

- Department of Neurosurgery, Junshin Hospital, Kakogawa, Japan.
- Department of Neurosurgery, Kobe University Graduate School of Medicine, Kobe, Japan.
Correspondence Address:
Satoshi Inoue, Department of Neurosurgery, Junshin Hospital, Kakogawa, Japan.
DOI:10.25259/SNI_998_2022
Copyright: © 2023 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Satoshi Inoue1, Atsushi Fujita2, Eiji Kurihara1, Takashi Sasayama2. PulseRider “jack-up” technique for wide-necked basilar tip aneurysms that incorporate parent arteries: A technical note. 13-Jan-2023;14:9
How to cite this URL: Satoshi Inoue1, Atsushi Fujita2, Eiji Kurihara1, Takashi Sasayama2. PulseRider “jack-up” technique for wide-necked basilar tip aneurysms that incorporate parent arteries: A technical note. 13-Jan-2023;14:9. Available from: https://surgicalneurologyint.com/surgicalint-articles/12105/
Date of Submission
31-Oct-2022
Date of Acceptance
23-Dec-2022
Date of Web Publication
13-Jan-2023
Abstract
Background: Treatment of intracranial wide-necked bifurcation aneurysms remains challenging. We report a novel PulseRider “jack-up” technique for the treatment of wide-necked basilar tip aneurysms.
Case Description: We performed coil embolization in three patients with an unruptured wide-necked basilar tip aneurysm. Aneurysm neck diameters ranged between 7.6 and 11 mm and dome-to-neck ratios ranged from 1.0 to 1.15. All three aneurysms were very shallow with aspect ratios of 0.51–0.69 and incorporated both posterior cerebral arteries into the aneurysm wall. Because each was difficult to embolize using the standard PulseRider procedure, the PulseRider was deployed more proximally than usual and a coil frame constructed above it. Then, the coil was pushed or “jacked up” into the aneurysm with the PulseRider. Adequate embolization was achieved in all three patients.
Conclusion: Coil embolization using the PulseRider jack-up technique is effective for treatment of wide-necked basilar tip aneurysms that incorporate parent arteries.
Keywords: Aspect ratio, Balloon assist technique, Stent assist coil embolization, Y-stenting
INTRODUCTION
Treatment of wide-necked bifurcation cerebral aneurysms in which the parent artery is incorporated into the aneurysm remains challenging. Treatment options include double catheter coil embolization, balloon-assisted coiling, and several stent-assisted coiling techniques, including Y- and T-stenting.[
PulseRider leaflets can be deployed in three positions: (1) an intra-aneurysmal position with both leaflets within the aneurysm, (2) an extra-aneurysmal position with both leaflets outside the aneurysm but within the parent artery, and (3) a hybrid position with one leaflet within the aneurysm and the other within the parent artery.[
We recently treated three patients with a wide-necked shallow basilar tip aneurysm that was not amenable to treatment using the standard PulseRider procedure. In all three, the parent artery itself was dilated and both posterior cerebral arteries (PCAs) or superior cerebellar arteries (SCAs) were incorporated into the aneurysm wall. The dome-to-neck and aspect ratios were also low in each aneurysm. Placing the PulseRider in the aneurysm neck in the standard fashion left a large space uncovered, which allowed deviation and migration of coil loops into the parent artery, even with small coils and after adjusting the PulseRider position. With the “jack-up” technique, the PulseRider is deployed more proximally than usual, a coil frame is constructed above it, and the coil is jacked up into the aneurysm later using the PulseRider. Using this technique achieved successful embolization in all three patients. To the best of our knowledge, neither this technique nor similar ones have been previously reported. Here, we report our experience and describe several technical tips.
METHODS
Three patients with an unruptured wide-necked basilar tip aneurysm underwent endovascular treatment. Aneurysm measurements were performed using three-dimensional rotational angiography. Dome-to-neck and aspect ratios were calculated. Dual antiplatelet therapy (aspirin 100 mg/day and clopidogrel 75 mg/day) was initiated at least 1 week before the treatment. Platelet function was evaluated using the VerifyNow aspirin reaction unit (ARU) and P2Y12 reaction unit (PRU) assays (Werfen, Bedford, MA, USA). Treatment was performed under general anesthesia. Patients were heparinized to achieve an activated clotting time (ACT) of 200–300 s. A 90 cm 5-Fr guiding catheter (Fubuki Dilator Kit; Asahi Intecc Medical, Aichi, Japan) was placed through the femoral artery to the vertebral artery in parallel with Prowler Select Plus (Cerenovus) and Excelsior SL10 (Stryker Neurovascular, Fremont, CA, USA) microcatheters. A 120 cm Guidepost (Tokai Medical Products, Inc., Aichi, Japan) was used as an intermediate catheter for the Prowler Select Plus as needed.
We first attempted coil embolization using the standard PulseRider procedure. The PulseRider was deployed through the Prowler Select Plus at the standard location in the aneurysm neck [
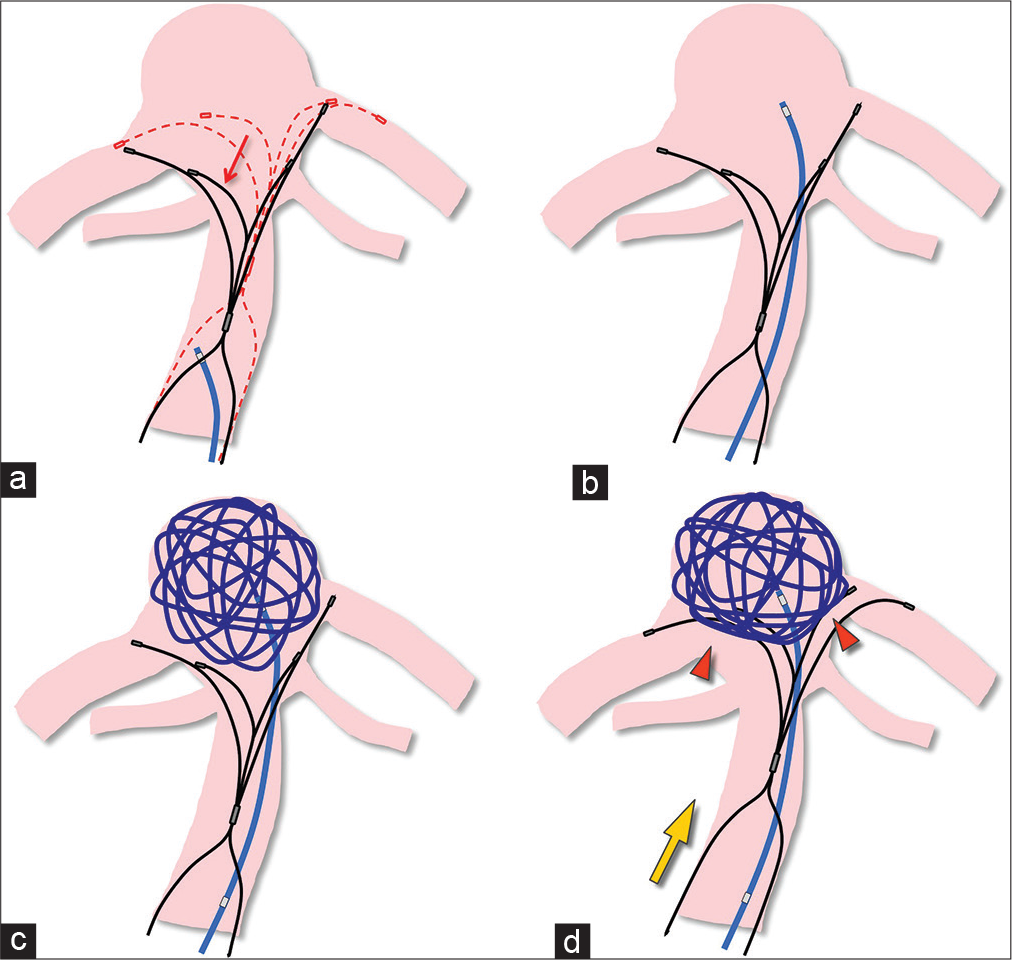
Figure 1:
With the PulseRider jack-up technique, (a) the PulseRider is temporarily positioned lower than usual (red arrow). The dotted lines indicate the typical position. (b) A microcatheter is then guided into the aneurysm for placement of coils. (c) A three-dimensional frame is created using the coil itself. (d) The PulseRider is advanced (yellow arrow) to pack the coil mass (arrowheads) into the aneurysm and then detached after coil embolization is completed.
The SL10 and PulseRider were temporarily withdrawn proximally into the parent artery [
CASE DESCRIPTION
Case 1
A 76-year-old woman with an incidental unruptured basilar tip aneurysm that enlarged during follow-up underwent endovascular treatment. Aspirin and clopidogrel were started 1 week before. The ARU and PRU were 392 and 135, respectively, at 2 days before the treatment.
On angiography, both PCAs were incorporated into the aneurysm wall and bifurcated laterally [
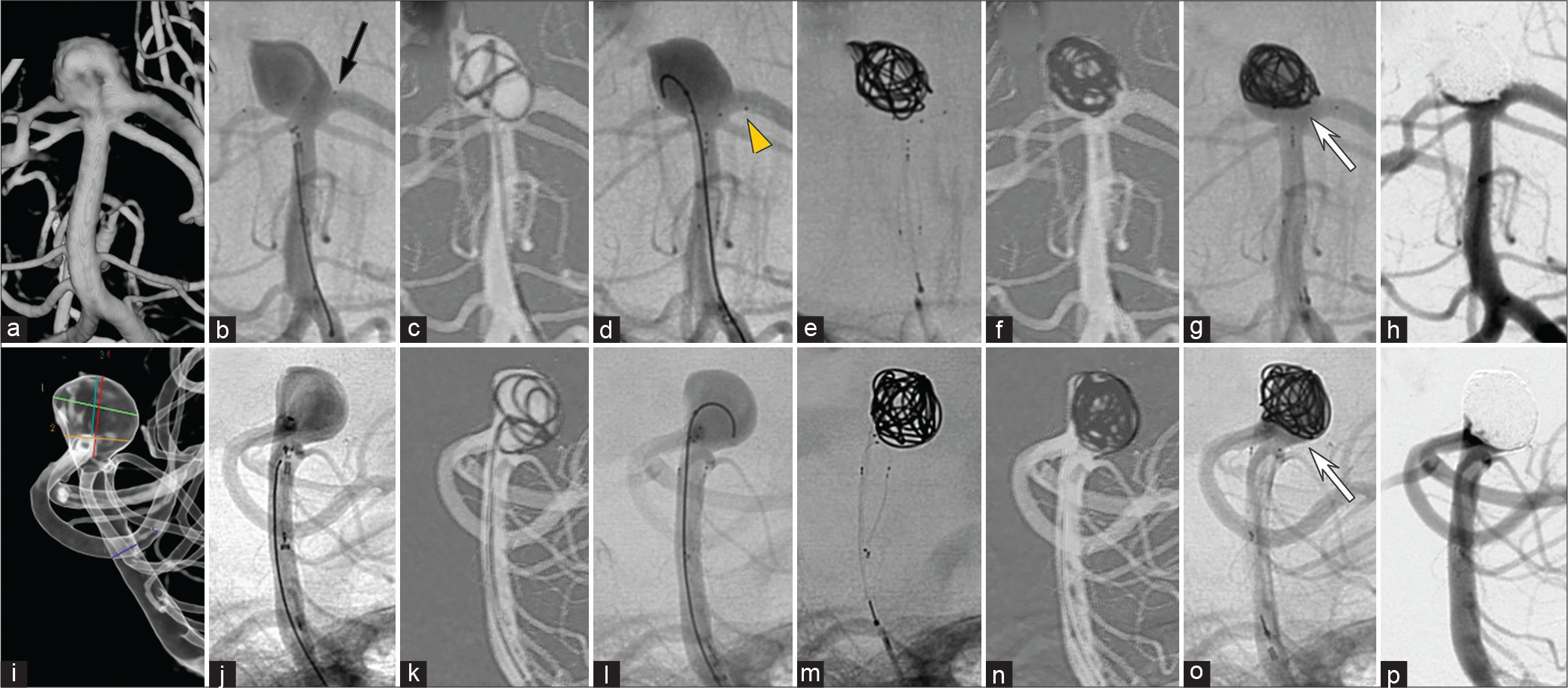
Figure 2:
(a-p) Angiography images of the basilar tip aneurysm in case 1. Panels are described in detail in the text. The black arrow indicates the PulseRider deployed in the normal position. The yellow arrowhead indicates the device position after partial proximal withdrawal. The white arrows indicate the coil mass “jacked up” into the aneurysm.
After the procedure, the patient complained of mild diplopia. Diffusion-weighted magnetic resonance imaging on the next day showed a high-signal area in the left paramedian medulla oblongata. Magnetic resonance angiography (MRA) was normal. The patient was discharged home on day 13.
Case 2
A 60-year-old woman presented with a ruptured left internal carotid artery aneurysm that was surgically clipped. Seventy-four days later, an unruptured basilar tip aneurysm was treated endovascularly. On angiography, both PCAs and SCAs branched off the wall in the middle of the dome [
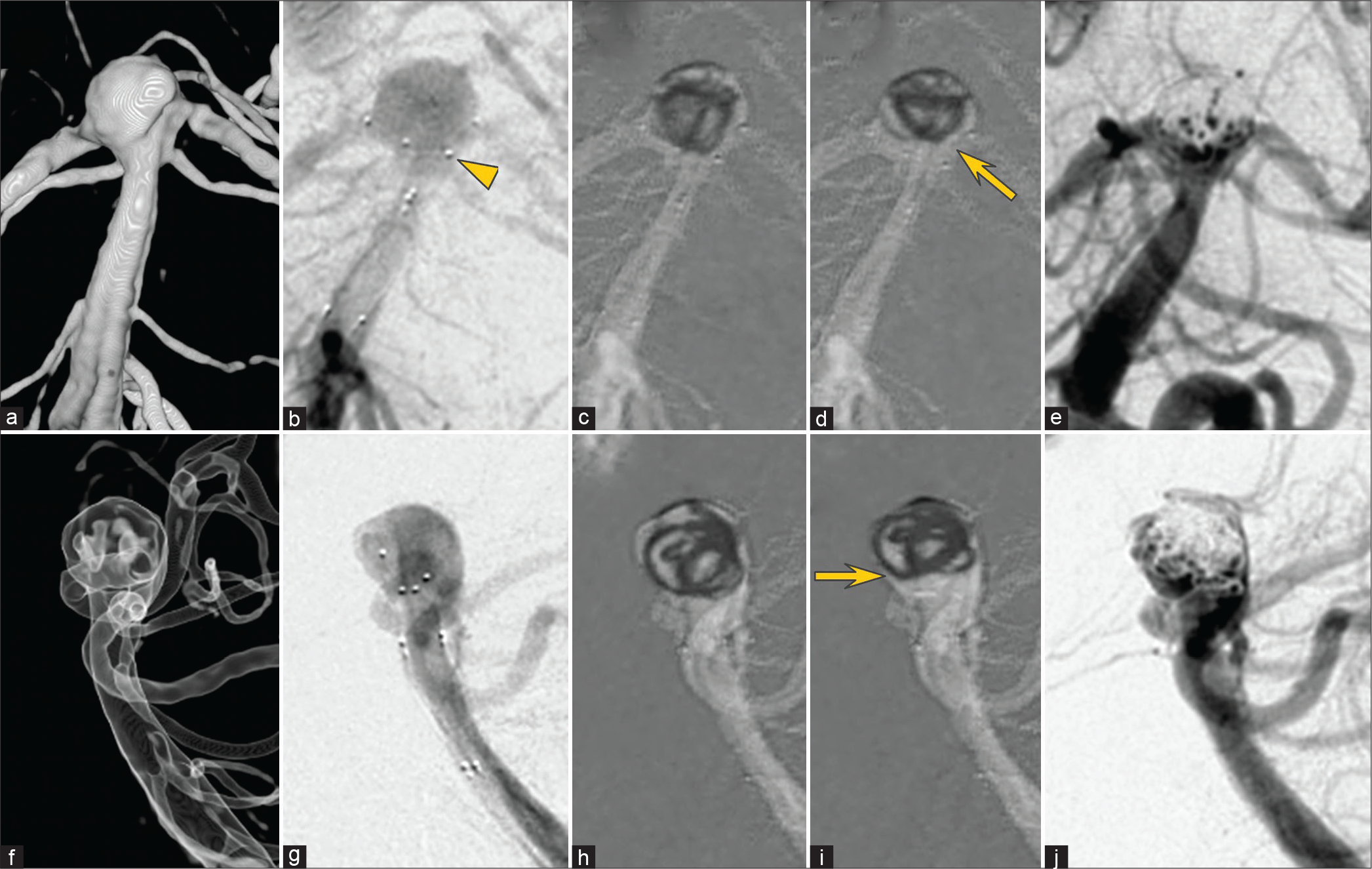
A PulseRider (10T/3.5–4.5) was deployed in the extra-aneurysmal position with the leaflets inside each PCA [
Case 3
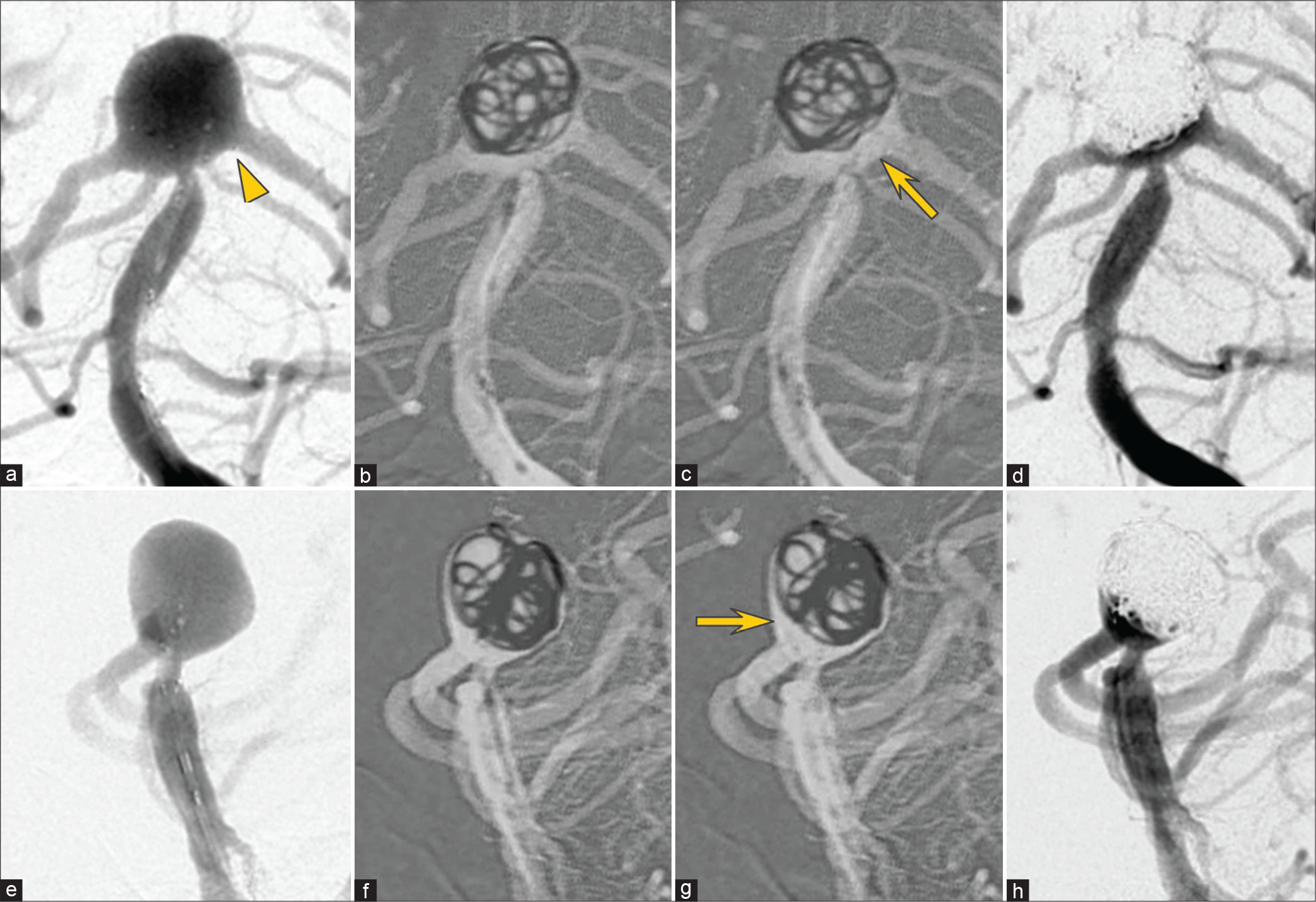
A 74-year-old woman with a brainstem infarction showed an unruptured basilar tip aneurysm on MRA. Angiography showed incorporation of both PCAs and SCAs into the aneurysm wall; both PCAs branched laterally. Aneurysm measurements were as follows: diameter, 11 mm; neck, 11 mm; and height, 7 mm. Dome-to-neck and aspect ratios were 1.0 and 0.64, respectively. A PulseRider (10T/3.5–4.5) was deployed in the hybrid position, with the left leaflet in the left PCA and the right leaflet in the aneurysm. An Axium Prime Frame (8 mm × 30 cm) was inserted but easily deviated. Therefore, the PulseRider was temporarily withdrawn proximally [
DISCUSSION
Wide-necked aneurysms are generally defined as those with a neck diameter of 4 mm or greater or a dome-to-neck ratio <2.0. These criteria are also considered indications for use of PulseRider in Japan. Brinjikji et al.[
Advantages of the PulseRider jack-up technique
The jack-up technique has several advantages. First, it is simpler and easier than balloon-assisted or stent-assisted techniques since it does not require a wire or catheter to select branches. Second, before creating and jacking up the coil frame, the coil and PulseRider are not detached, allowing repeated and partial reinsertion of the coil, if necessary. Third, the coiling catheter is guided into the aneurysm with the PulseRider in a lower position than usual, which provides more distance between the catheter tip and the aneurysm and may reduce the risk of aneurysm rupture caused by jumping of the catheter. Fourth, if only a single coil is jacked up, the PulseRider’s handling is minimally compromised. Fifth, since the coiling catheter is not strongly fixed, it retains maneuverability. Sixth, the coils inside the aneurysm are minimally changed by the jack-up maneuver, whereas coils that deviate into the parent artery may be compressed and increase in density (especially in case 1). This may be advantageous for subsequent embolization. Finally, the low metal content makes PulseRider less thrombogenic, and therefore, although an off-label use, less antithrombotic medication may be required when used in ruptured aneurysms.[
Challenges with the PulseRider jack-up technique
Potential complications of the jack-up technique include aneurysm perforation and parent artery dissection due to aneurysm or vessel injury caused by the PulseRider leaflets.
These can occur with standard PulseRider implantation as well as the jack-up technique. With the latter, leaflet visibility may be reduced because a coil is present. Therefore, we first place the PulseRider in its standard neck position to ensure good alignment with the neck and parent artery and then pull it back before advancing it again after the coil frame has been constructed. However, multiple device advancements may increase the potential for complications.
CONCLUSION
The PulseRider jack-up technique is a simple and useful technique for coil embolization of wide-necked basilar tip aneurysms that incorporate the PCAs and SCAs. This method can serve as a rescue technique for cases in which standard PulseRider placement results in coil protrusion into the parent artery.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
References
1. Aydin K, Stracke CP, Barburoglu M, Yamac E, Berdikhojayev M, Sencer S. Long-term outcomes of wide-necked intracranial bifurcation aneurysms treated with T-stent-assisted coiling. Neurosurg. 2019. 6: 1-10
2. Brinjikji W, Cloft HJ, Kallmes DF. Difficult aneurysms for endovascular treatment: Overwide or undertall?. AJNR Am J Neuroradiol 200;. 30: 1513-7
3. Folzenlogen Z, Seinfeld J, Kubes S, Kumpe D, Case D, Roark C. Use of the pulserider device in the treatment of ruptured intracranial aneurysms: A case series. World Neurosurg. 2019. 127: e149-54
4. Granja MF, Cortez GM, Aguilar-Salinas P, Agnoletto GJ, Imbarrato G, Jaume A. Stent-assisted coiling of cerebral aneurysms using the Y-stenting technique: A systematic review and meta-analysis. J Neurointerv Surg. 2019. 11: 683-9
5. Pranata R, Yonas E, Vania R, Sidipratomo P, July J. Efficacy and safety of pulserider for treatment of wide-necked intracranial aneurysm-A systematic review and meta-analysis. Interv Neuroradiol. 2021. 27: 60-67
6. Spiotta AM, Sattur MG, Kan P, Crowley RW. Bifurcation aneurysm treatment with pulserider: Technical nuances, device selection, positioning strategies, and overcoming geometric challenges. World Neurosurg. 2020. 142: 339-51
7. Weinberg JH, Sweid A, Asada A, Abbas R, Joffe D, El Naamani K. coil embolization of wide-neck bifurcation aneurysms via shouldering and framing: A safe alternative to conventional techniques. World Neurosurg. 2020. 139: e800-6

