico Policicchio1, Riccardo Boccaletti2, Gina Casu2, Anna Mingozzi3, Giampiero Muggianu2, Giovanni Nodari2, Walter Marco Sias2, Giosué Dipellegrini2. Pedicled multifidus muscle flaps to treat dural tears due to penetrating spinal stab wounds: Two case reports and a literature review. 19-Jan-2024;15:19
How to cite this URL: Domenico Policicchio1, Riccardo Boccaletti2, Gina Casu2, Anna Mingozzi3, Giampiero Muggianu2, Giovanni Nodari2, Walter Marco Sias2, Giosué Dipellegrini2. Pedicled multifidus muscle flaps to treat dural tears due to penetrating spinal stab wounds: Two case reports and a literature review. 19-Jan-2024;15:19. Available from: https://surgicalneurologyint.com/surgicalint-articles/12712/
Date of Submission
08-Dec-2023
Date of Acceptance
03-Jan-2024
Date of Web Publication
19-Jan-2024
Abstract
Background: Penetrating spinal injuries occasionally lead to dural tears (DT) and cerebrospinal fluid (CSF) leaks that risk both infectious and neurological complications. Here, we reviewed two cases and the literature regarding the safety/efficacy and limitations of repairing traumatic DT utilizing pedicled multifidus muscle flaps.
Case Description: Two males, ages 73 and 50, presented with Brown-Sequard syndromes and DT/CSF fistulas attributed to knife-induced spinal injuries at the D3–D4 and D11–D12 levels. Intraoperatively, DT was repaired utilizing pedicle multifidus muscle flaps. Postoperatively, both patients demonstrated partial recovery of neurological function along with no residual symptoms/signs of DT/CSF fistulas.
Conclusion: Penetrating traumatic spinal injuries may result in DT/CSF fistulas that can be adequately repaired utilizing pedicle multifidus muscle flaps.
Keywords: CSF leakage, Dural tear, Pedicled multifidus muscle flap, Penetrating spinal injury, Spine surgery
INTRODUCTION
Penetrating spinal injuries may result in dural tears (DT)/cerebrospinal fluid (CSF) leaks that can result in wound infections, meningitis, and abscesses.[
CASES DESCRIPTIONS
Case 1: Clinical presentation
A 73-year-old male presented with paraparesis (left plegic; right paretic), hypoesthesia from the chest down, and a CSF leak following a posterior T3–T4 knife wound. The magnetic resonance (MR)-documented a left T3–T4 ligamentum flavum laceration, a dural tear, and a thin left-sided posterolateral T2–T5 subdural hematoma (SDH). The computed tomography (CT) showed a fracture of the left upper T3 facet joint [
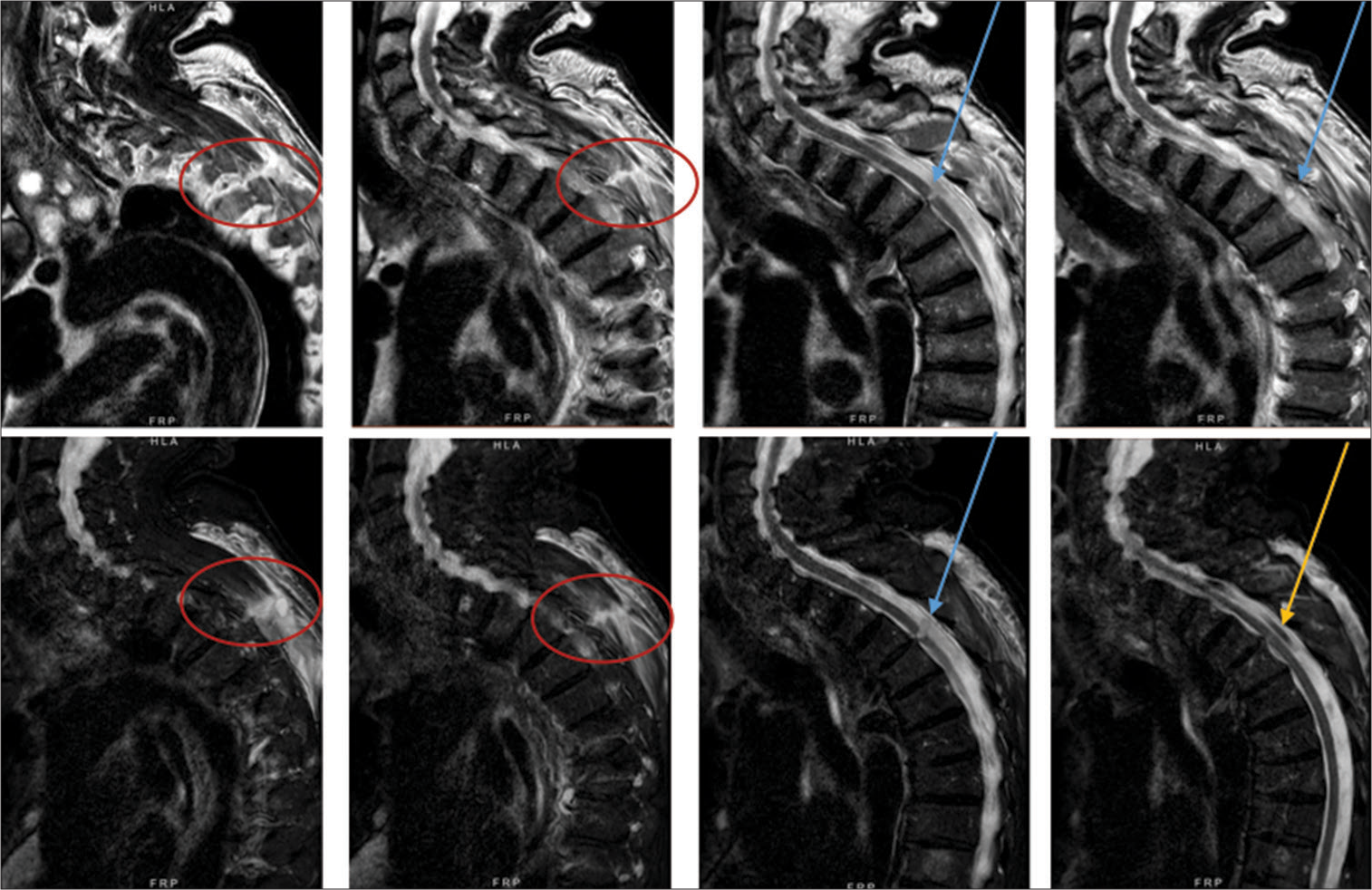
Figure 1:
Spinal magnetic resonance imaging of patient 1. Upper row: sagittal slices, T2-weighted sequences. Lower row: sagittal slices, short-tau inversion recovery sequences. Red circles indicate a fracture of the articular facet and a laceration of the yellow ligament on the left. Blue arrows indicate the spinal cord lesion; yellow arrow indicates subdural hematoma.
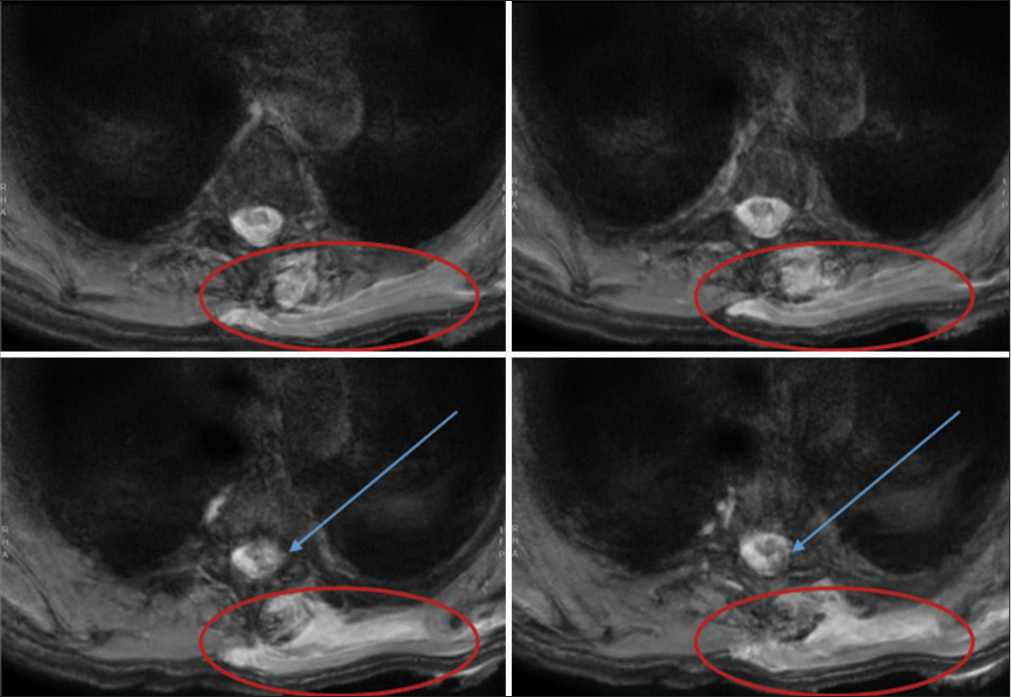
Figure 2:
Spinal magnetic resonance imaging of patient 1. Axial slices, short-tau inversion recovery sequences. Red circles indicate a fracture of the articular facet, a laceration of the yellow ligament, and a contusion of the paravertebral tissues on the left. Blue arrows indicate the spinal cord lesion.
Surgery
A left-sided T4 hemilaminectomy and partial T3–T5 hemilaminectomies allowed for the removal of the SDH. However, the significant lateral/foraminal and anterolateral DT/CSF leak was non-suturable and required an indirect dural repair using the CO2 laser and a pedicled multifidus muscle flap.[
Postoperative course
Postoperatively, the patient was placed on seven days of cefazolin, during which time the motor function of the right lower extremities improved, but the left remained plegic. The postoperative magnetic resonance imaging (MRI) confirmed adequate thoracic cord decompression and appropriate placement of the pedicled multifidus muscle flap repair [
Case 2
Twenty-four hours after a stab wound at the D11–D12 level, a 50-year-old male presented with right lower extremity paralysis, bilateral lower extremity sensory deficits, and a DT/CSF leak. The thoracic CT scan showed no retained metallic fragments or bony pathology. The MRI showed a tear in the right yellow/interspinous ligaments at the D11–D12 level, a laceration of the right posterolateral cord, and a DT/CSF with CSF extending into the paravertebral muscles [
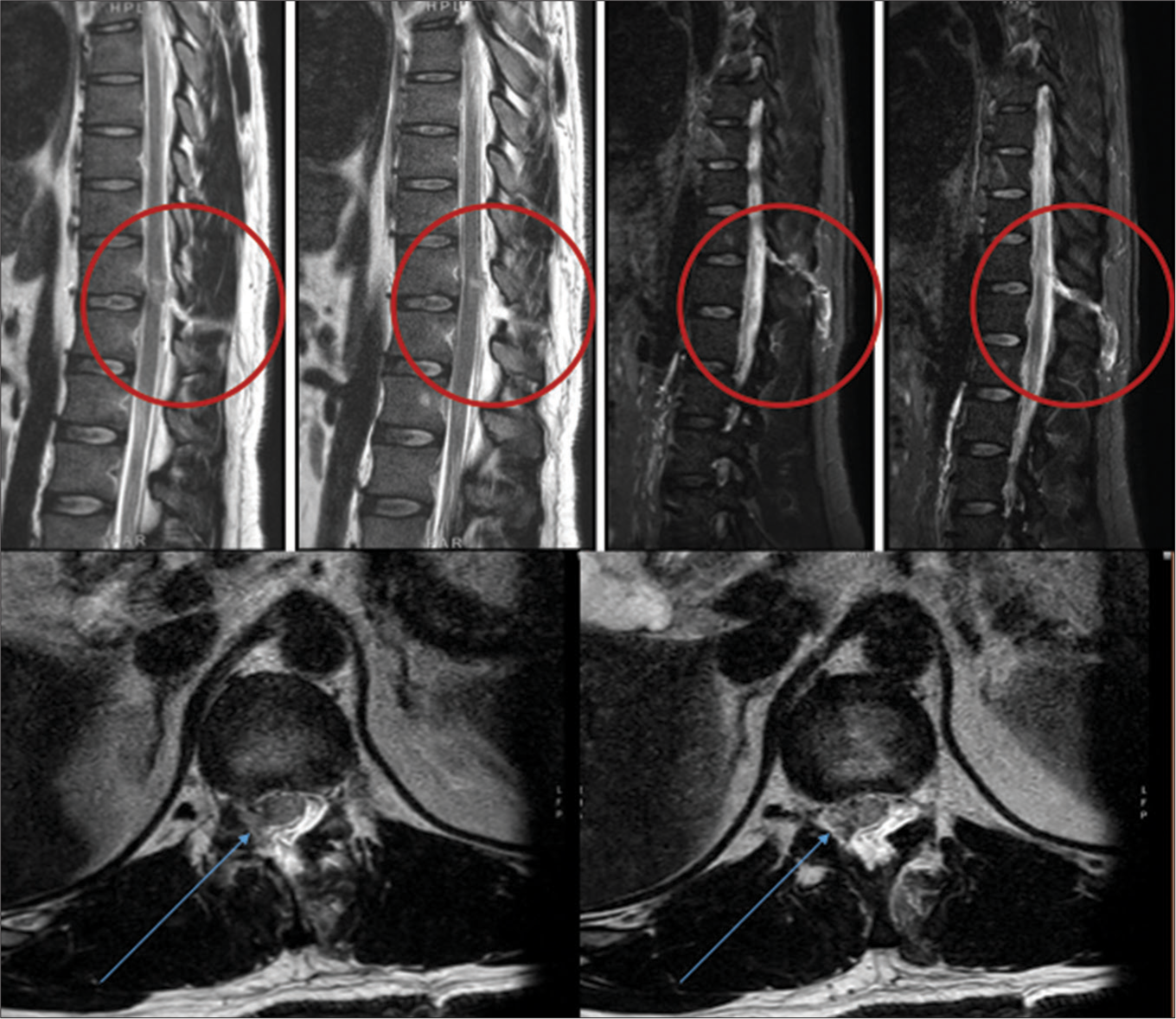
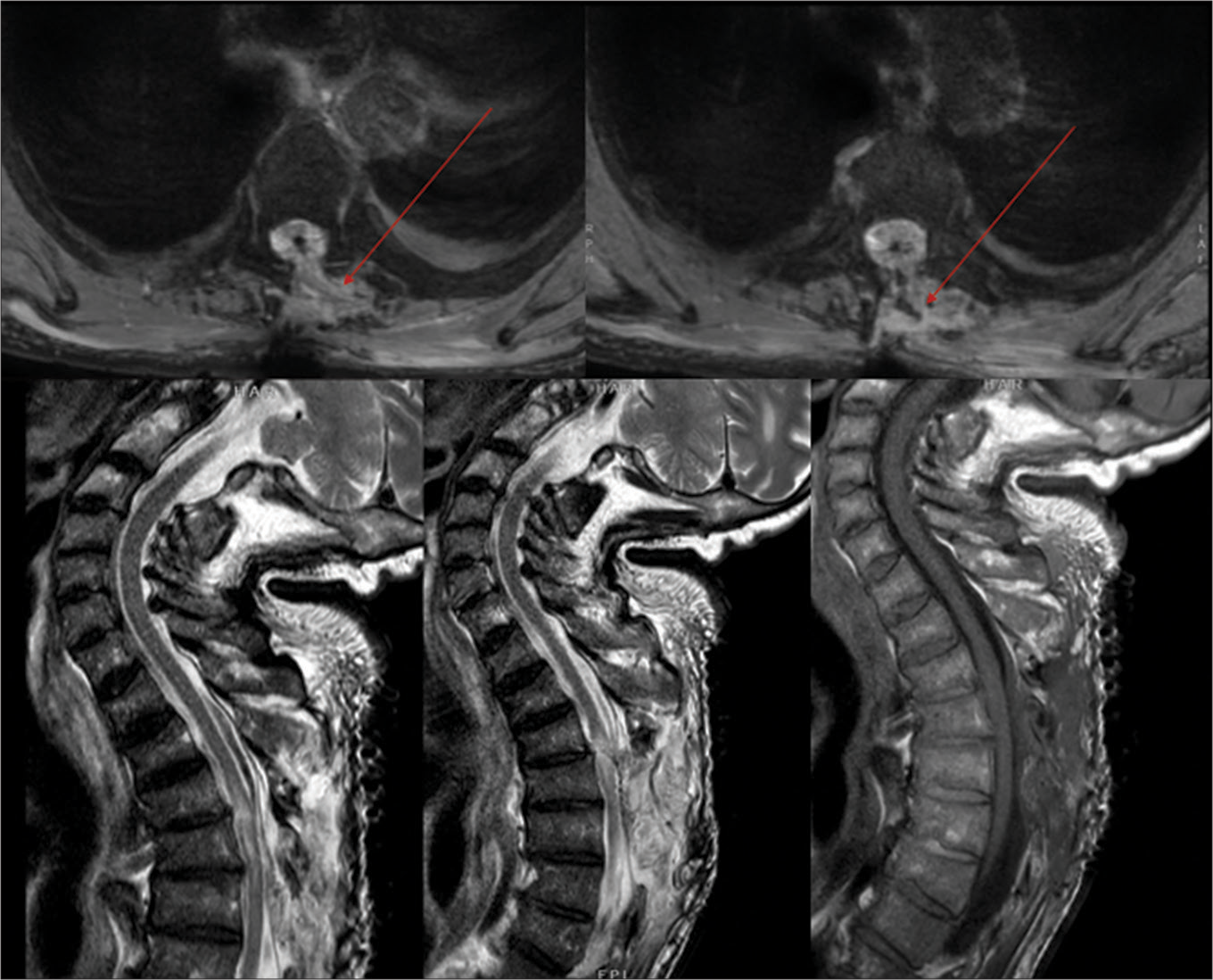
Figure 4:
Spinal magnetic resonance imaging of patient 2, sagittal and axial scans. Red circles indicate the laceration of the yellow ligament and the interspinous ligament with signs of a cerebrospinal fluid fistula (hyperintensity in the short-tau inversion recovery sequences and a small fluid collection in the subcutaneous tissue). Blue arrows indicate the lesion on the posterior-lateral side of the thecal sac.
Surgery
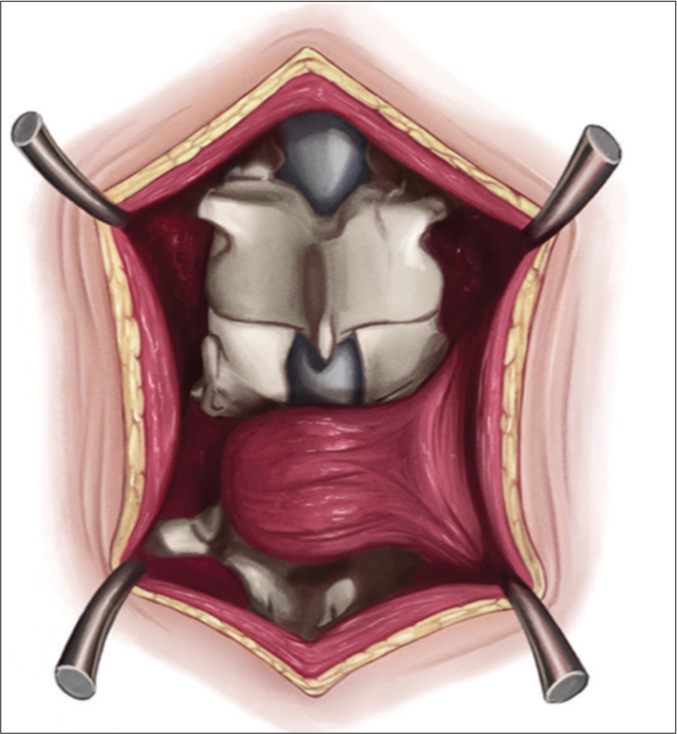
The bilateral D11 laminectomy documented multiple posterolateral/anterolateral nonsaturable dural lacerations and a minor spinal cord “tear.” Here, too, the dura was indirectly repaired by rotating pedicled multifidus muscle flaps [
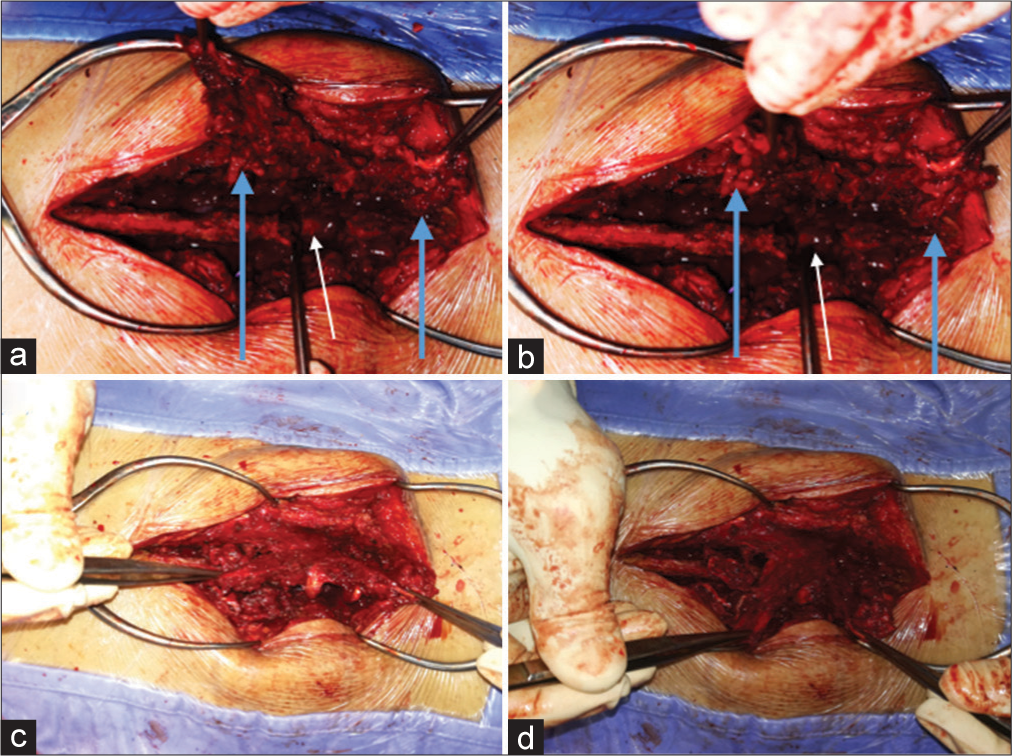
Figure 5:
Intraoperative pictures of patient 2 showing the harvesting of the pedicled multifidus muscle flap. (a and b) show the flap already harvested on the left side, with blue arrows indicating the cephalad and caudal extremities of the flap and a white arrow showing the exposed dura mater at the level of the laminectomy. (c and d) display the flap rotated to cover the dura mater, filling the laminectomy, with yellow arrows indicating the pedicle of the flap, which is attached at the level of the intertransverse space.
Postoperative course
Postoperatively, the patient’s right lower leg motor function improved, but the sensory deficit remained unchanged. He received a 7-day course of cefazolin. The postoperative MR and clinical examinations showed no recurrent CSF leak. Twelve days later, when the wound was fully healed, the patient was transferred to a rehabilitation unit. At six postoperative months, he qualified for the American Spinal Cord Injury Association (AIS) score of D (i.e., motor grade of at least three below the neurologic level of injury).
DISCUSSION
Dural repairs for penetrating spinal injuries, including multifidus muscle flaps
Conservative management of DT/CSF leaks risks wound infections, meningitis, septicemia, and death.[
Lack of success with spinal drain placement for these DT/CSF fistulas has included overdrainage, pneumocephalus, intracranial hemorrhages, and meningitis (i.e., 3–8%).[
CONCLUSION
Traumatic spinal cerebro spinal fluid (CSF) leaks/DT following penetrating spinal cord injuries may require indirect readily provided by utilizing pedicle multifidus muscle flaps.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of AI-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Brazdzionis J, Ogunlade J, Elia C, Wacker MR, Menoni R, Miulli DE. Effectiveness of method of repair of incidental thoracic and lumbar durotomies: A comparison of direct versus indirect repair. Cureus. 2019. 11: e5224
2. Carpenter H, Hurndall KH, Asokan AK, Fernandes R. Penetrating trauma causing cerebrospinal fluid leak without nerve root damage. BMJ Case Rep. 2018. 2018: bcr2017221461
3. Enicker B, Gonya S, Hardcastle TC. Spinal stab injury with retained knife blades: 51 Consecutive patients managed at a regional referral unit. Injury. 2015. 46: 1726-33
4. Epstein NE. Dural repair with four spinal sealants: Focused review of the manufacturers’ inserts and the current literature. Spine J. 2010. 10: 1065-8
5. Epstein NE. A review article on the diagnosis and treatment of cerebrospinal fluid fistulas and dural tears occurring during spinal surgery. Surg Neurol Int. 2013. 4: S301-17
6. Fiani B, Figueras RA, De Stefano F, Gautam N, Khan A, Soula M. Nonmissile penetrating spinal injuries: Mechanisms, expectations, and management. Surg Neurol Int. 2020. 11: 406
7. Kim JY, Oh BH, Kim IS, Hong JT, Sung JH, Lee HJ. The safety and effectiveness of lumbar drainage for cerebrospinal fluid leakage after spinal surgery. Neurochirurgie. 2023. 69: 101501
8. Kumar A, Pandey PN, Ghani A, Jaiswal G. Penetrating spinal injuries and their management. J Craniovertebr Junction Spine. 2011. 2: 57-61
9. Ozsoy KM, Menekse G, Okten AI, Guzel A. Cerebrospinal fluid fistula due to penetrating trauma. Indian J Neurotrauma. 2013. 10: 52-4
10. Policicchio D, Boccaletti R, Dipellegrini G, Doda A, Stangoni A, Veneziani SF. Pedicled multifidus muscle flap to treat inaccessible Dural tear in spine surgery: Technical note and preliminary experience. World Neurosurg. 2021. 145: 267-77
11. Policicchio D, Santonio FV, Boccaletti R, Giosuè D, Giampiero M, Adriana P. Flexible fiber CO2 laser in microsurgical treatment of intraventricular tumors: Usefulness and limitations. World Neurosurg. 2019. 122: e427-35

