

- Department of Neurosurgery, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India.
Correspondence Address:
Vikrant Yadav, Department of Neurosurgery, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India.
DOI:10.25259/SNI_515_2023
Copyright: © 2023 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Vikrant Yadav, Nityanand Pandey. Quartet of catastrophe: Bilateral epidural hematoma in both supratentorial and infratentorial compartments – A case report and a novel surgical technique to approach. 13-Oct-2023;14:369
How to cite this URL: Vikrant Yadav, Nityanand Pandey. Quartet of catastrophe: Bilateral epidural hematoma in both supratentorial and infratentorial compartments – A case report and a novel surgical technique to approach. 13-Oct-2023;14:369. Available from: https://surgicalneurologyint.com/surgicalint-articles/12588/
Date of Submission
17-Jun-2023
Date of Acceptance
29-Sep-2023
Date of Web Publication
13-Oct-2023
Abstract
Background: Epidural hematoma (EDH) is the most common form of traumatic brain lesion in the posterior fossa. This condition is rapidly fatal if not identified and treated accordingly, due to the proximity of the brain stem. Prompt diagnosis is made by early computed tomography (CT) of the head and emergent evacuation is of utmost importance.
Case Description: A 28-year-old male presented to the emergency room with complaints of headache and vomiting following a road traffic accident. CT scan revealed EDH around the transverse sinus extending into supratentorial and infratentorial compartment bilaterally. The patient was planned for emergency surgery but relatives did not give consent initially they agreed after 24 h when the patient became unconscious. A midline incision was made and a small infratentorial craniectomy with two burr holes was made bilaterally above the transverse sinus. Excellent recovery was seen following a surgical procedure.
Conclusion: Posterior fossa EDH is a rare but potentially fatal entity. Bilateral extension in supratentorial and infratentorial compartments makes it a “quartet of catastrophe.” Prompt diagnosis and emergent evacuation lead to excellent recovery. Two burr holes in supratentorial compartments and a small infratentorial craniectomy can avoid sinus injury.
Keywords: Epidural hematoma, Infratentorial, Posterior fossa, Supratentorial
INTRODUCTION
Posterior fossa infratentorial epidural hematoma (EDH) are extremely rare lesions (0.1–0.3%) in traumatic brain injuries.[
Hereby authors describe a case of bilateral supratentorial and infratentorial EDH for which a novel technique was used to evacuate EDH which avoided sinus injury and minimal blood loss resulting in better convalescence.
CASE ILLUSTRATION
A 28-year-old male presented to the emergency room with complaints of severe headache and vomiting following a road traffic accident where he had an impact on the back of his head with a blunt object. The patient was fully conscious at the time of admission. He was resuscitated with fluids and antiemetics. His vitals were stable. Initial CT head scans after 6 h from injury showed a fracture in the occipital bone [
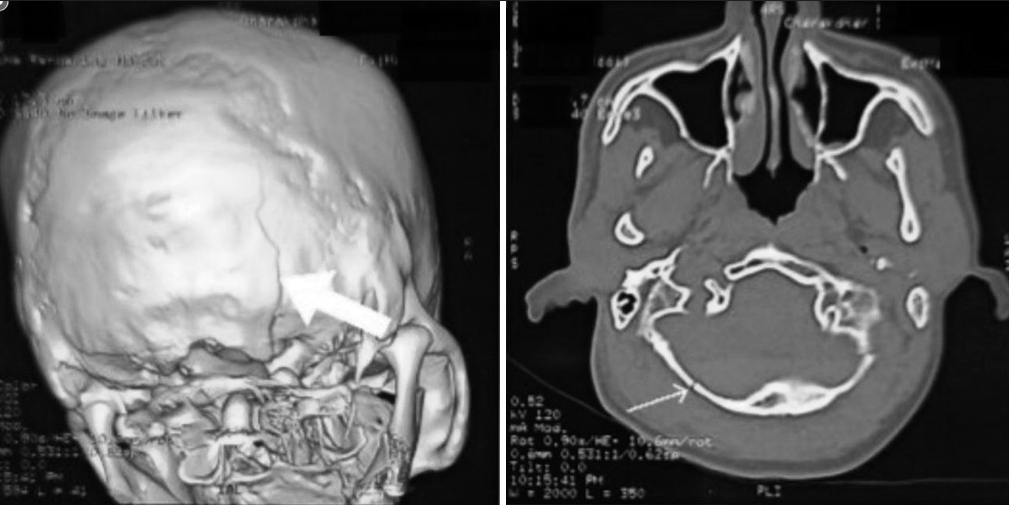
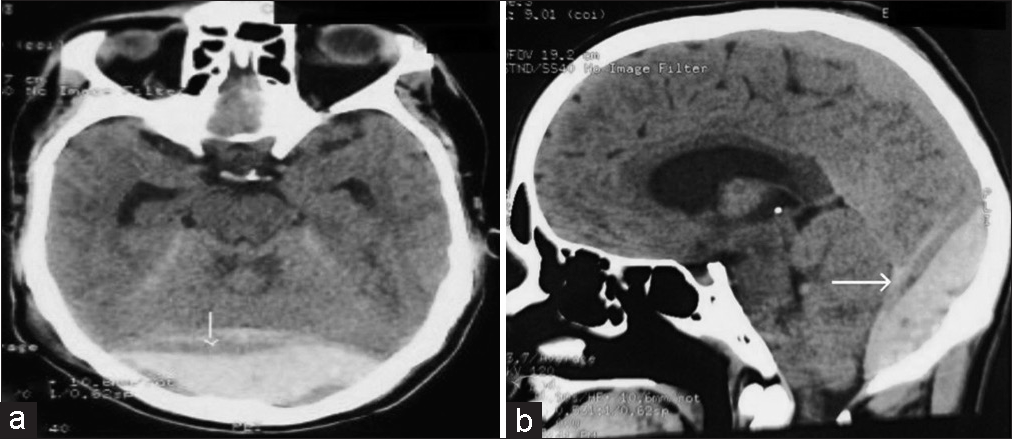
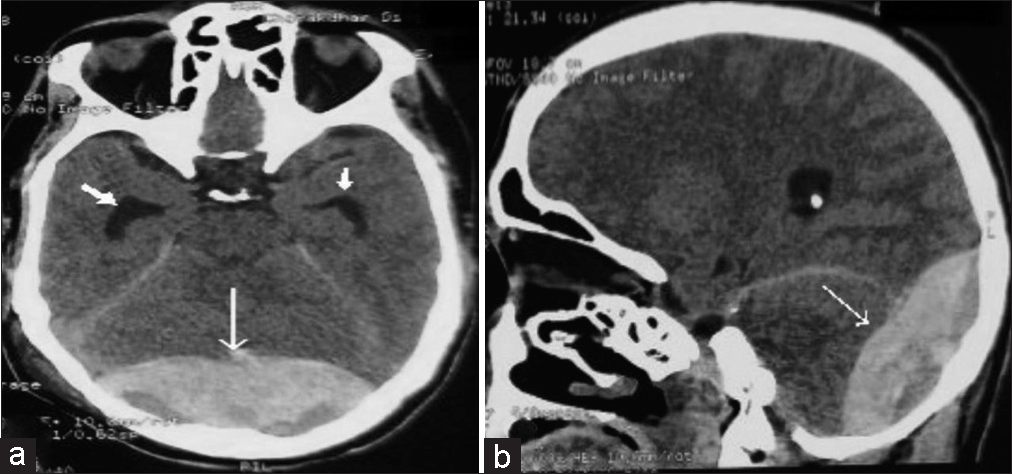
Figure 3:
(a) Preoperative axial computed tomography (CT) scan head after 24 h of admission showing an increase in the size of hematoma (thin arrow) with an increase in the size of temporal horns (thick arrow) (b) preoperative sagittal CT scan head after 24 h of admission showing an increase in the size of hematoma (thin arrow).
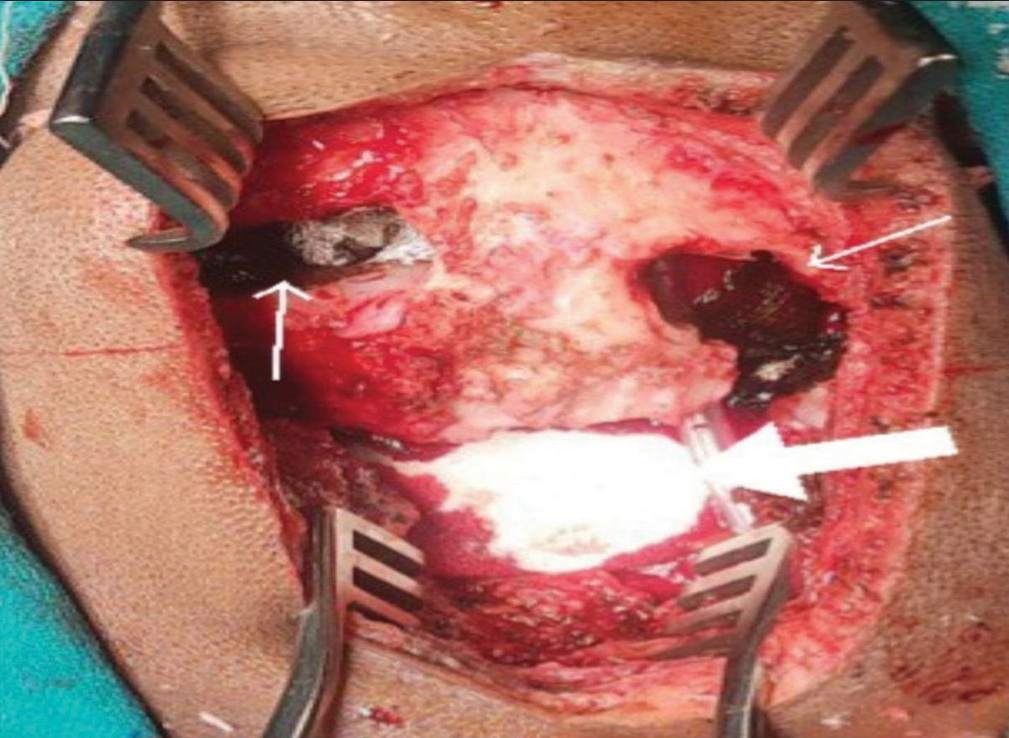
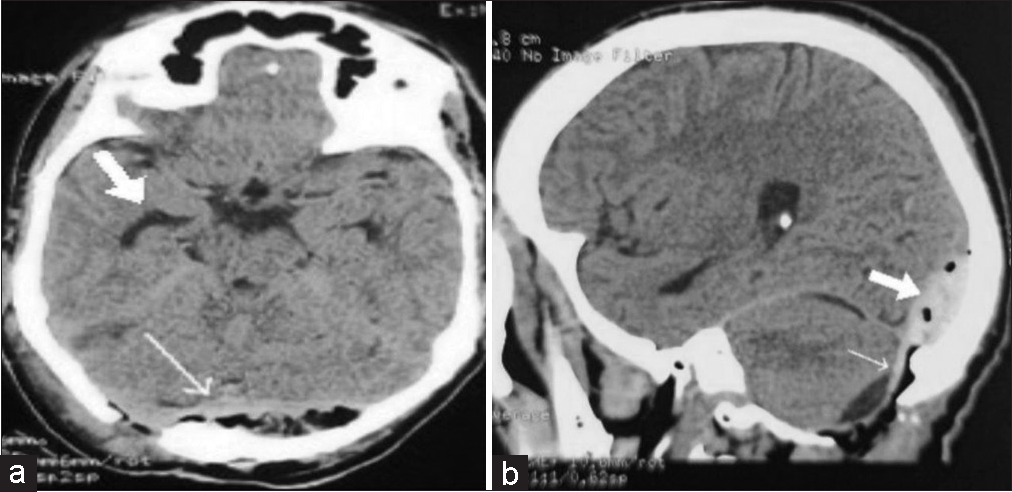
Figure 5:
(a) Postoperative axial computed tomography (CT) scan head on day 1 showing evacuated Epidural hematoma (EDH) (thin arrow) and decrease in size of ventricles (thick arrow) (b) postoperative sagittal CT scan head showing evacuated infratentorial EDH (thin arrow) and a small amount of residual blood (thick arrow).
DISCUSSION
Posterior fossa infratentorial EDH is a rare entity in (0.1– 0.3%) the continuum of traumatic brain injuries.[
Emergent surgical evacuation is the treatment of choice in these types of patients. Suboccipital craniectomy/ craniotomy with evacuation of EDH has excellent results for infratentorial EDH. For supratentorial extensions of EDH craniotomy or burr holes can be made. Bony strips over sinuses are not touched as inadvertent injury to sinuses leads to air embolism, hypotension due to massive bleeding, or hypoxic brain injury.[
In our case, bilateral extension of EDH in both supratentorial and infratentorial compartments was managed by a novel technique by making two burr holes in supratentorial compartments and small infratentorial craniectomy to minimize venous sinuses injury. A small amount of residual blood trickles down slowly through the burr hole after a few days which is easily absorbed by subgaleal tissue.
Mortality in posterior fossa EDH is 0–50% in various studies due to late presentation, intraoperative bleeding, etc.[
CONCLUSION
Posterior fossa EDH is a rare but fatal entity. Extension of hematoma above supratentorial regions bilaterally makes a “quartet of catastrophe.” Prompt diagnosis along with safe and emergent evacuation of hematoma leads to excellent recovery. Two burr holes in supratentorial compartments and a small infratentorial craniectomy can avoid sinus injury.
Declaration of patient consent
Patient’s consent not required as patient’s identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)- assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
Acknowledgment
I am grateful to Dr Rajat Jangir for his invaluable effort in drafting the manuscript.
References
1. Aggarwal A, Salunke P, Futane S, Sodhi HB. Bilateral posterior fossa and temporo-occipital extra-dural hematomas: A simple novel technique. Asian J Neurosurg. 2017. 12: 253-5
2. Al-Nakshabandi NA. The swirl sign. Radiology. 2001. 218: 433
3. Al-Zekri M, Assoumane I, Bachir S, Handis C, Khelifa A, Morsli A. Supra-and infra-tentorial subacute extradural hematoma. Chin J Traumatol. 2020. 23: 122-4
4. Pandey S, Sharma V, Shinde N, Sharma M. Bilateral occipital extradural hematoma in a child. J Pediatr Neurosci. 2015. 10: 270-2
5. Sadie AR, Epstein FJ, Ransohoff J. Epidural hematoma of posterior fossa. N Y State J Med. 1978. 78: 801-3
6. Verma SK, Borkar SA, Singh PK, Tandon V, Gurjar HK, Sinha S. Traumatic posterior Fossa extradural hematoma: Experience at Level I trauma center. Asian J Neurosurg. 2018. 13: 227-32

