

- Department of Neurosurgery, Takeda General Hospital, Kyoto City, Kyoto, Japan.
Correspondence Address:
Masahiro Kawanishi, MD, PhD, Department of Neurosurgery, Takeda General Hospital, Kyoto City, Kyoto, Japan.
DOI:10.25259/SNI_606_2022
Copyright: © 2022 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, transform, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Masahiro Kawanishi, Hidekazu Tanaka, Yutaka Ito, Makoto Yamada, Kunio Yokoyama, Naokado Ikeda, Akira Sugie. Regression of retro-odontoid pseudotumor following botulinum injection into cervical muscles. 22-Jul-2022;13:321
How to cite this URL: Masahiro Kawanishi, Hidekazu Tanaka, Yutaka Ito, Makoto Yamada, Kunio Yokoyama, Naokado Ikeda, Akira Sugie. Regression of retro-odontoid pseudotumor following botulinum injection into cervical muscles. 22-Jul-2022;13:321. Available from: https://surgicalneurologyint.com/surgicalint-articles/11729/
Date of Submission
07-Jul-2022
Date of Acceptance
10-Jul-2022
Date of Web Publication
22-Jul-2022
Abstract
Background: Posterior fixation of C1/2 has become more commonly performed to treat retro-odontoid pseudotumor (ROP). Here, we report a 60-year-old female with cervical dystonia (CD), whose ROP regressed and whose quadriparesis improved after a series of cervical intramuscular botulinum injections.
Case Description: A 60-year-old female with 30 years of CD newly presented with a progressive quadriparesis. When the MRI showed ROP compression the cervical spinal cord, she refused surgery and underwent multiple cervical muscular botulinum injections over the next 2 years. Following these injections, the patient’s quadriparesis improved as the ROP regressed on subsequent MR studies.
Conclusion: Over a 2-year period, multiple cervical botulinum injections caused regression of a retro-odontoid cervical pseudotumor improvement in the patient’s quadriparesis.
Keywords: Botulinum, Regression, Cervical dystonia, Retro-odontoid pseudotumor
INTRODUCTION
Retro-odontoid pseudotumor (ROP) is a nonneoplastic mass that forms behind the dentate ligament located dorsal to the axial vertebrae. Posterior fusion is the typical treatment of choice for ROP-related atlantoaxial instability (AAI). Here, a 60-year-old female with 30 years’ duration of cervical dystonia (CD) newly developed a progressive quadriparesis attributed to ROP that markedly improved following repeated botulinum injections over a 2-year period.
CASE REPORT
Clinical presentation
A 60-year-old female, with CD for 30 years’ duration, newly presented over the past 2 years with a progressive quadriparesis. On neurological examination, she was quadriparetic, exhibiting right more than left clumsiness of the hands and a spastic lower extremity paresis.
MR examination and botulinum injections
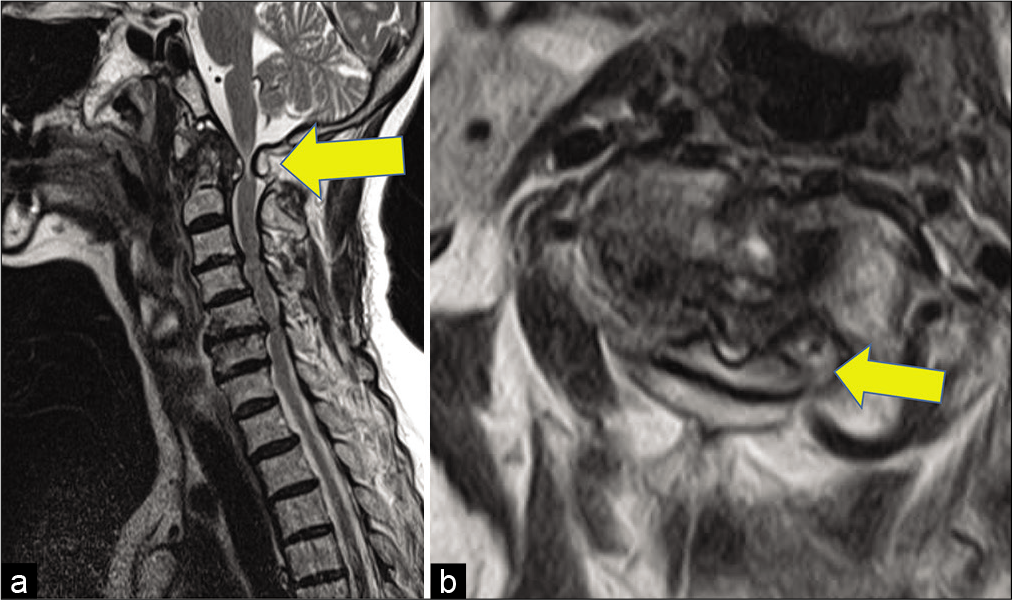
The cervical MR showed a low-intensity mass behind the odontoid process that compressed the cervical spinal cord and resulted in a high intrinsic cord signal [
DISCUSSION
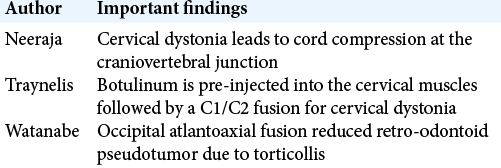
Acquired CD usually occurs between the ages of 20 and 60. It often leads to progressive cervical spinal degeneration most typically involving the C5/6 level. Interestingly, it rarely occurs above C2, and when it is present, which is seen in conjunction with AAI and myelopathy. Neeraja et al. reported that long-standing CD can lead to cord compression at the craniovertebral junction and result in myelopathy [
Posterior surgery for ROP
In general, posterior fixation of C1/2 has generally is typically required to treat ROP with AAI.[
CONCLUSION
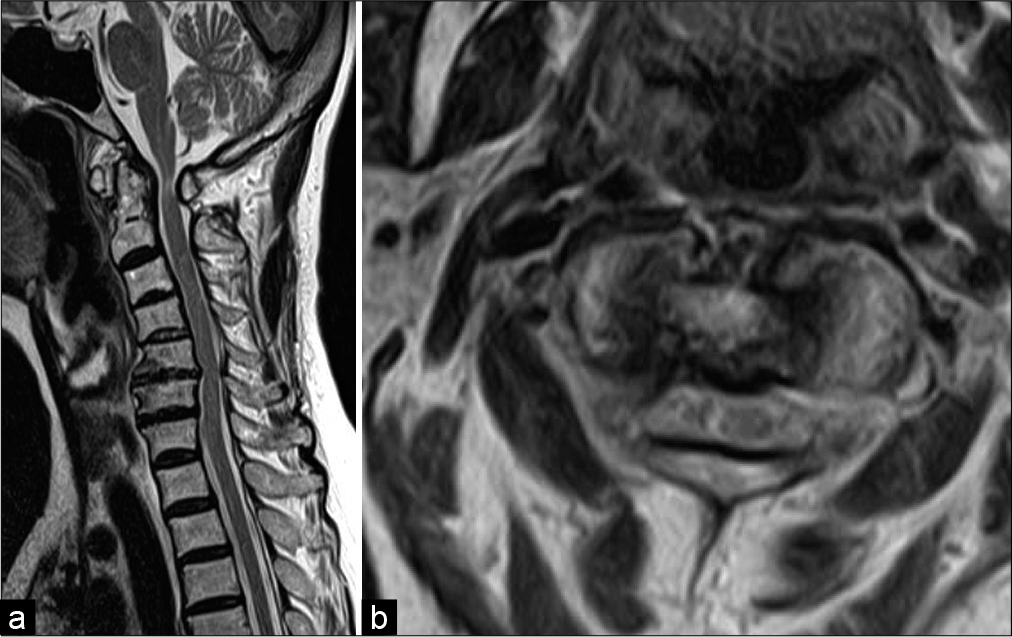
In a 60-year-old female, repeated intramuscular cervical botulinum injections over a 2-year period caused regression of ROP. This results in improvement of her quadriparesis in proportion to progressive resolution of her cord compression and high cord signal.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Goel A, Darji H, Shah A, Prasad A, Hawaldar A. Retroodontoid and retro-C2 body pseudotumor, pannus, and/or cyst. A study based on analysis of 63 cases. World Neurosurg. 2021. 151: e170-7
2. Nakazawa T, Inoue G, Imura T, Miyagi M, Saito W, Shirasawa E. Regression of retro-odontoid pseudotumor using external orthosis without atlantoaxial fusion: A case report. JBJS Case Connect. 2019. 9: e0329
3. Neeraja K, Prasad S, Surisetti BK, Holla VV, Sharma D, Kamble N. Cervical myeloradiculopathy and atlantoaxial instability in cervical dystonia. World Neurosurg. 2021. 146: e1287-92
4. Traynelis VC, Ryken T, Rodnitzky RL, Menezes AH. Botulinum toxin enhancement of postoperative immobilization in patients with cervical dystonia. Technical note. J Neurosurg. 1992. 77: 808-9
5. Watanabe M, Iwashina T, Sakai D, Yamamoto Y, Mochida J. Cervical myelopathy with retroodontoid pseudotumor caused by atlantoaxial rotatory fixation and senile tremor. Tokai J Exp Clin Med. 2009. 34: 39-41

