

- Department of Neurosurgery, Faculty of Medicine, Zagazig University, Zagazig, Sharkia, Egypt.
- Department of Radiodiagnosis Faculty of Medicine, Zagazig University, Zagazig, Sharkia, Egypt.
- Department of ENT, Faculty of Medicine, Zagazig University, Zagazig, Sharkia, Egypt.
Correspondence Address:
Mohamed M. Arnaout
Department of Neurosurgery, Faculty of Medicine, Zagazig University, Zagazig, Sharkia, Egypt.
DOI:10.25259/SNI_472_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Mohamed M. Arnaout1, Ahmed A. Bessar2, Ismail Elnashar3, Hassan Abaza1, Mansour Makia1. Pituitary adenoma surgeries in COVID-19 era: Early local experience from Egypt. 29-Oct-2020;11:363
How to cite this URL: Mohamed M. Arnaout1, Ahmed A. Bessar2, Ismail Elnashar3, Hassan Abaza1, Mansour Makia1. Pituitary adenoma surgeries in COVID-19 era: Early local experience from Egypt. 29-Oct-2020;11:363. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=10360
Date of Submission
27-Jul-2020
Date of Acceptance
23-Sep-2020
Date of Web Publication
29-Oct-2020
Abstract
Background: The pandemic of COVID-19 has a great impact on all health-care services worldwide. Neurosurgical recommendations are to postpone the endoscopic endonasal pituitary surgeries during the pandemic. We would like to express our experience with urgent pituitary adenomas during the current COVID-19 pandemic.
Methods: In our country, COVID-19 has started to become a paramount problem by March 2020. Nine cases of pituitary adenomas have presented with urgent manifestations. The endoscopic endonasal approach was performed in eight patients, while a craniotomy was selected for a recurrent pituitary adenoma. Pre- and postoperative thorough clinical evaluations with chest CT scans were performed. Other strict infection control measures have been applied.
Results: In 8 weeks duration starting from the past days of February 2020, we have operated on four females and five males of pituitary adenomas. Visual deterioration was the main presenting symptom. The driving factor for surgery was saving vision in eight patients. Fortunately, the postoperative course was uneventful for all patients. No suspected COVID-19 infection has been reported in any patient or health-care team except one patient. In our city, PCR test was routinely not available.
Conclusion: In the era of COVID-19, strict infection control precautions should be employed to limit the possibility of transmission of any possible infection to patient or any of the surgical team. We believe that the risk of getting such infection is not increased by the endonasal approach. Long-term follow-up and large numbers of prospective studies are recommended to delineate the impact of COVID-19 infection on pituitary surgeries.
Keywords: COVID-19, Craniotomy, Endoscopic, Endonasal, Pituitary
INTRODUCTION
The pandemic of COVID-19 (or sometimes referred to as SARS-CoV-2) has a great impact on all health-care services worldwide. The elective surgical procedures have been suspended in many countries. There are some reports that the ENT surgeons are at higher risk for such infection because of high viral load in the nasopharynx.[
The recommendations of neurosurgery and skull-base societies were in cope with limiting the endoscopic endonasal approach only for urgent pituitary surgeries. Furthermore, they recommend using the craniotomy whenever possible for pituitary lesions. Most hypophysis tumors are slowly-growing lesions, so observation is possible in patients with stable pituitary tumors. This can be employed by regular radiological imaging and visual assessment plus medical treatment for secreting adenomas.[
Most of pituitary tumors are benign accounting for about 10–15% of all brain tumors. These tumors are mostly slowly-growing so small proportion of patients need urgent intervention.[
According to our experience, we are not suggesting craniotomy for midline pituitary adenomas. We have an experienced team for endoscopic endonasal approach tailoring experienced ENT and neurosurgeons. We would like to express our experience with the urgent pituitary adenomas during the current COVID-19 pandemic.
MATERIALS AND METHODS
In our country, COVID-19 has started to become a paramount problem by March 2020. During these times, nine cases of pituitary adenomas have presented with urgent manifestations to preclude any delay for intervention. We have operated on five males and four females who presented to our facility.
The endoscopic endonasal approach was performed in eight patients, while a craniotomy was selected for a recurrent pituitary adenoma that was previously operated by frontolateral approach 8 years ago. In the former patient, we used the same approach.
Before the endoscopic endonasal approach, a thorough history taking was asked especially for any recent fever, anosmia, new cough, any chest related problem, and any self-isolation status. A complete laboratory for all patients was done including routine preoperative blood tests in addition to HIV, HBV, and HCV markers. A chest CT scan was ordered 2 h before surgery. Further investigations were not indicated at that time because the provisional diagnosis of COVID-19 was clinical and CT chest is of high diagnostic value. Furthermore, PCR was not available in our city.
In the operating room, strict infection control precautions have been considered. Every surgical team has been asked to wear one surgical mask plus N95 on top in addition to face shields.[
Postoperative care was delivered in the usual manner plus some precautions. In the intensive care unit, very special attention was paid for any chest or upper airway problem. Special partition in was prepared away from other patients both in intensive care unit and the ward. CBC in the second day was looked for to exclude any abnormalities related to COVID.
Before discharge from hospital, all cases had careful examination for any airway difficulties, cough, fever, and chest CT scans were obtained. Nasopharyngeal swab was considered if any suspicious for any abnormality related to COVID. Of note, it was not available in our city. In our facility, PCR (polymerase chain reaction) was not considered in any patient except if clinically indicated. Furthermore, the Egyptian ministry of health protocol was limiting the PCR test to those of high clinical suspension.[
All patients were followed on regular basis using phone calls, limiting the clinic visit to the 3-month MRI.
RESULTS
In 8 weeks duration starting from the past days of February 2020, we have operated on nine consecutive emergencies of pituitary adenomas. Four females and five males were operated on. The visual deterioration was the main presenting symptom. The other presenting symptoms with the demographic data are presented in
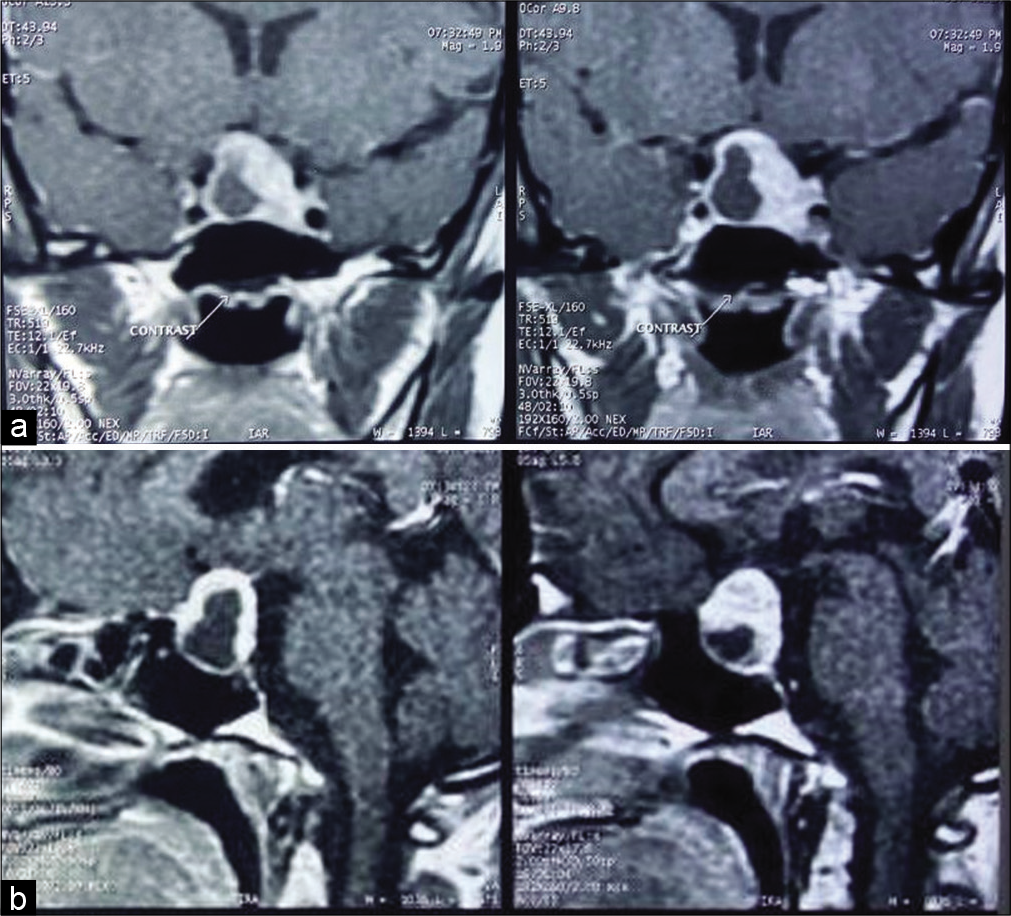
Figure 1:
(Case 5) (a) Two images of coronal section of contrast-enhanced T1WI MRI showing pituitary apoplexy in the form of necrotic cystic part surrounded by homogenous enhancement of fleshy part of the histopathologically confirmed pituitary adenoma. The tumor is pushing the optic chiasm upwards. (b) Two images of sagittal section of contrast-enhanced T1WI MRI showing the sellar and suprasellar two tumor components.
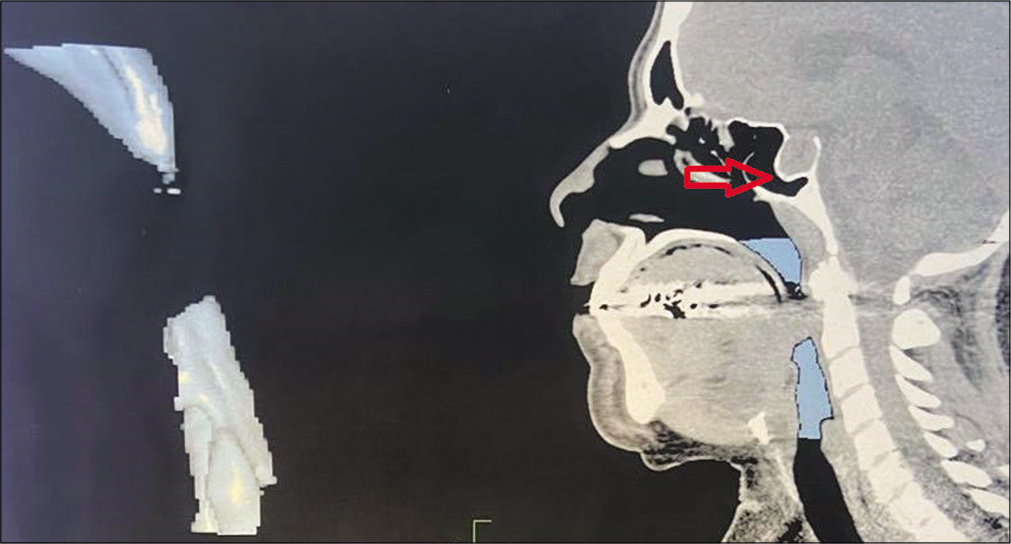
Figure 2:
(Case 3) Non-enhanced CT reformatted mid-sagittal image of the pharyngx, clivus, and sella showing swelling of the back of the tongue obstructing the airway in a patient of growth hormone secreting adenoma. The hollow red arrow points to the expansion of the sellar region by the pituitary adenoma. The well pneumatized sphenoid sinus encourages the endoscopic endonasal approach.
The endoscopic endonasal was performed in all patients except one because it is considered the gold-standard approach for midline adenomas. Frontolateral approach was selected in the recurrent case because we believe the transcranial approach is more save in the time of COVID-19.
During history taking, all patients and relatives have denied any symptom of recent fever, anosmia, cough, and any chest related problem. No self-isolation has been reported. Chest CT scans ordered for every case 2 h before surgeries were normal [
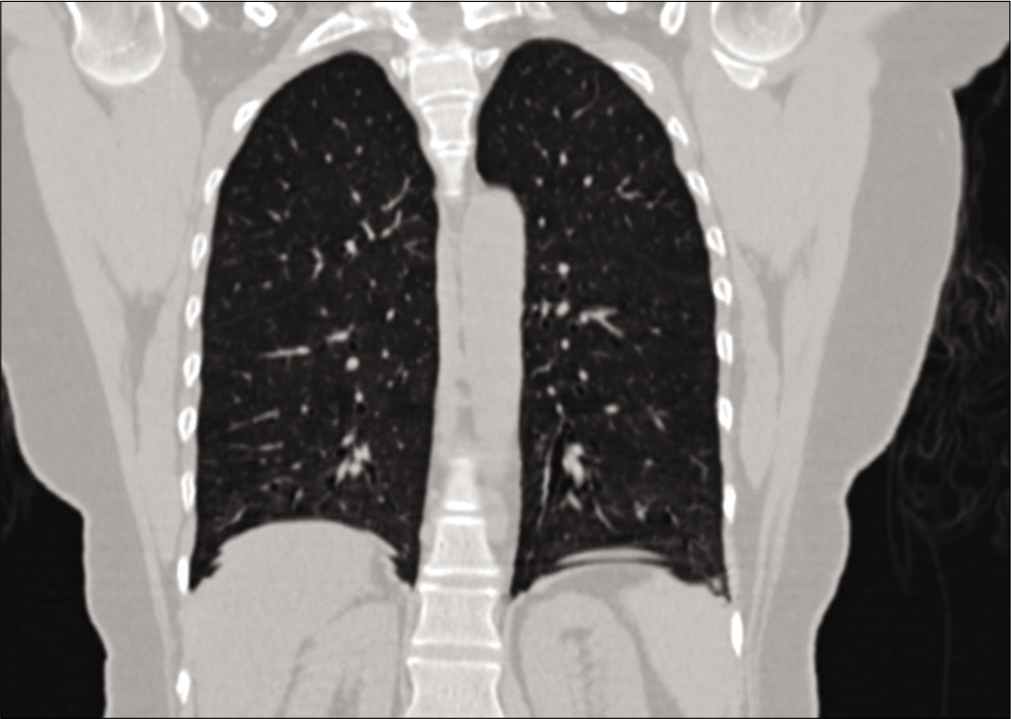
Figure 3:
Preoperative chest CT scan with coronal reformat (identical or alternative to chest X-ray in case of limited resources). This CT scan was performed 2 h before surgery to exclude any abnormality (case 5). As long as there is no suspicion of COVID-19, no further investigations were necessary.
In postoperative day 2, all our cases had an uneventful recovery in the ward without any significant complication except some CSF leak in two patients (cases 7 and 9) which had been stopped with the conservative measures.
The operative and postoperative courses were nontedious for COVID-19 except in one patient (case 3) who developed postoperative anosmia. In this particular case, the transseptal endoscopic endonasal approach was tailored because of the profound nasal septum deviation. This anosmia was not associated with any fever, cough, or any COVID-19 related symptoms. It started to improve after 2 weeks from surgery. In this particular case, a CT chest and other laboratory markers were obtained which were normal. We send her for nasopharyngeal swab and PCR. The initial and the repeated test after 48 h were negative.
As long as the postoperative course was without complications, no nasopharyngeal swab or PCR for COVID-19 were ordered except for one. Chest CT scans for every patient were free just before discharge from hospital. All patients were followed over the phone without reporting any problem related to surgery or COVID-19. The average follow-up was 2 months.
DISCUSSION
In the early 2020, a new virus has been reported in China. It spread gradually to all over the world. On January 30, the ongoing pandemic of COVID-19 has been announced by the WHO as public health emergency of international concern.
Many of the properties of this new virus were unknown. This, in turn, has a great psychological burden on the health-care providers.[
The recommendations for neurosurgical procedures were established by neurosurgical and skull base societies during the COVID-19 pandemic. It was recommended to postpone all endoscopic endonasal approaches aiming at reducing the possible spread of COVID-19 infection. The exception for endonasal was the midline pituitary adenomas which cannot be approached by craniotomy sufficiently. This was because the viral load is high in the nasopharynx. Trans-cranial surgeries were allowed with moderation. Strict infection control precautions were recommended in both.[
In December 2019, a case has been reported from China of a patient who developed symptoms of COVID-19 after endoscopic endonasal approach for pituitary adenoma surgery. In this patient, the postoperative fever was expected to be due to postoperative CSF leak and associated infection. A newly developed cough was the clue for more investigation of this fever of unknown origin. Later on, he passed away after 1 month from surgery due to respiratory failure. The 14 staffs that were associated with his care were diagnosed positive for COVID-19. All of them were reported to recover completely. Apart from this case report, up to date no cases reported worldwide to develop COVID-19 after the endonasal approach. This particular patient had the COVID-19 infections before surgery. The incubation period for COVID-19 has been reported to start from few days up to 2 weeks. In our opinion, meticulous preoperative evaluation and chest X-ray could be the cutoff suspicion for COVID-19 if appropriately achieved for preoperative diagnosis. We did not proceed for further investigations in our cases because it was clinically not indicated. Furthermore, at the time of our surgeries the COVID-19 was new in Egypt.[
The dilemma of diagnosis of COVID-19 is still not well established. Although PCR of nasopharyngeal swab is considered the most appropriate test, yet false results have been reported. Therefore, two separate negative tests should be performed in case of suspension to increase the sensitivity. Different gene targets were investigated for PCR. They are varying from country to another with different accuracy profiles.[
In one report from The Mount Sinai Department of Neurosurgery, they have operated on two cranial and one spine emergencies during COVID-19 pandemic. In their first case of frontoparietal mass, a chest X-ray was abnormal. This patient was managed as COVID-19 despite coronavirus nasopharyngeal swab testing was negative. In the second case of suspected large pituitary adenoma, a ventriculoperitoneal shunt was inserted to alleviate hydrocephalus. No PCR nasopharyngeal swab testing was done.[
In our cases, we devoted for frontolateral approach in only one recurrent case (case 1) of pituitary adenoma because we believe in this early experience it will be safer than the endonasal approach because of the reported recommendations of limiting the elective endoscopic neurosurgical practice.[
The direct spread from the nasopharynx to the surgeon or the nursing staffs has never been documented. During the endoscopic endonasal approach, it is rarely that droplets or blood escape from the nostril to outside. This is because we usually use two suction tubes with regular cleaning of the surgical field for better visualization. In such way, airborne or droplet possible spread of COVID-19 will be extremely difficult. In agree with the reported case of COVID-19 after endonasal approach, we believe that the strict infection control measures to be applied for any endonasal endoscopic surgeries with no need to postpone. This should include the personal protective measures for patient and surgical team as well as the negative pressure operating rooms.[
In a meta-analysis, the face mask and N95 respirators were considered equal in protection from COVID-19 in general healthcare. However, N95 was recommended for high risk surgical procedures with possible aerosol generation. In our study, we use both to augment protection because of the low evidence for each at that time.[
We think that coincidence of COVID-19 and endonasal approach is overrated because the spread of COVID-19 is limited to case report. The natural history of the disease is the profound factor of spread, progression, or regression. The endonasal approach has no role in increasing spread other than the natural spread of COVID-19. Intraoperative droplets and aerosols in the endonasal approach can be limited using two suction systems and avoid using bone drilling or tissue debriders. Given the intranasal working channel, the spread outside nose should be very confined.
For elective pituitary surgeries during COVID-19, we believe more prospective studies are advised taking into consideration the impact of possible postoperative electrolyte imbalance or hypopituitarism on the immune system.[
We have established a management algorithm applied for urgent pituitary adenoma surgeries in setting of limited resources for nonsuspected COVID-19 patients [
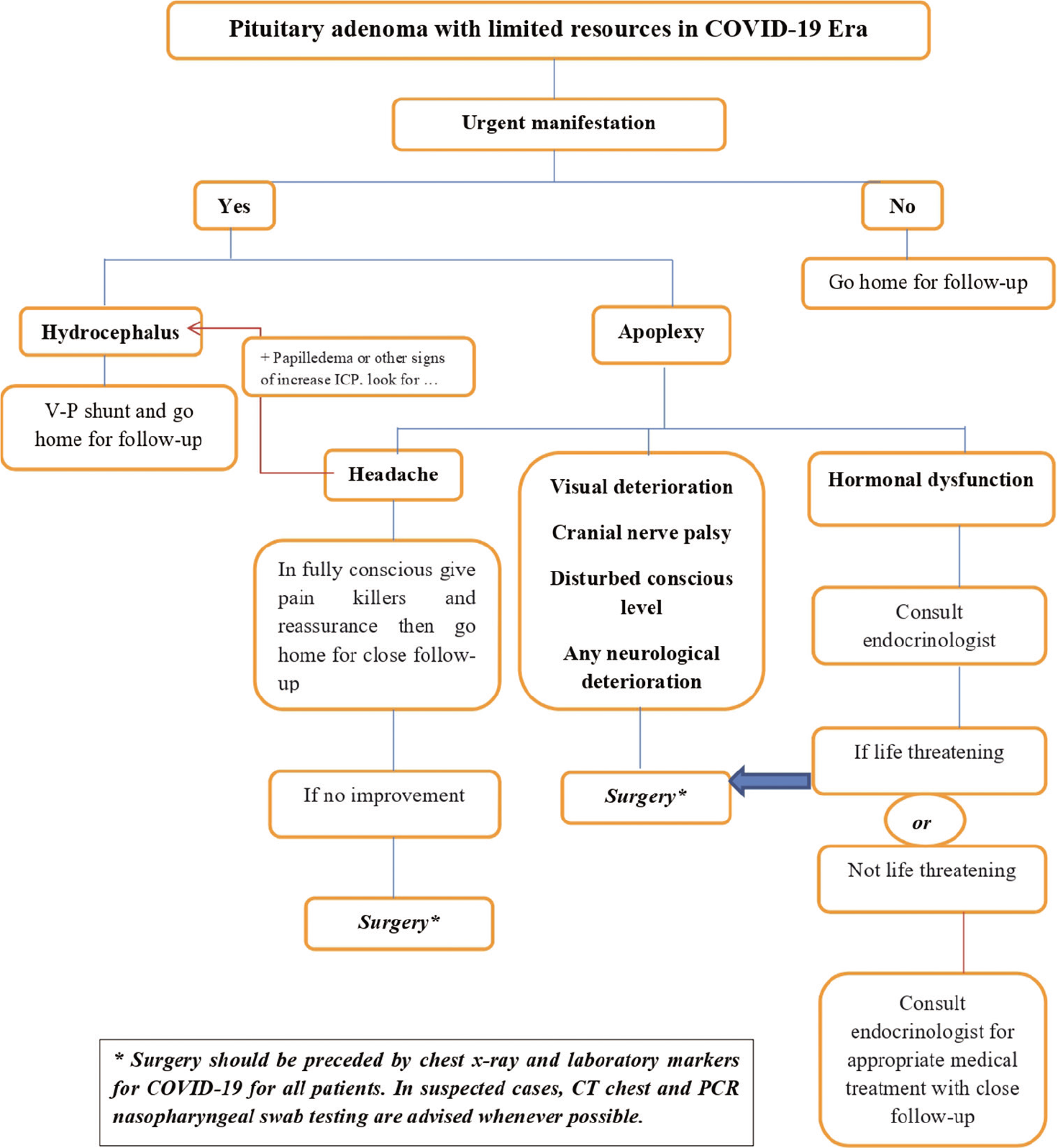
Figure 4:
The management algorithm applied for urgent pituitary adenoma surgeries in setting of limited resources for nonsuspected COVID-19 patients. The same algorithm can be applied after proper COVID-19 testing and proper diagnosis. The close follow-up means regular radiological imaging and visual assessment plus medical treatment for secreting adenomas.
The main limitations of our study were the unavailability of preoperative PCR testing and small number of cases. It should not be sufficient to conclude recommendations. However, given the lack knowledge for endonasal approach in COVID-19 era, we believe our study provides some background for scientists and clinicians conducting research in this area of interest. Some reports have confirmed that CT chest is superior to PCR testing for COVID-19 diagnosis. In a study of 1014 patients, CT chest was confirmed to be more sensitive than PCR testing. In this study, 60–93% of patients had positive CT chest scans consistent with COVID-19 before (or parallel to) the first positive PCR results. Furthermore, 42% of patients had negative CT chest before PCR turned negative. This study concluded that CT chest can be used as a primary tool for diagnosis of COVID-19.[
CONCLUSION
In the era of COVID-19, strict infection control precautions should be employed to limit the possibility of transmission of any possible infection to patient or any of the surgical team. We believe that the risk of getting such infection is not increased by the endonasal approach. Long-term follow-up and large numbers of prospective studies are recommended to delineate the impact of COVID-19 infection on pituitary surgeries, especially the endonasal approach.
Declaration of patient consent
Patient’s consent not obtained as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Ai T, Yang Z, Hou H, Zhan C, Chen C, Lv W. Correlation of chest CT and RT-PCR testing for coronavirus disease 2019 (COVID-19) in China: A report of 1014 cases. Radiology. 2020. 296: E32-40
2. Arnaout MM, Gerges MM, Cummock MD, El Asri AC, Greenfield JP, Anand VK. Endonasal surgery for suprasellar germ cell tumors: Two cases and review of the literature. Acta Neurochir (Wien). 2019. 161: 1699-704
3. Bamps S, Roosen G, Vanvolsem S, Wissels M, Put E, Duyvendak W. Even with COVID-19 neurosurgeons should still perform necessary urgent/emergent neurosurgery to avoid major permanent neurological deficits. Surg Neurol Int. 2020. 11: 75
4. Bartoszko JJ, Farooqi MA, Alhazzani W, Loeb M. Medical masks vs N95 respirators for preventing COVID-19 in healthcare workers: A systematic review and meta-analysis of randomized trials. Influenza Other Respir Viruses. 2020. 14: 365-73
5. . Available from: https://www.ecmoexperts.com/covid-19-resources-egyptian-diagnosis-treatment [Last accessed on 2020 Jul 21].
6. Dolecek TA, Propp JM, Stroup NE, Kruchko C. CBTRUS statistical report: Primary brain and central nervous system tumors diagnosed in the United States in 2005-2009. Neuro Oncol. 2012. 14: v1-49
7. Gao Y, Zhong C, Wang Y, Xu S, Guo Y, Dai C. Endoscopic versus microscopic transsphenoidal pituitary adenoma surgery: A meta-analysis. World J Surg Oncol. 2014. 12: 94
8. Hassan HA, Bessar MA, Herzallah IR, Laury AM, Arnaout MM, Basha MA. Diagnostic value of early postoperative MRI and diffusion-weighted imaging following trans-sphenoidal resection of non-functioning pituitary macroadenomas. Clin Radiol. 2018. 73: 535-41
9. Hassany M, Abdel-Razek W, Asem N, AbdAllah M, Zaid H. Estimation of COVID-19 burden in Egypt. Lancet Infect Dis. 2020. 20: 896-7
10. Kessler RA, Zimering J, Gilligan J, Rothrock R, McNeill I, Shrivastava RK. Neurosurgical management of brain and spine tumors in the COVID-19 era: An institutional experience from the epicenter of the pandemic. J Neurooncol. 2020. 148: 211-9
11. Kolias A, Tysome J, Donnelly N, Sharma R, Gkrania-Klotsas E, Budohoski K. A safe approach to surgery for pituitary and skull base lesions during the COVID-19 pandemic. Acta Neurochir (Wien). 2020. 162: 1509-11
12. Lauer SA, Grantz KH, Bi Q, Jones FK, Zheng Q, Meredith HR. The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: Estimation and application. Ann Intern Med. 2020. 172: 577-82
13. Lo YT, Teo NW, Ang BT. Editorial. Endonasal neurosurgery during the COVID-19 pandemic: The Singapore perspective. J Neurosurg. 2020. 1: 1-3
14. Mukherjee A, Helbert M, Davis J, Shalet S. Immune function in hypopituitarism: Time to reconsider?. Clin Endocrinol (Oxf). 2010. 73: 425-31
15. Patel ZM, Fernandez-Miranda J, Hwang PH, Nayak JV, Dodd R, Sajjadi H. Letter: Precautions for endoscopic transnasal skull base surgery during the COVID-19 pandemic. Neurosurgery. 2020. 87: E66-7
16. Ramakrishna R, Zadeh G, Sheehan JP, Aghi MK. Inpatient and outpatient case prioritization for patients with neuro-oncologic disease amid the COVID-19 pandemic: General guidance for neuro-oncology practitioners from the AANS/CNS tumor section and society for neuro-oncology. J Neurooncol. 2020. 147: 525-9
17. Rothe C, Schunk M, Sothmann P, Bretzel G, Froeschl G, Wallrauch C. Transmission of 2019-nCoV infection from an asymptomatic contact in Germany. N Engl J Med. 2020. 382: 970-1
18. Schaller K. Neurosurgeons in the corona crisis: Striving for remedy and redemption. A message from the president of the EANS. Acta Neurochir (Wien). 2020. 162: 1217-9
19. Vukkadala N, Qian ZJ, Holsinger FC, Patel ZM, Rosenthal E. COVID-19 and the otolaryngologist: Preliminary evidence-based review. Laryngoscope. 2020:
20. Coronavirus Disease (COVID-19) Outbreak. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019. [Last accessed on 2020 Jul 21].
21. Zhu W, Huang X, Zhao H, Jiang X. A COVID-19 patient who underwent endonasal endoscopic pituitary adenoma resection: A case report. Neurosurgery. 2020. 87: E140-6

