

- Department of Neurosurgery, National Institute of Mental Health and Neurosciences (NIMHANS), Bengaluru, Karnataka, India
Correspondence Address:
A. R. Prabhuraj
Department of Neurosurgery, National Institute of Mental Health and Neurosciences (NIMHANS), Bengaluru, Karnataka, India
DOI:10.4103/sni.sni_395_17
Copyright: © 2017 Surgical Neurology International This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Harsh Deora, A. R. Prabhuraj, Nupur Pruthi. Posterior epidural migration of lumbar disc: Will the real “disc” please stand up?. 18-Dec-2017;8:302
How to cite this URL: Harsh Deora, A. R. Prabhuraj, Nupur Pruthi. Posterior epidural migration of lumbar disc: Will the real “disc” please stand up?. 18-Dec-2017;8:302. Available from: http://surgicalneurologyint.com/surgicalint-articles/posterior-epidural-migration-of-lumbar-disc-will-the-real-disc-please-stand-up/
Date of Submission
25-Oct-2017
Date of Acceptance
09-Nov-2017
Date of Web Publication
18-Dec-2017
Abstract
Background:Posterior epidural lumbar disc fragment migration is rare and most commonly occurs at the L3-L4 level where it may contribute to cauda equina compression.
Case Description:Here, we report three cases of epidural migration of a lumbar disc, two of which led to bladder dysfunction/cauda equina compression. Early decompression (e.g., laminectomy) and aggressive postoperative physiotherapy led to significant postoperative improvement in all three patients.
Conclusion:Migration of large sequestrated lumbar disc herniations leading to cauda equina compression should be recognized early and promptly treated with decompressive laminectomies to achieve the best postoperative outcomes.
Keywords: Cauda equina, low back pain, lumbar disc, posterior epidural migration
INTRODUCTION
Posterior epidural migration of lumbar disc fragments (PEMLDF) is rare and typically occurs in middle-aged men at the L3-L4 level. There are only 78 cases reported in the literature, including the three from this study. Notably, 41 patients presented with an acute cauda-equina syndrome (CES) resulting in bladder dysfunction.
CASE REPORTS
Case 1
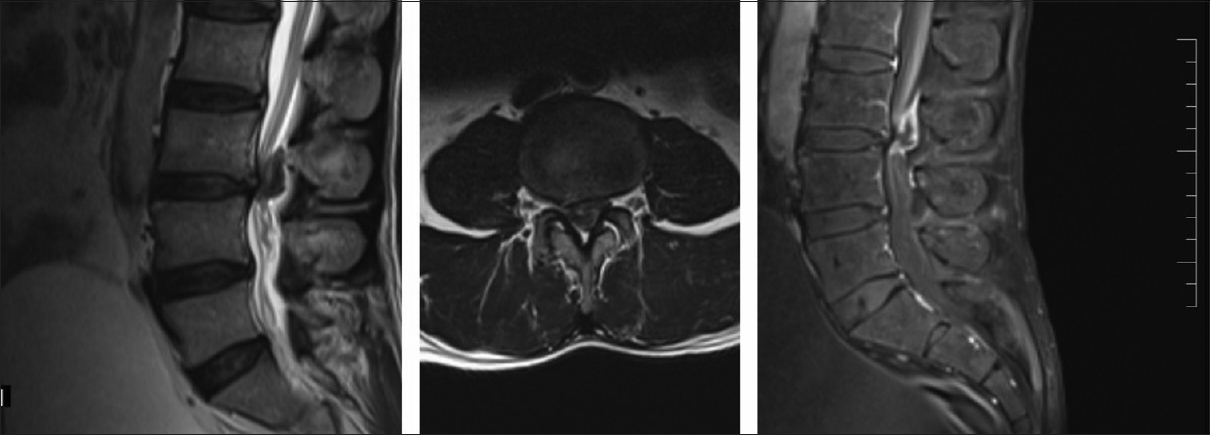
A 52-year-old male presented with a traumatic onset of right greater than left-side low back and leg pain of 3-years duration. However, he experienced increased onset of numbness, tingling, weakness, and urinary hesitancy over the last 3 weeks [

Case 2
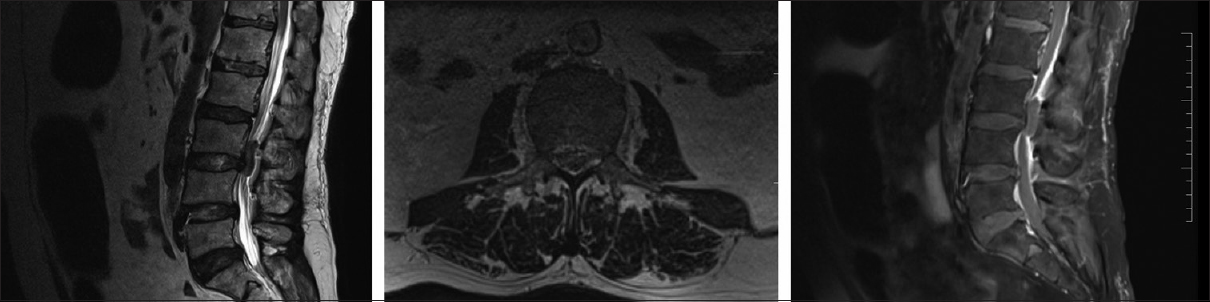
A 60-year-old male presented with 2-year history of back/bilateral leg pain accompanied by 7-day onset of urinary incontinence and 4 days of paraplegia [
Case 3
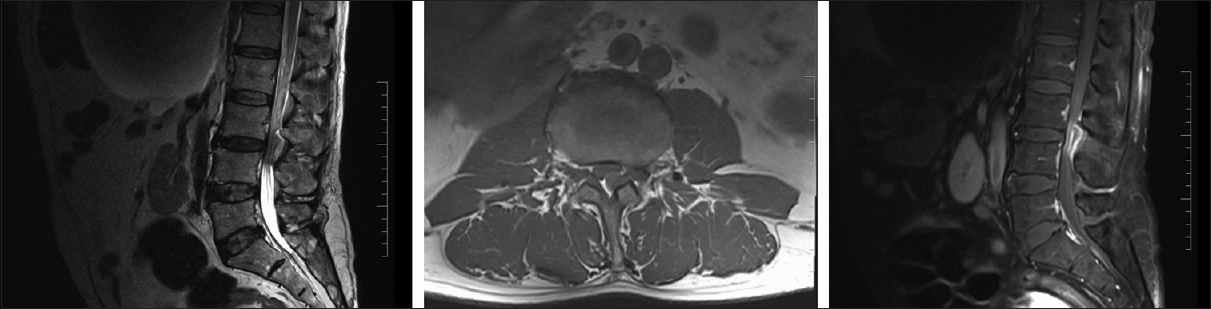
A 57-year-old male with a history of low back pain was unable to walk for the last 2 weeks [
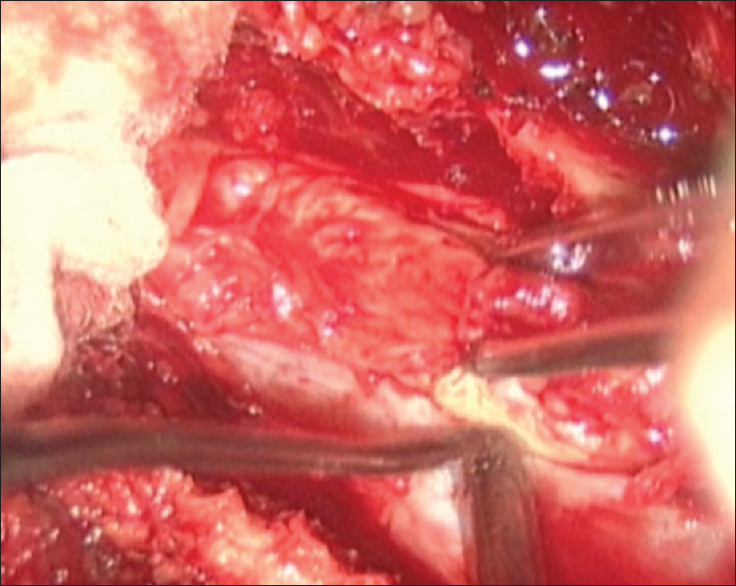
Summary of surgery
All three patients underwent L3 laminectomy and L3-4 discectomy without fusion [
DISCUSSION
PEMLDF is rare and typically appears in middle-aged males who perform heavy labor. They typically present with MR-documented L3-4 (39.2%) ventral sequestrated disc herniations (e.g., T1 iso/hypointense and T2 hyperintense with rim enhancement) resulting in cauda equina syndromes. Seventy-five cases have been reported in the literature; our cases brings this figure to 78.[
Treatment options
Urgent decompressive laminectomy and discectomy at the L3-L4 level without fusion addressed the cauda equina syndrome attributed to massive thecal sac and bilateral L4 root compression.[
CONCLUSION
Three patients with PEMLDF and large ventral sequestrated disc herniations that had migrated to the L3-4 level were treated with L3-L4 laminectomies/diskectomies without fusions. Early diagnosis and decompression correlated with better postoperative results and a greater chance of recovery of sphincter function.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that name and initial will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. El Asri AC, Naama O, Akhaddar A, Gazzaz M, Belhachmi A, El Mostarchid B. Posterior epidural migration of lumbar disk fragments: Report of two cases and review of the literature. Surg Neurol. 2008. 70: 668-71
2. Elgamri A, Sami A, Aqqad A, Hilmani S, Ibahioin K, Naja A. Posterior migration of a lumbar disc herniation as a cause of cauda equina syndrome. J Radiol. 2009. 90: 731-3
3. Lombardi V. Lumbar spinal block by posterior rotation of anulus fibrosus.Case report. J Neurosurg. 1973. 39: 642-7
4. Mobbs RJ, Steel TR. Migration of lumbar disc herniation: An unusual case. J Clin Neurosci. 2007. 14: 581-4
5. Takano M, Hikita T, Nishumara S, Kamata M. Discography aids definitive diagnosis of posterior epidural migration of lumbar disc fragments: Case report and literature review. BMC Musculoskelet Disord. 2017. 18: 151-
6. Turan Y, Yilmaz T, Gocmez C, Ozevren H, Kemaloglu S, Teke M. Posterior epidural migration of a sequestered lumbar intervertebral disc fragment. Turk Neurosurg. 2017. 27: 85-94

