

- Department of Neurosurgery, University of Iowa, 200 Hawkins Drive, Iowa City, IA, United States.
DOI:10.25259/SNI_829_2020
Copyright: © 2021 Surgical Neurology International This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.How to cite this article: Colin Gold, Scott Seaman, Satoshi Yamaguchi. Relationship between odontoid fracture angle and cervical sagittal balance. 14-Apr-2021;12:157
How to cite this URL: Colin Gold, Scott Seaman, Satoshi Yamaguchi. Relationship between odontoid fracture angle and cervical sagittal balance. 14-Apr-2021;12:157. Available from: https://surgicalneurologyint.com/?post_type=surgicalint_articles&p=10715
Date of Submission
17-Nov-2020
Date of Acceptance
13-Mar-2021
Date of Web Publication
14-Apr-2021
Abstract
Background: Fractures can occur in various locations within the odontoid process with differing orientations. However, little is known about what factors contribute to the anterior versus posterior angles/orientation of these fractures.
Methods: We evaluated 74 patients with odontoid fractures (2013–2018) from a single-institution. Patients’ fracture angles/orientations were measured on computed tomography studies, and were grouped into oblique posterior (OP) or oblique anterior (OA) groups. We also took into account cervical sagittal balance utilizing upright x-rays. Other variables studied included patients’ ages, sagittal balance measurements, and the mechanisms of injury.
Results: Fracture angles were significantly steeper in the OP group. OP fractures had larger C2-C7 sagittal vertical axis, occiput-C2 angles, and occiput-C7 angles versus anteriorly oriented fractures. In our linear regression model, advanced age and large occiput-C2 angles were predictive of the odontoid fracture angle. Patients who sustained ground-level falls also had significantly steeper fracture angles versus those involved in motor vehicle accidents.
Conclusion: The odontoid tends to fracture at a steep, posterior angle in elderly patients who demonstrate a large positive sagittal balance when the head is extended following a ground-level falls.
Keywords: Angulation, Cervical spine, Dens, Fracture, Odontoid, Sagittal balance
INTRODUCTION
Odontoid fractures are common cervical spine traumatic fractures and there is no clear agreement regarding the optimal management strategy.[
MATERIALS AND METHODS
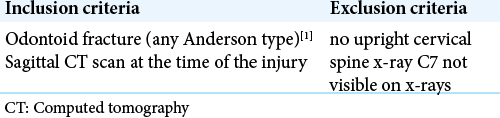
This study was performed with institutional review board approval, utilizing multiple inclusion/ exclusion criteria [
Clinical data
Patients with odontoid fractures averaged 76 years of age (2013–2018). The Anderson fracture types/odontoid fracture angles were measured utilizing computed tomography (CT) scans, while cervical sagittal balance was based upon standing/sitting cervical spine X-rays [
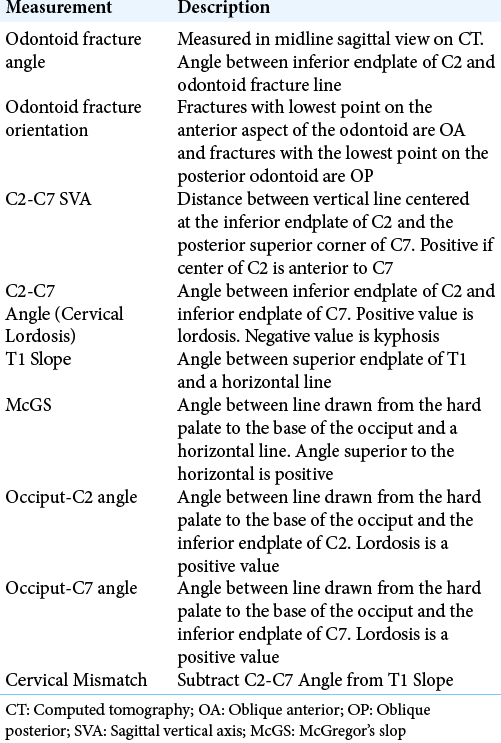
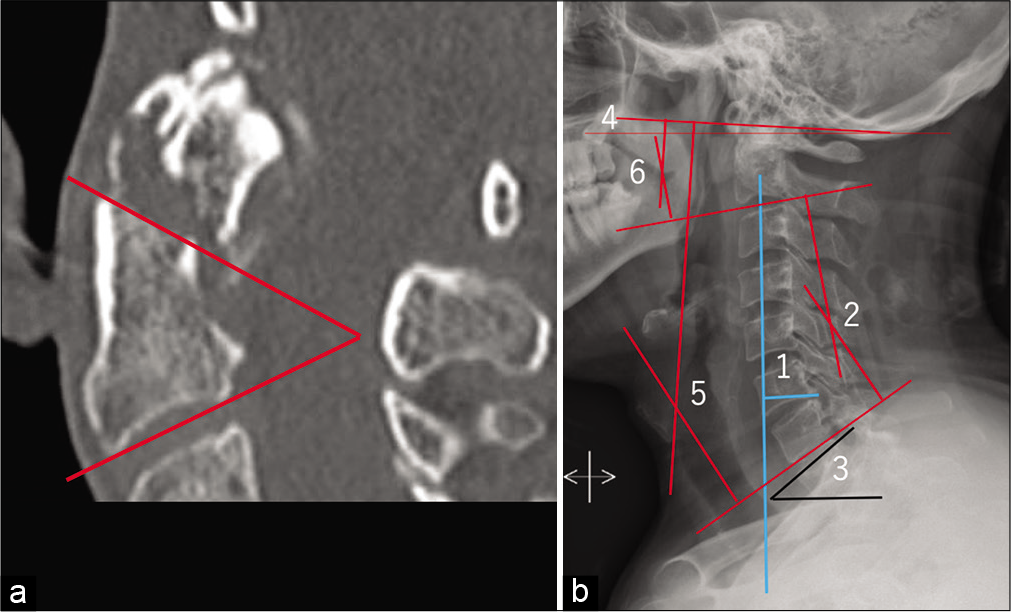
Figure 1:
(a) Mid-sagittal computed tomography (CT) demonstrating odontoid fracture angle measurement. (b) Cervical sagittal balance measurements key. (1). C2-C7 sagittal vertical axis (SVA), (2). C2-C7 angle (cervical lordosis), (3). T1 slope, (4). McGregor’s slope (McGS), (5). Occipitut-C7 angle, (6). Occiput-C2 angle.
Statistical analysis
All statistical analysis was performed using SPSS (SPSS Inc., IBM, Chicago, IL), independent samples t-tests, linear regression models, one-way ANOVA of the multiple variables under consideration.
RESULTS
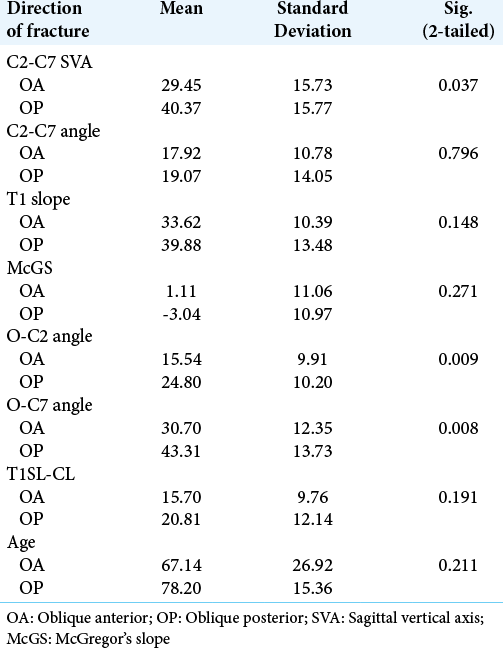
The odontoid fracture angles were significantly steeper for posterior versus anterior fractures (40.57 vs. 17.03, P = 0.000). There were also significant differences in C2-C7 SVA, O-C2 angle, and O-C7 angle between oblique anterior (OA) versus oblique posterior (OP) fractures [
DISCUSSION
Our measures of cervical sagittal balance determined the anterior versus posterior dens fracture angulation (e.g. C2- C7 SVA, O-C2 angle, and O-C7 angle). A more positive C2-C7 SVA and larger O-C2 and O-C7 angles were associated with posteriorly oriented fractures.
The most severely angulated odontoid fractures were associated with ground-level falls (e.g. significantly greater (40.23°), and falls from a height (35.81°) versus MVAs (18.45°). This finding is an agreement with those of Blizzard et al. 2017, in which the authors found that the two most significant measurements in predicting dens fracture angle were anteroposterior sagittal balance and lower cervical disc inclination levels.[
Our linear regression analysis predicted dens fracture angles with an R2 value of 0.21 using O-C2 angle and age.
CONCLUSION
This study showed that the orientation of the occiput relative to the dens and subaxial cervical spine largely predicted the dens fracture angle and orientation. Posteriorly-oriented odontoid fractures were associated with large C2-C7 SVAs, O-C2 angles, and O-C7 angles, while advanced age and large O-C2 angles were predictors of steep fracture angles [

Declaration of patient consent
Institutional Review Board (IRB) permission obtained for the study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
1. Anderson LD, D’Alonzo RT. Fractures of the odontoid process of the axis. J Bone Joint Surg. 1974. 56: 1663-74
2. Blizzard SR, Krishnamoorthy B, Shinseki M, Betsch M, Yoo J. The magnitude of angular and translational displacement of dens fractures is dependent on the sagittal alignment of the cervical spine rather than the force of injury. Spine J. 2017. 17: 1859-65
3. Charles YP, Ntilikina Y, Blondel B, Fuentes S, Allia J, Bronsard N. Mortality, complication, and fusion rates of patients with odontoid fracture: The impact of age and comorbidities in 204 cases. Arch Orthop Trauma Surg. 2019. 139: 43-51
4. Pal D, Sell P, Grevitt M. Type II odontoid fractures in the elderly: An evidence-based narrative review of management. Eur Spine J. 2011. 20: 195-204
5. Reinhold M, Bellabarba C, Bransford R, Chapman J, Krengel W, Lee M. Radiographic analysis of type II odontoid fractures in a geriatric patient population: Description and pathomechanism of the “Geier”-deformity. Eur Spine J. 2011. 20: 1928-39
6. Ryan MD, Henderson JJ. The epidemiology of fractures and fracture-dislocations of the cervical spine Injury. 1992. 23: 38-40

