

- Department of Neurosurgery, All India Institute of Medical Sciences, Rishikesh, Uttarakhand, India.
- Department of Pathology, All India Institute of Medical Sciences, Rishikesh, Uttarakhand, India.
- Department of Medical oncology-Hematology, All India Institute of Medical Sciences, Rishikesh, Uttarakhand, India.
Correspondence Address:
Rajnish Kumar Arora
Department of Medical oncology-Hematology, All India Institute of Medical Sciences, Rishikesh, Uttarakhand, India.
DOI:10.25259/SNI_634_2020
Copyright: © 2020 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Garga Basu1, Michael L. Anthony2, Anamika Bakliwal3, Debranjani Chattopadhyay3, Prashant P. Joshi2, Rajnish Kumar Arora1, Radhey Shyam Mittal1, Uttam Kumar Nath3. Primary anaplastic lymphoma kinase-negative anaplastic large cell lymphoma of cervical spine presenting with quadriplegia: A case report and literature review. 06-Nov-2020;11:373
How to cite this URL: Garga Basu1, Michael L. Anthony2, Anamika Bakliwal3, Debranjani Chattopadhyay3, Prashant P. Joshi2, Rajnish Kumar Arora1, Radhey Shyam Mittal1, Uttam Kumar Nath3. Primary anaplastic lymphoma kinase-negative anaplastic large cell lymphoma of cervical spine presenting with quadriplegia: A case report and literature review. 06-Nov-2020;11:373. Available from: https://surgicalneurologyint.com/surgicalint-articles/10376/
Date of Submission
12-Sep-2020
Date of Acceptance
15-Oct-2020
Date of Web Publication
06-Nov-2020
Abstract
Background: An anaplastic large cell lymphoma (ALCL) involving the cervical spine and leading to quadriplegia is very rare.
Case Description: A 48-year-old immunocompetent male presented with quadriplegia that warranted an anterior cervical corpectomy/fusion. He was previously being presumptively treated for cervical disease attributed to tuberculosis. The histopathology and immunohistochemistry revealed an ALCL that was anaplastic lymphoma kinase (ALK) negative. The patient had a favorable response to surgery followed by CHOEP (cyclophosphamide, doxorubicin, vincristine, etoposide, and prednisolone) chemotherapy.
Conclusion: ALK-negative ALCL presenting with quadriplegia due to primary involvement of cervical spine is extremely rare, but must be diagnosed and appropriately managed.
Keywords: Anaplastic large cell lymphoma, Anaplastic lymphoma kinase negative, Cervical spine, Quadriplegia
INTRODUCTION
Primary lymphoma of the spine is very rare.[
CASE REPORT
A 48-year-old male patient presented with 1 year’s duration of progressive right-sided neck pain, a right C6 radiculopathy, and eventually a right > left spastic quadriparesis. The MRI revealed a destructive lesion involving the C3-C5 vertebra with an epidural collection. The original diagnosis was Potts disease (radiological diagnosis alone), and anti-tubercular drugs were utilized for 3 months. He finally developed a spastic quadriplegia with bladder involvement, leading to a contrast enhanced cervical MRI (CEMRI) and holospinal – CT. When these studies confirmed a destructive C3-5 lesion with an epidural collection, unchanged from prior study, the patient underwent an anterior C3, C4 (complete), and C5 (partial) corpectomy/fusion using an expandable cage [
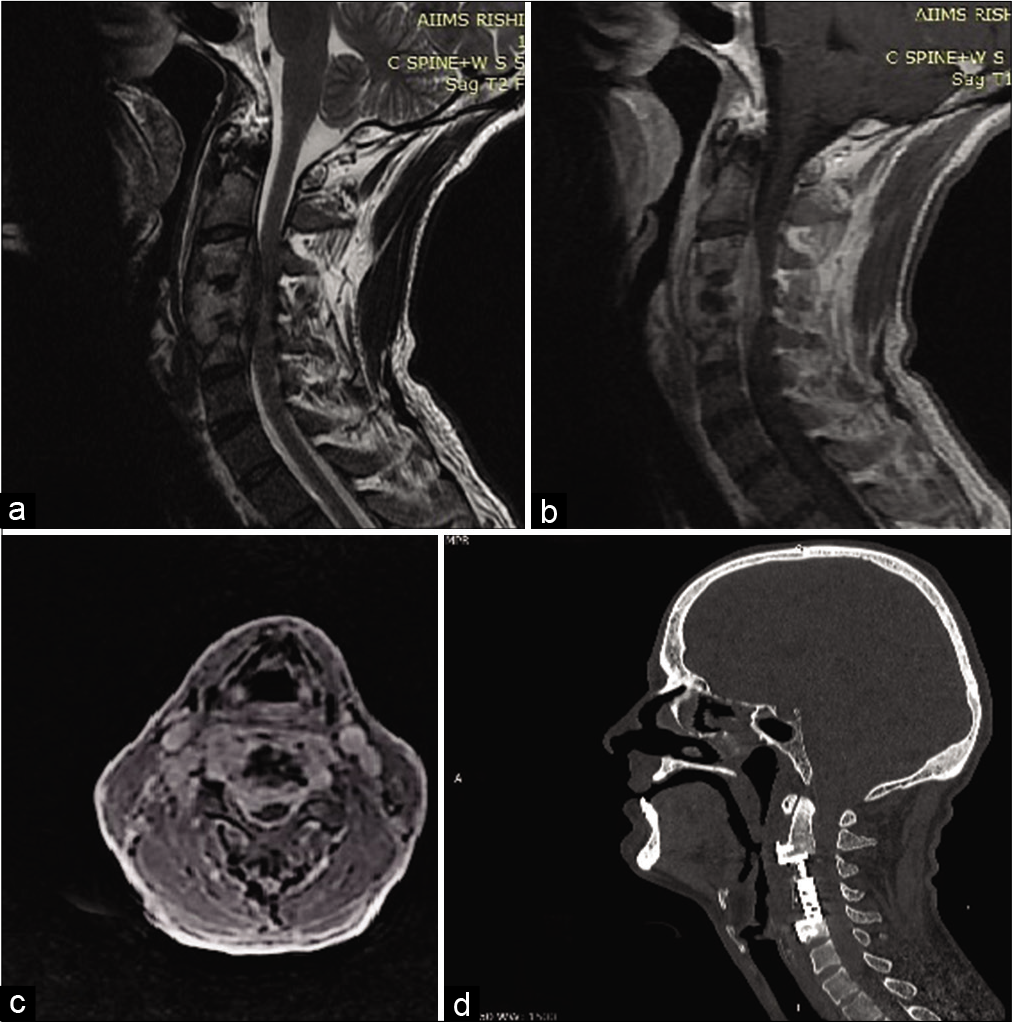
Figure 1:
(a) T2 sagittal MRI cervical spine showing complete destruction C4 with partial destruction of C3 and C5 body with anterior epidural collection with compression of cervical spinal cord between C3 and C5. (b) T1 gadolinium contrast-enhanced sagittal MRI cervical spine showing contrast-enhanced epidural lesion anterior to C3-C5. (c) Axial contrast-enhanced cervical MRI at C4 showing canal compromise. (d) Postoperative NCCT cervical spine shows adequate decompression between C3 and C5 with expandable titanium cage in situ.
Pathology
The histopathology showed diffuse sheets of large atypical oval to polygonal cells admixed with lymphocytes, eosinophils, neutrophils, plasma cells, and histiocytes. The tumor cells showed oval to horseshoe shaped nuclei, coarse chromatin, prominent nucleoli, and moderate amount of pale eosinophilic cytoplasm.
Immunohistochemistry
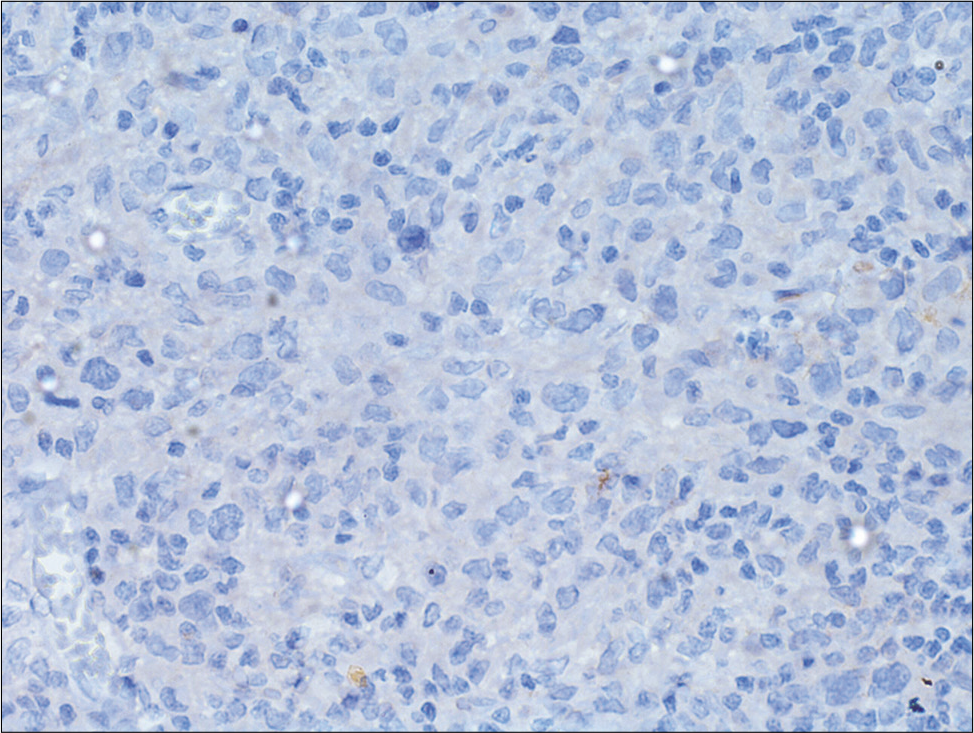
Immunohistochemistry showed tumor cells to be positive for CD3, CD4, CD7, CD8, CD30, and CD43 and negative for ALK-1, CD15, CD68, CD20, CD79a, CK, CD1A, and S-100; Ki-67 index of tumor cells was 20% [
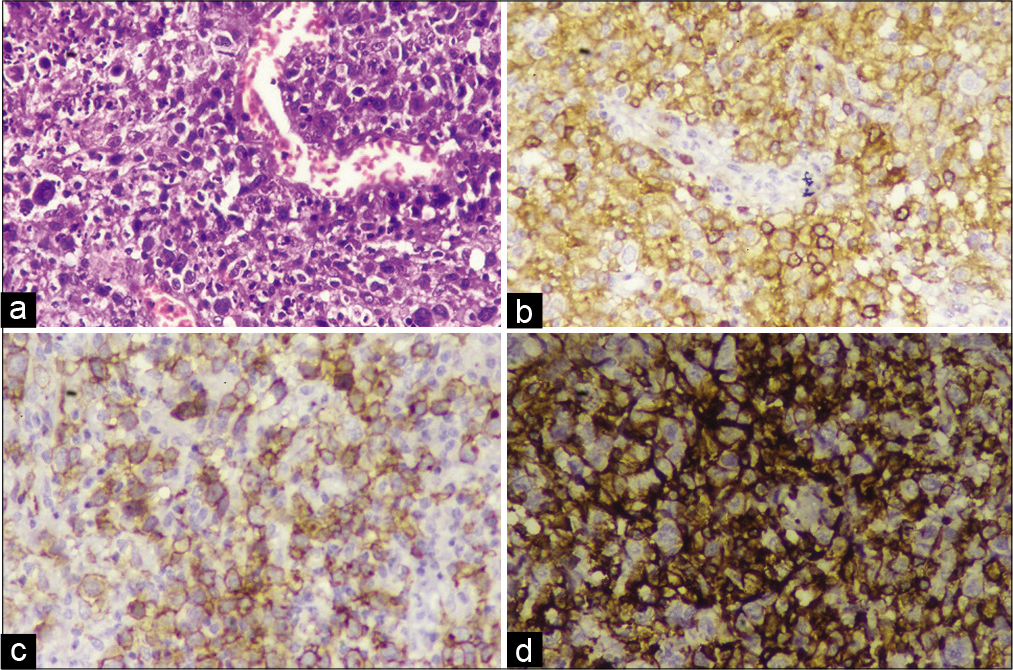
Figure 2:
Photomicrographs showing (a) large atypical cells scattered around and at places focally aggregated; the atypical cells have abundant cytoplasm, wreath-like nuclei, embryo-shaped nuclei with open chromatin and multiple nucleoli; background shows mixed lymphoid population and eosinophils (H&E, ×400). Immunohistochemistry showing (b and c) diffuse, strong positivity for CD4 and CD30, respectively, in the atypical cells, and (d) diffuse positivity of LCA in large atypical cells.
Staging of tumor
For staging, a CECT scan of the neck, thorax, abdomen, and pelvis, with bone marrow biopsy, CSF study with cytospin, and 99mTc-MDP bone scan were performed. The bone scan showed focal involvement at the operative site but there was no evidence of marrow involvement with lymphoma. The final diagnosis was primary ALK-negative ALCL of cervical spine.
Postoperative course
In the postoperative period, he was treated with CHOEP (cyclophosphamide, doxorubicin, vincristine, etoposide, and prednisolone) chemotherapy. He has received three cycles of CHOEP chemotherapy. A total of 6 cycles of CHOEP chemotherapy are planned. Postoperatively, he exhibited only mild residual spasticity.
DISCUSSION
Anaplastic large T-cell lymphoma (ALCL) is a CD30-expressing subtype of peripheral T-cell lymphomas; it accounts for less than 5% of all non-Hodgkin lymphomas.[

Chemotherapy
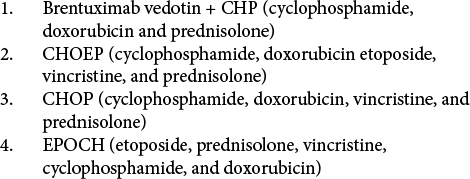
Six cycles of multiagent chemotherapy, with or without involved site radiation therapy, are preferred for the treatment of ALK-negative ALCL. The first-line chemotherapy regimen consists of brentuximab vedotin + CHP (cyclophosphamide, doxorubicin, and prednisolone) [
Vertebral involvement
Primary vertebral involvement by ALCL is very rare[
CONCLUSION
In a patient presenting with quadriplegia, an ALK-negative anaplastic large cell cervical spine lymphoma was diagnosed following an anterior corpectomy/fusion from C3-C5; this followed by appropriate chemotherapy resulted in significant neurological improvement.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Abrego G, García J, Gilbert B, Forseen S, Toscano M. ALK positive anaplastic large cell lymphoma of the thoracic spine. J Radiol Case Rep. 2016. 10: 1-12
2. Bakshi NA, Ross CW, Finn WG, Valdez R, Ruiz R, Koujok K. ALK-positive anaplastic large cell lymphoma with primary bone involvement in children. Am J Clin Pathol. 2006. 125: 57-63
3. Chan JKC, Ng CS, Hui PK, Leung WT, Sin VC, Lam TK. Anaplastic large cell Ki-1 lymphoma of bone. Cancer. 1991. 68: 2186-91
4. Kumar S, Wanchu A, Sharma A, Mukherjee K, Radotra BD, Gupta V. Spinal cord compression caused by anaplastic large cell lymphoma in an HIV infected individual. J Cancer Res Ther. 2010. 6: 376-8
5. Novello M, Lauriola L, Pepa GM, Giuseppe LR, Coli A, Visocchi M. ALK-positive anaplastic large cell lymphoma presenting as intradural spinal mass: First reported case and review of literature. Neuropathology. 2013. 33: 418-23
6. Smith ZA, Sedrak MF, Khoo LT. Primary bony non-Hodgkin lymphoma of the cervical spine: A case report. J Med Case Rep. 2010. 4: 35
7. Splavski B, Muzevic D, Ladenhauser-Palijan T, Splavski B Jr. Primary central nervous system anaplastic large T-cell lymphoma. Med Arch. 2016. 70: 311-3

