

- Department of Neurosurgery, Nara Medical University Hospital, Kashihara, Nara, Japan
- Department of Orthopedics, Nara Medical University Hospital, Kashihara, Nara, Japan
- Department of Radiation, Nara Medical University Hospital, Kashihara, Nara, Japan
Correspondence Address:
Yasuhiro Takeshima
Department of Neurosurgery, Nara Medical University Hospital, Kashihara, Nara, Japan
DOI:10.4103/sni.sni_57_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Yasuhiro Takeshima, Hideki Shigematsu, Kengo Konishi, Ichiro Nakagawa, Yasushi Motoyama, Hiroyuki Nakase. Posterior atlantoaxial fusion using a C2 transverse foramen-penetrating screw: A technical note. 24-Oct-2017;8:262
How to cite this URL: Yasuhiro Takeshima, Hideki Shigematsu, Kengo Konishi, Ichiro Nakagawa, Yasushi Motoyama, Hiroyuki Nakase. Posterior atlantoaxial fusion using a C2 transverse foramen-penetrating screw: A technical note. 24-Oct-2017;8:262. Available from: http://surgicalneurologyint.com/surgicalint-articles/posterior-atlantoaxial-fusion-using-a-c2-transverse-foramen%e2%80%91penetrating-screw-a-technical-note/
Date of Submission
05-Feb-2017
Date of Acceptance
05-Mar-2017
Date of Web Publication
24-Oct-2017
Abstract
Background:Although recent development of screw instrumentation techniques for rigid fixation of the atlantoaxial joint has increased surgical options, patients in whom screws of any type cannot be safely placed are sometimes encountered. We present a unique surgical technique for C1-2 transarticular screw placement utilizing a novel trajectory.
Methods:A 35-year-old male with a history of Down's syndrome and cognitive dysfunction with hyperkinesis spontaneously developed rapid onset of tetraparesis and gait disturbance. Radiographs of the cervical spine revealed atlantoaxial subluxation (AAS) that could not be reduced. Computed tomography (CT) of the head showed multiple subacute cerebral infarctions in the territory of the right vertebral artery (VA). Three-dimensional CT angiography of the craniovertebral junction additionally confirmed right VA occlusion at the C2/3 level, a left C2 origin of the posterior inferior cerebellar artery, and hypoplasia of the bilateral C2 pedicles/C2 lamina. Because traditional screw-placement was not feasible, we performed a unique atlantoaxial fusion utilizing a C2 transverse foramen-penetrating screw with iliac bone grafting performed under neuronavigation.
Results:The postoperative course was uneventful, and the patient regained the ability to ambulate, returning to his previous level of function. The CT of the cervical spine 12 months postoperatively showed rigid bony C1-C2 fusion, without recurrence of stroke.
Conclusion:We introduced a novel C1-C2 transarticular screw-placement technique in which the trajectory went through the ipsilateral VA foramen due to already extent VA occlusion.
Keywords: Atlantoaxial, Down's syndrome, posterior fusion, transverse foramen, vertebral artery occlusion
INTRODUCTION
Destruction of the atlantoaxial junction potentially impairs spinal cord function and vertebral artery (VA) compromise,[
Here, we describe a novel trajectory for atlantoaxial transarticular screw placement in a patient with unilateral VA occlusion.
CASE REPORT
A 35-year-old male with Down syndrome and hyperkinesis rapidly became tetraparetic. Cervical radiographs revealed atlantoaxial subluxation (AAS) [Figure
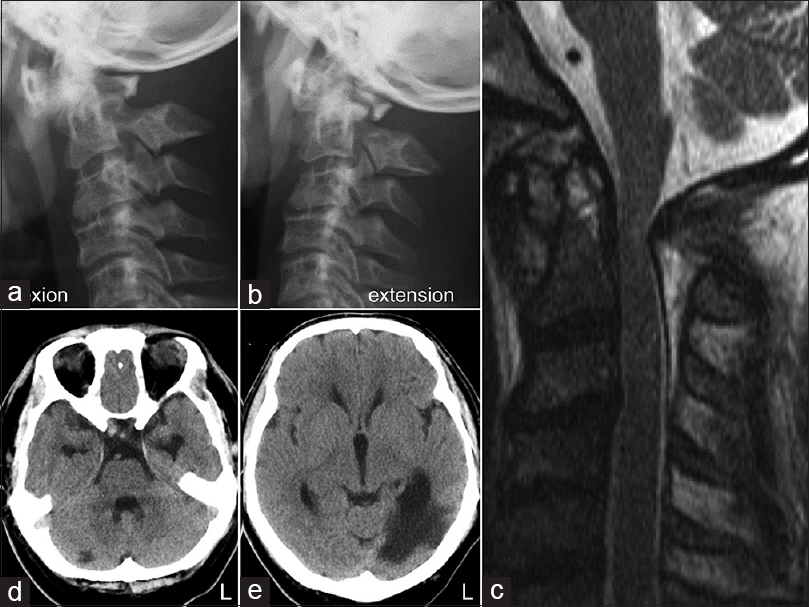
Figure 1
Initial radiographical examinations. (a and b) Dynamic lateral radiographs of the cervical spine in flexion (a) and extension (b) positions showing AAS without complete reduction of the atlantoaxial joint. (c) Preoperative sagittal T2-weighted MRI of the cervical spine showing cervical canal stenosis with intramedullary signal change at the C1 level. (d and e) Axial CT images of the brain. Low-density areas in the right superior cerebellar artery area (d) and in the left posterior cerebral artery area (e) indicate subacute infarctions
Three-dimensional CT angiography (3D-CTA) showed a complete right VA occlusion at the C2/3 level, a left C2 origin of the posterior inferior cerebellar artery (PICA), and hypoplasia of the bilateral C2 pedicles and C2 lamina [Figure
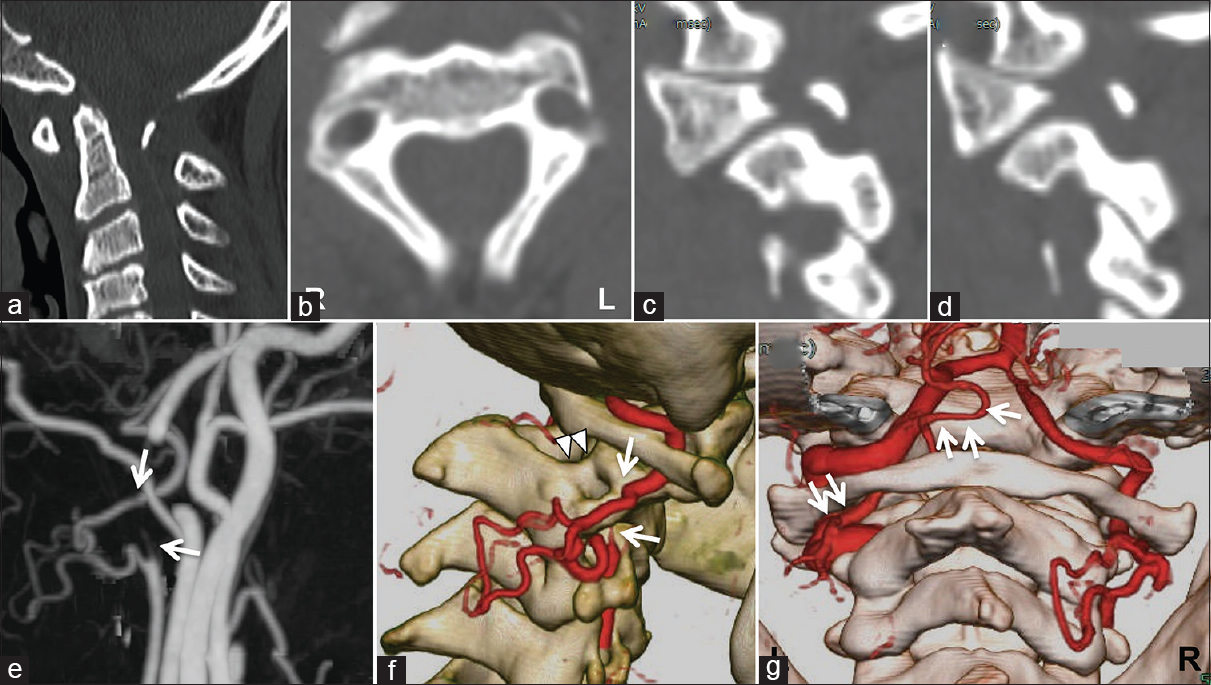
Figure 2
Preoperative CT and 3D-CTA images. (a) Sagittal image demonstrating AAS and significant atrophic posterior arch of the axis. (b-d) CT mages demonstrating hypoplasia of the right (c) and left (d) C2 pedicles and the rather thin C2 lamina. (e and f) 3D-CTA images showing complete regional occlusion of the right VA at the C2 transverse foramen with collateral flow (arrows indicating occlusion borders) and hypoplasia of the right C2 pedicles (arrowheads). (g) 3D-CTA image showing the laterality of the VAs and the left C2 origin of the PICA (arrows)
Because traditional screw-placement techniques could not be utilized, the atlantoaxial fusion involved placing a C2 transverse foramen-penetrating screw was accomplished.
Modified surgical technique
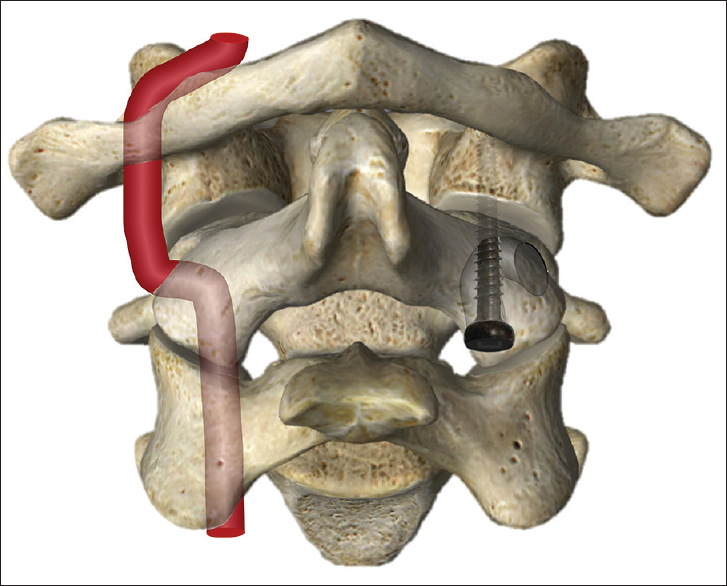
Subsequent to C1 laminectomy, a right atlantoaxial transarticular screw was inserted, aided by neuronavigation using a unique trajectory through the C2 transverse foramen. Although the screw was placed in the same direction as a standard atlantoaxial transarticular screw, a lateral entry point was utilized to penetrate the transverse foramen. A left C1 lateral mass screw was then placed under the special attention to the left C2 origin of PICA with the partial drilling of the C2 vertebral body. Finally, a C2 interlaminar screw placement, rod connection, and iliac bone grafting were performed.
The postoperative course was uneventful. Cervical X-rays showed adequate bilateral atlantoaxial screw placement [Figure
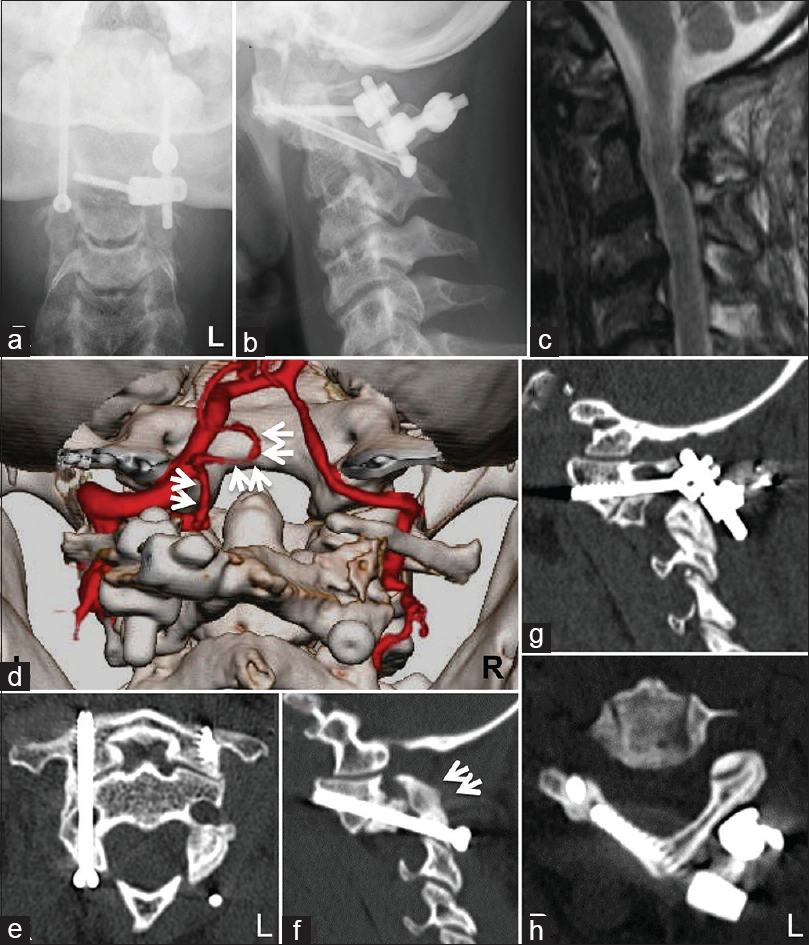
Figure 3
Postoperative radiographical examinations. (a and b) Anteroposterior and lateral view of cervical radiographs showing on-target atlantoaxial screw placements. (c) Sagittal T2-weighted MRI of the cervical spine showing decompression of the spinal cord at the C1 level. (d) Posterior view of reconstructed 3D-CTA image at the craniovertebral junction showing a patent left PICA (arrows). (e-h) CT images at the 12-month follow-up showing the trajectory of each screw and bony fusion between C1 and C2 (arrows)
DISCUSSION
New techniques for the atlantoaxial fixation
The atlantoaxial transarticular screw technique provides rigid fixation and high fusion rates, however, is technically demanding due to the proximity of the VAs. C1 lateral mass screws and C2 pedicle/pars screws[
Unique fusion technique
Rigid internal fixation was needed in this case as the patient exhibited hyperkinesis. However, traditional C1-C2 screw placement was not feasible in this case due to the multiple congenital anomalies. Therefore, we had to develop a novel trajectory for screw insertion. Because this patient already had a complete unilateral occlusion of VA, a screw could be uniquely and safely placed traversing the ipsilateral C2 transverse foramen [
CONCLUSION
Here, we introduced the novel C1-C2 transarticular screw-placement technique in a patient in whom the ipsilateral VA was already completely occluded.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Ebraheim N, Rollins JR, Xu R, Jackson WT. Anatomic consideration of C2 pedicle screw placement. Spine. 1996. 21: 691-5
2. Harms J, Melcher RP. Posterior C1-C2 fusion with polyaxial screw and rod fixation. Spine. 2001. 26: 2467-71
3. Takeshima Y, Matsuda R, Hironaka Y, Motoyama Y, Nakase H. Rheumatoid arthritis-induced lateral atlantoaxial subluxation with multiple vertebrobasilar infarctions. Spine. 2015. 40: E186-9
4. Takeshima Y, Nishimura F, Park YS, Nakase H. Fusion surgery for recurrent cerebellar infarctions due to bilateral atlantoaxial rotational vertebral artery occlusion. Spine. 2014. 39: E860-3
5. Wright NM. Posterior C2 fixation using bilateral, crossing C2 laminar screws: Case series and technical note. J Spinal Disord Tech. 2004. 17: 158-62

