

- Department of Neurosurgery, Moriyama Memorial Hospital, Tokyo, Japan
Correspondence Address:
Atsushi Ishida
Department of Neurosurgery, Moriyama Memorial Hospital, Tokyo, Japan
DOI:10.4103/2152-7806.162552
Copyright: © 2015 Ishida A. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.How to cite this article: Ishida A, Matsuo S, Asakuno K, Nemoto A, Niimura K, Yoshimoto H, Shiramizu H, Yuzawa M. Rebleeding from clipped aneurysm after 35 years: Report of 2 cases. Surg Neurol Int 10-Aug-2015;6:134
How to cite this URL: Ishida A, Matsuo S, Asakuno K, Nemoto A, Niimura K, Yoshimoto H, Shiramizu H, Yuzawa M. Rebleeding from clipped aneurysm after 35 years: Report of 2 cases. Surg Neurol Int 10-Aug-2015;6:134. Available from: http://surgicalneurologyint.com/surgicalint_articles/rebleeding-from-clipped-aneurysm-after-35-years-report-of-2-cases/
Abstract
Background:A successfully applied clip for a ruptured aneurysm keeps the aneurysm's neck closed, preventing rerupture throughout the patient's life. Unfortunately, rebleeding from a clipped aneurysm does occur, but the likelihood declines with time. Since relatively old people suffer from subarachnoid hemorrhage, they die from diseases other than rebleeding, such as cancer. Therefore, rebleeding from a clipped aneurysm after two decades is quite rare.
Case Description:Here, we report 2 cases of rerupture after an extremely long time since the initial clipping. In both cases, the old clip was removed, and the regrown gourd-shaped aneurysm was successfully obliterated. The clips in both cases were submitted to their manufacturers and inspected thoroughly. They were found to be second-generation, stainless steel clips, and were almost intact, even keeping their closing forces. In both cases, the clip existed on the surface of the newly made dome, and the previous dome completely disappeared.
Conclusions:We experienced 2 cases of rebleeding from the clipped aneurysm after 35 years. In one of the cases, the clip was a Yasargil second generation stainless steel clip that retained its mechanical properties and surface elemental composition in vivo for a long time. These cases should be informative as they show extremely long-term course of a clip applied for a ruptured aneurysm.
Keywords: Long-term follow-up, rebleeding, subarachnoid hemorrhage
INTRODUCTION
Complete neck clipping for ruptured aneurysms has been the most important procedure in modern neurosurgical history. Until recent dramatic improvement of endovascular obliteration, clipping was the dominant treatment for subarachnoid hemorrhage (SAH), being performed in a large number of cases. SAH caused by aneurysmal rupture had its peak in their 50's and 60's, and survivors usually died because of cancer or cardiovascular disease. For all that, intracranial aneurysms develop during life and survivors of SAH are at risk for a recurrence.[
Here, we describe in detail the cases of rerupture from the treated aneurysm after 35 years. We also describe the regrown aneurysm and the retrieved clips, which were studied thoroughly by their manufacturers.
CASE REPORTS
Case 1
History and examination
A 75-year-old man had SAH due to left middle cerebral artery aneurysmal rupture and clipping surgery 35 years ago. It appeared that he was doing well afterward; however, he collapsed, and he was then transferred to a nearby hospital. It was determined that he had suffered a second SAH due to a rupture of the original aneurysm [
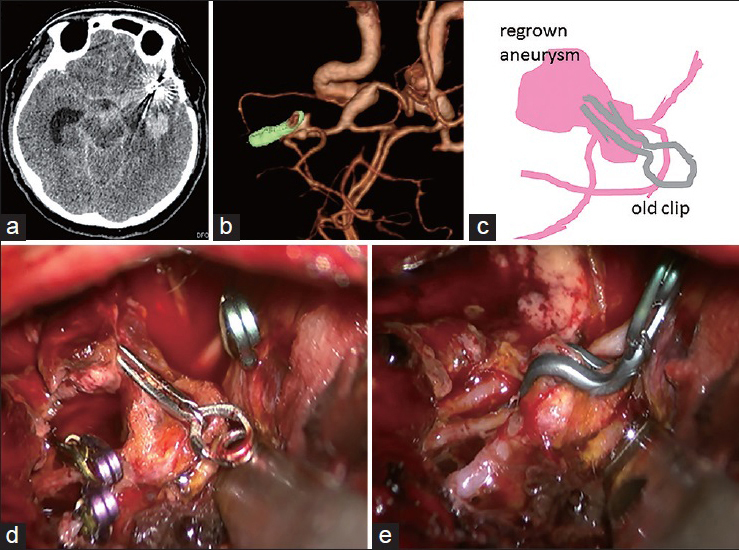
Figure 1
Case 1. (a) Head computed tomography scan. (b) Three-dimensional computed tomography angiography showing a gourd-shaped regrown aneurysm under the clip (implanted for 35 years) at left middle cerebral artery bifurcation. (c) Schematic image of the regrown aneurysm. (d) Intraoperative photograph showing the old clip with cotton clothes on the regrown aneurysm. (e) A crank-shaped clip was applied along the closure line
Operation
Fronto-temporal craniotomy was performed as in the previous operation. After careful removal of sylvian fissure hematoma, the old clip was identified [
Postoperative course
The postoperative recovery was uneventful, but intracerebral hematoma caused irreversible brain damage. Even after ventriculoperitonial shunt, the patient has been bedridden since the SAH occurred.
Characteristics of the retrieved clip
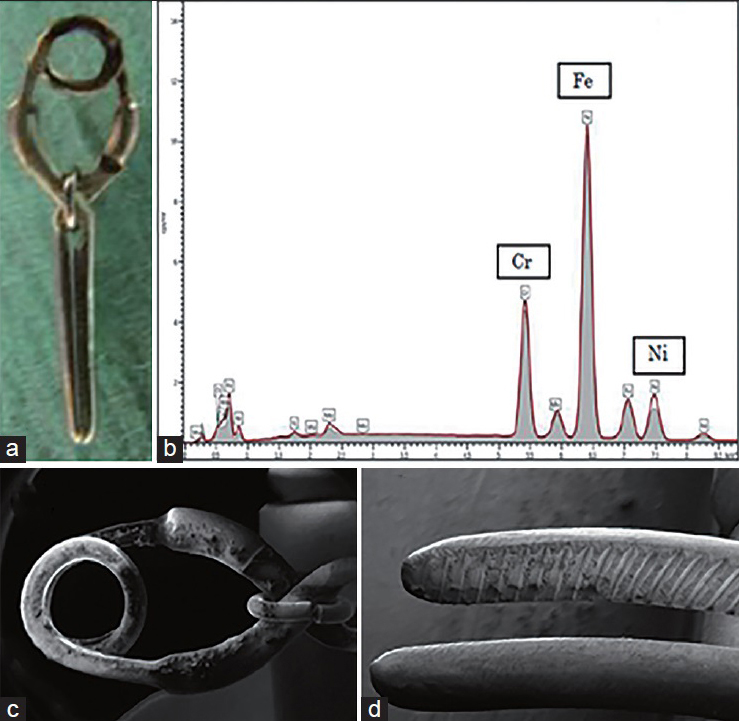
The clip was found to be a Yasargil Phynox aneurysm clip (Aesculap AG, Tuttlingen, Germany). It was a second-generation product (code number, FD742), and there was no severe damage or any corrosion [
Case 2
History and examination
A 72-year-old woman had SAH, and a ruptured anterior communicating artery aneurysm clipped 35 years ago and appeared to have fully recovered afterward. The patient presented with a severe headache. CT scanning showed SAH in the interhemispheric fissure, indicating rerupture of the previous aneurysm [
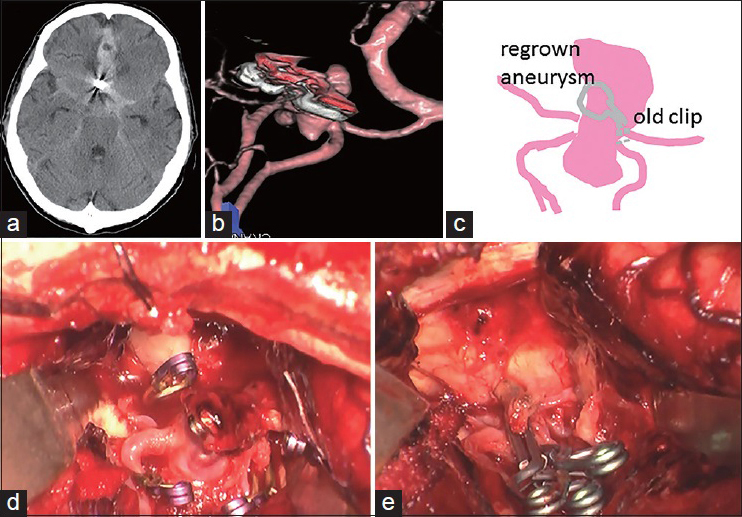
Figure 3
Case 2. (a) Head computed tomography scan. (b) Three-dimensional angiography showing a guard-shaped regrown aneurysm under the clip (implanted for 35 years) at anterior communicating artery. (c) Schematic image of the regrown aneurysm. (d) Intraoperative photograph showing the old clip on the regrown aneurysm. (e) Three straight clips were applied to obliterate the aneurysm completely
Operation
Skin incision and craniotomy were performed, as they had been 35 years prior. By removing and washing the hematoma, the interhemispheric fissure was easily opened, and the clip head appeared. Clearing the hematoma away from the clip, the aneurysm appeared in full view [
Postoperative course
The patient awoke from the surgery without neurological defects but with minor disturbance of cognitive function, and then returned to normal daily life. The postoperative and follow-up CTA showed no evidence of a residual aneurysm.
Characteristics of the retrieved clip
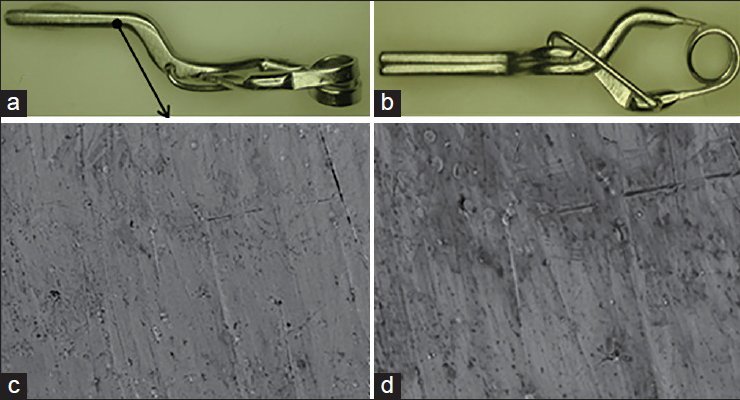
The clip was determined to be a product of Mizuho Ikakogyo Co., Ltd., (Tokyo, Japan). It was identified as a Sugita clip (Sugita No. 3, 07-940-03). Without XRP spectroscopy, it was concluded that it was Elgiloy (cobalt-chromium alloy) because it was the company's only product 35 years ago, at the time of original implantation. There was no severe damage or any corrosion of the clip [Figure
DISCUSSION
Published data on long-term morbidity and mortality of survivors of SAH are still limited. Long-term causes of death in survivors of SAH were largely unrelated to the SAH and were mainly other factors (mostly cancer and cardiovascular disease).[
Previous studies have used varying methods and criteria in studying and reporting long-term mortality rates of SAH survivors. The largest study to date reported that there were 13 lethal rebleeds from the clipped saccular intracranial aneurysms out of 1440 cases at the median times of 4.9 years.[
Even after operations performed by experienced neurosurgeons, neck remnants are found in nearly 10% of cases.[
Kashimura et al. emphasize that removal of previously placed clips is necessary when reoperation is performed for cerebral aneurysms that have reruptured a long time after their initial clipping.[
The first-generation Yasargil aneurysm clip was made in 1968 from implant steel with a half spring coil and no jaw guidance. The second-generation clip was introduced in 1970 with a 1.5 spring coil and safety ring to optimize closing force and stability. The Yasargil aneurysm clip made from Phynox increased magnetic resonance imaging safety again in 1983 (third-generation). The previous study demonstrated that the third-generation Yasargil aneurysm clips retain their mechanical properties and surface elemental composition in vivo for a long period.[
References
1. Huttunen T, von und Zu Fraunberg M, Koivisto T, Ronkainen A, Rinne J, Sankila R. Long-term excess mortality of 244 familial and 1502 sporadic one-year survivors of aneurysmal subarachnoid hemorrhage compared with a matched Eastern Finnish catchment population. Neurosurgery. 2011. 68: 20-7
2. Kashimura H, Ogasawara K, Kubo Y, Otawara Y, Ogawa A. Microsurgical removal of previously placed aneurysm clips and application of new clips for recurrent cerebral aneurysms. Technical note. J Neurosurg. 2007. 107: 881-3
3. Kivisaari RP, Porras M, Ohman J, Siironen J, Ishii K, Hernesniemi J. Routine cerebral angiography after surgery for saccular aneurysms: Is it worth it?. Neurosurgery. 2004. 55: 1015-24
4. Kossowsky R, Dujovny M, Kossovsky N, Keravel Y. Failure of a Heifetz aneurysm clip. J Neurosurg. 1982. 57: 233-9
5. Molyneux AJ, Birks J, Clarke A, Sneade M, Kerr RS. The durability of endovascular coiling versus neurosurgical clipping of ruptured cerebral aneurysms: 18 year follow-up of the UK cohort of the International Subarachnoid Aneurysm Trial (ISAT). Lancet. 2015. 385: 691-7
6. Otawara Y, Endo MM, Ogasawara K, Kubo Y, Ogawa A, Watanabe K. Reliability of cobalt-chromium alloy aneurysm clips after long-term implantations in patients with cerebral aneurysms. J Neurosurg. 2006. 105: 713-6
7. Otawara Y, Ogasawara K, Kubo Y, Kashimura H, Ogawa A, Watanabe K. Mechanical and surface properties of Yasargil Phynox aneurysm clips after long-term implantation in a patient with cerebral aneurysm. Neurosurg Rev. 2009. 32: 193-6
8. Servo A, Puranen M. Delayed breaking of a Heifetz aneurysm clip. Case report. J Neurosurg. 1977. 47: 463-5
9. Tsutsumi K, Ueki K, Usui M, Kwak S, Kirino T. Risk of recurrent subarachnoid hemorrhage after complete obliteration of cerebral aneurysms. Stroke. 1998. 29: 2511-3
10. Wermer MJ, Greebe P, Algra A, Rinkel GJ. Incidence of recurrent subarachnoid hemorrhage after clipping for ruptured intracranial aneurysms. Stroke. 2005. 36: 2394-9

